Herpes: Multiple small, discrete, punched-out ulcers on background of normal mucosa
CMV and HIV: 1 or more large, flat ulcers
HPV: Multiple papillary excrescences
EBV: Deep, linear ulcers
TOP DIFFERENTIAL DIAGNOSES
• Candida, reflux, or drug-induced esophagitis
PATHOLOGY
• Impaired immune surveillance: Radiation and chemotherapy render esophageal mucosa vulnerable to infection
CLINICAL ISSUES
• Odynophagia is most common presenting symptom
• Herpes: Usually in immunocompromised patients but can occur in otherwise healthy patients
Especially in sexual partners of patients with active herpes infection
• Treatment
Analgesics for odynophagia
Antiviral therapy for CMV, VZV, and persistent herpes
DIAGNOSTIC CHECKLIST
• Small discrete, or large shallow ulcers should suggest viral esophagitis in immunocompromised patients with odynophagia
• Careful analysis of double-contrast patterns is necessary to distinguish plaques from ulcers
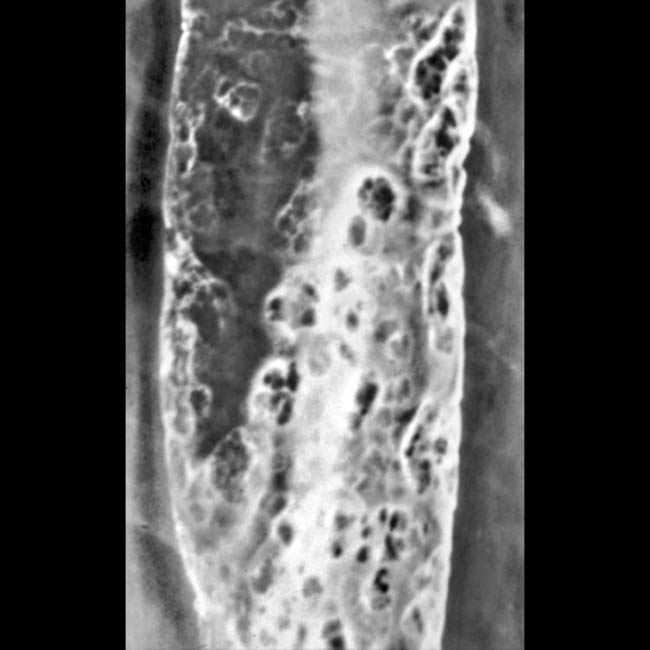
(Left) Spot film from esophagram shows tiny ulcers surrounded by a radiolucent halo of edematous mucosa in a patient with herpes esophagitis. Ulcers are seen en face and in profile .
(Right) Double-contrast esophagram shows elongated plaques in a patient with herpes esophagitis. The findings are indistinguishable from Candida esophagitis.
(Left) Barium esophagram film demonstrates at least 1 large superficial ulcer in this biopsy-proven HIV-induced ulceration. Giant superficial esophageal ulcers are usually caused by cytomegalovirus or HIV in the setting of AIDS.
(Right) Double-contrast esophagram film shows clusters of nodules due to a human papillomavirus infection, findings typical of squamous papillomatosis.







 and in profile
and in profile  .
.
 in a patient with herpes esophagitis. The findings are indistinguishable from Candida esophagitis.
in a patient with herpes esophagitis. The findings are indistinguishable from Candida esophagitis.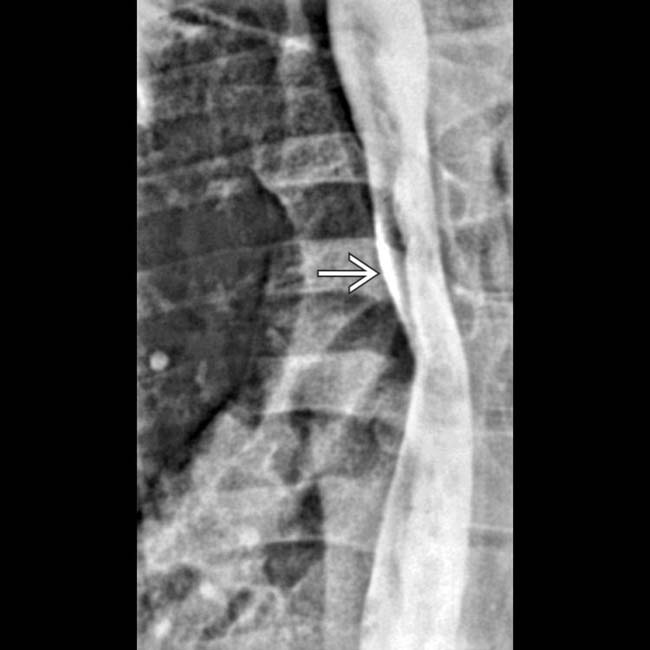
 in this biopsy-proven HIV-induced ulceration. Giant superficial esophageal ulcers are usually caused by cytomegalovirus or HIV in the setting of AIDS.
in this biopsy-proven HIV-induced ulceration. Giant superficial esophageal ulcers are usually caused by cytomegalovirus or HIV in the setting of AIDS.