Accounts for 5-15% of colonic adenomas




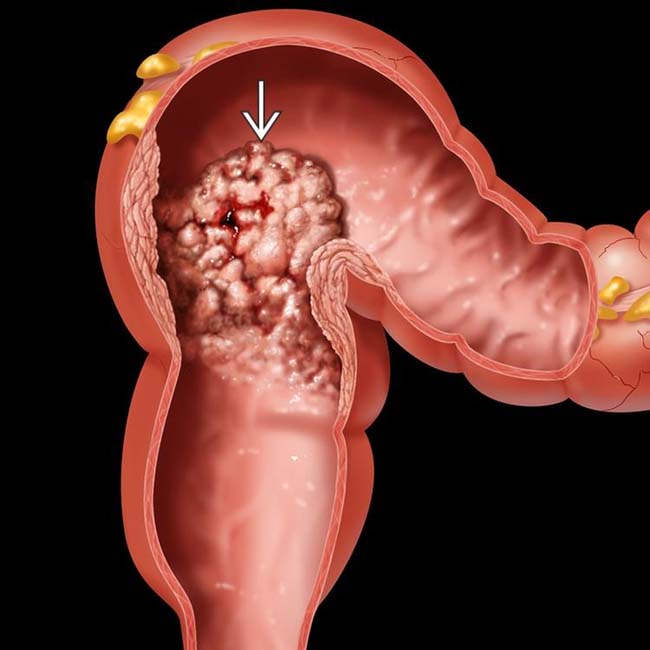
 in the rectosigmoid colon having a shaggy, nodular surface, sometimes likened to the surface of a cauliflower.
in the rectosigmoid colon having a shaggy, nodular surface, sometimes likened to the surface of a cauliflower.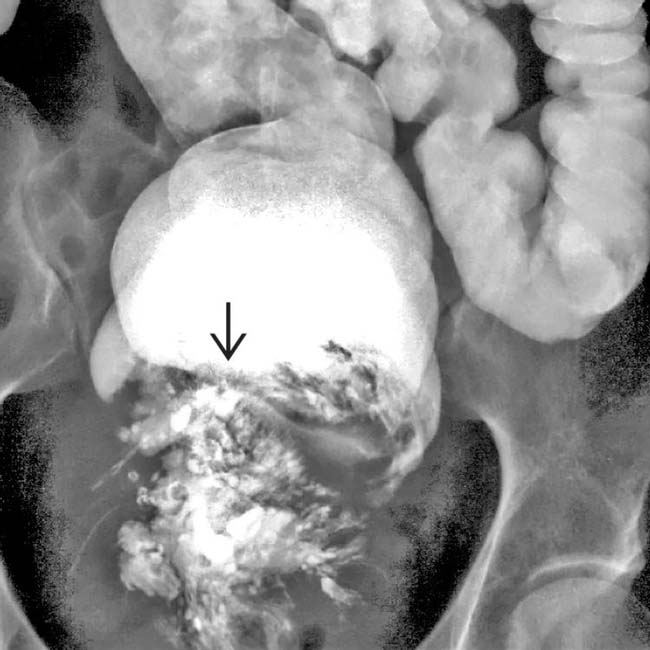
 with a frond-like surface. Note the absence of a colonic obstruction, a typical feature of this soft and compressible tumor.
with a frond-like surface. Note the absence of a colonic obstruction, a typical feature of this soft and compressible tumor.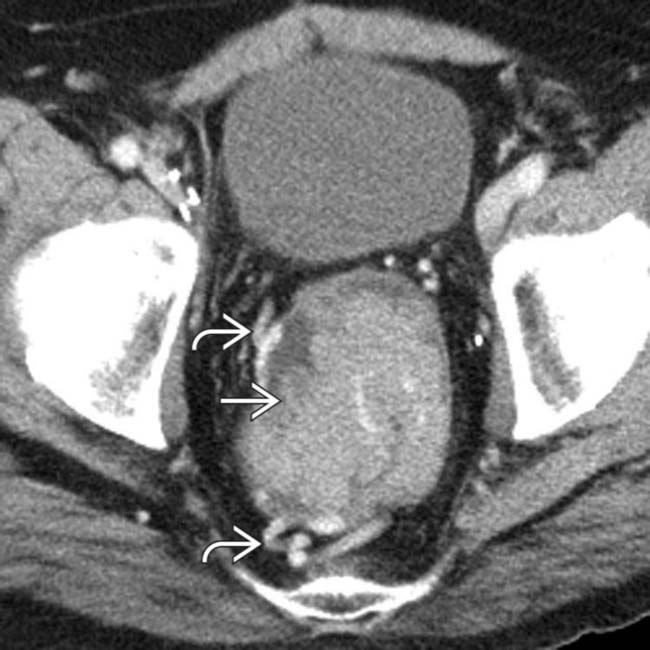
 that fills the rectum. Note large vessels
that fills the rectum. Note large vessels  within and draining the mass.
within and draining the mass.
 , but no definite signs of invasion through the rectal wall and no metastases. The resected villous adenoma had foci of frank carcinoma.
, but no definite signs of invasion through the rectal wall and no metastases. The resected villous adenoma had foci of frank carcinoma.IMAGING
General Features









Radiographic Findings















































 in the cecum, a typical appearance of a villous adenoma.
in the cecum, a typical appearance of a villous adenoma.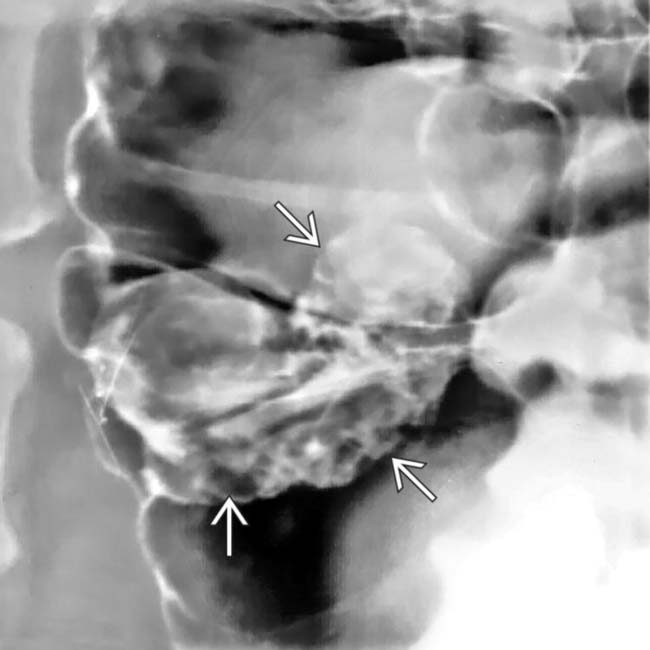
 coated with barium and outlined by air on this view.
coated with barium and outlined by air on this view.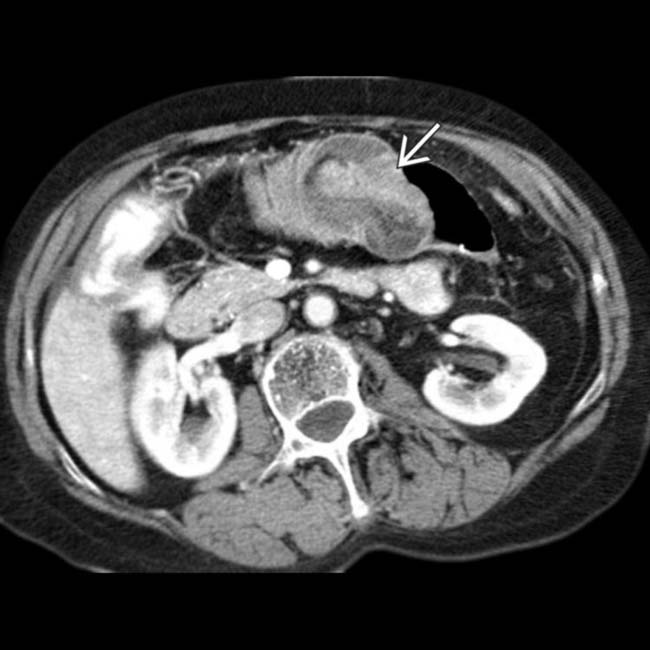
 .
.
 , a villous adenoma, as the lead point of the colonic intussusception.
, a villous adenoma, as the lead point of the colonic intussusception.
 that proved to be a 2nd villous adenoma.
that proved to be a 2nd villous adenoma.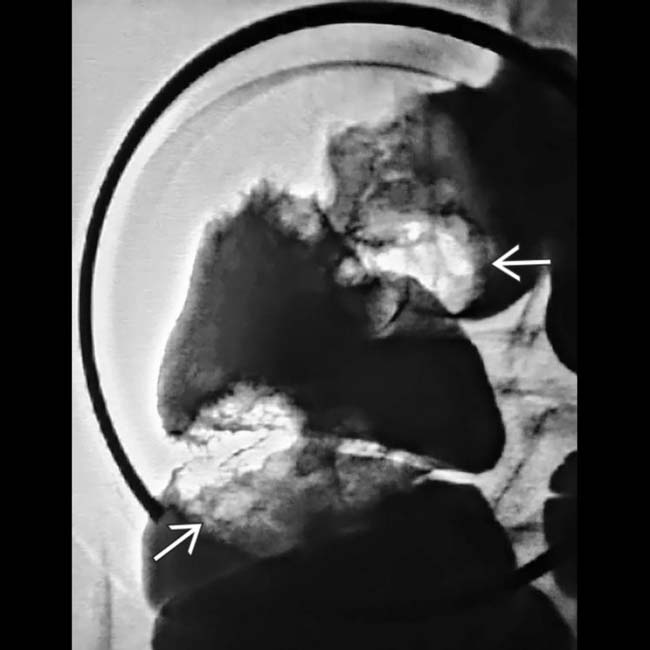
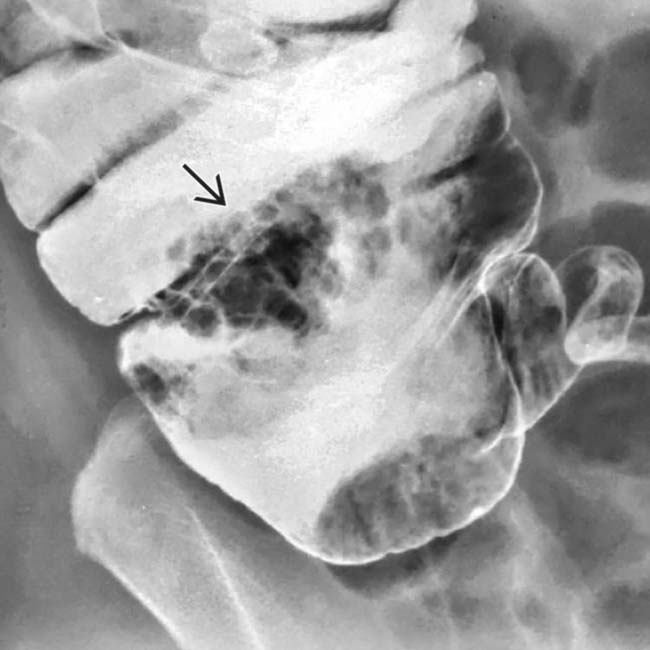
 seen as masses with irregular surface contours within the barium pool. A right hemicolectomy and histopathology confirmed the diagnosis.
seen as masses with irregular surface contours within the barium pool. A right hemicolectomy and histopathology confirmed the diagnosis.
 in the rectosigmoid colon with a very nodular surface. Barium within the rectum is diluted by mucus secreted by the tumor.
in the rectosigmoid colon with a very nodular surface. Barium within the rectum is diluted by mucus secreted by the tumor.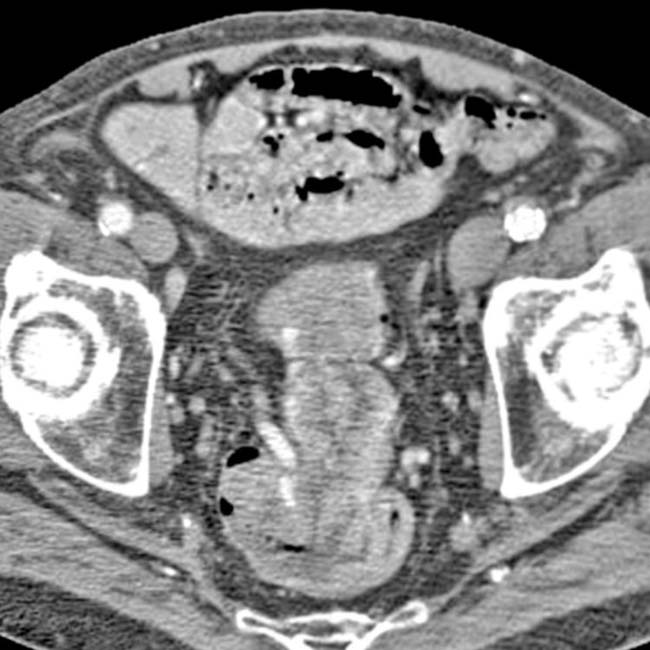

 within the rectum.
within the rectum.


