[level-membership-for-cardiovascular-category]
CHAPTER 39 Vascular Rings and Slings
Vascular rings and slings refer to a spectrum of arterial anomalies caused by abnormalities in development of the embryonic aortic arches.1–4 Complications arise from compression of the trachea, esophagus, or both, leading to respiratory distress and dysphagia. The vast majority of rings and slings are found in infants and young children, but the anomalies can be seen in adults. Computed tomography (CT) and magnetic resonance imaging (MRI) provide accurate anatomic delineation of the vascular anomalies and compressed structures and are the imaging studies of choice to establish the diagnosis. Treatment is surgical intervention for symptomatic patients.
Prevalence and Epidemiology
Vascular rings and slings represent approximately 1% of congenital cardiovascular anomalies,3 although this incidence may be underestimated because some lesions are asymptomatic. Most cases are sporadic, but there may be a genetic inheritance in some arch anomalies. Microdeletions of chromosome 22q11, in particular, have been associated with various arch anomalies.5
Etiology and Pathophysiology
Persistence of a segment of arch that should have regressed or regression of a segment that should have normally persisted explains the development of most arch anomalies. The theoretic embryonic double aortic arch model proposed by Edwards is most extensively used to demonstrate embryologic explanations for the variations in arch development.6 This model classifies vascular rings by the side of the ductus arteriosus and the site of dissolution of the double arches (Fig. 39-1).
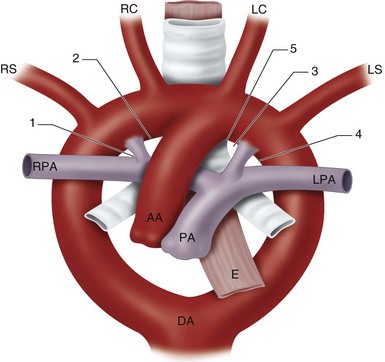
 FIGURE 39-1
FIGURE 39-1Vascular rings may be complete (true) or incomplete (Fig. 39-2).3 In complete rings, the vascular structures entirely surround and compress the trachea and esophagus. These include the double aortic arch and right arch with aberrant retroesophageal left subclavian artery. In the double arch, an atretic segment of arch may complete the ring. With an aberrant left subclavian, a left ligamentum arteriosum connects the descending aorta and left pulmonary artery completing the ring.
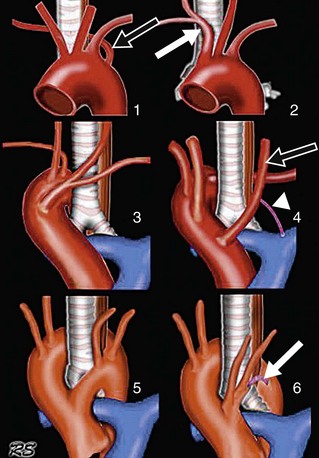
 FIGURE 39-2
FIGURE 39-2In incomplete rings, the vascular anomalies do not entirely encircle the trachea and esophagus, but do cause mass effect on these structures. These include the left arch with aberrant right subclavian artery and anomalous innominate artery.3 In the case of an aberrant right subclavian, the vessel itself or an aortic diverticulum (Kommerell diverticulum) at the takeoff of the artery compresses the posterior aspect of the esophagus. In anomalous innominate artery, the right innominate artery arises too far to the left from the arch and compresses the trachea anteriorly as it crosses the midline.
MANIFESTATIONS
Clinical Presentation
Symptoms vary with the tightness of the ring around the trachea and/or esophagus, and hence the degree of tracheobronchial compression. Tight rings usually manifest in neonates or infants. Symptoms include stridor, cough, repeated pulmonary infections, cyanosis, and respiratory failure, and feeding difficulties.1–4 Looser rings may be discovered in older children or adults in whom mild dysphagia or choking on food prompts evaluation. Some asymptomatic rings will be discovered incidentally during an imaging study performed for other clinical indications. Rings that are asymptomatic early in life can become symptomatic later in life if the vascular structures become ectatic and compress the airway or esophagus.2 Double aortic arches tend have more severe symptoms and present earlier than other rings.7 Slings commonly manifest in neonates, producing respiratory compromise.
Imaging Studies
Techniques and Findings
Radiography
Chest radiography is used to show the side of the aortic arch and compression of adjacent structures. If a right arch is identified, the likelihood of a vascular ring is high. If only a left arch is identified, a vascular ring is less likely, but not excluded.2,8
Computed Tomography
Computed tomography can provide accurate anatomic detail of the vascular anomalies and compressed trachea or esophagus. CT is especially useful for the evaluation of the tracheobronchial tree, simulating the surgical view.1
CT is performed using thin collimation (<1 mm), large pitch (<1.5), rapid scan time, and a single breath-hold, when possible. In adolescents and adults, contrast medium is injected via a power injector at a high flow rate of 3 to 4 mL/sec using a contrast volume of 100 to 150 mL (280 to 320 mg I/mL). Scan delay time is determined with an automatic bolus tracking system. The cursor is placed over the ascending aorta if aortic anomalies are suspected and over the main pulmonary artery if pulmonary sling is suspected. Electrocardiographic (ECG) gating is not needed. The volumetric data are reconstructed at a 3- to 5-mm slice thickness for routine viewing and at a 1- to 2-mm slice thickness for multiplanar reformatting and three-dimensional reconstructions. A standard reconstruction algorithm is used for reconstruction.9–11 (See Chapter 38, Coarctation of the Aorta, for pediatric techniques.)
Classic Signs
Double Aortic Arch
Chest radiographic findings include opacities lying on both sides of the tracheal air column, proximal tracheal indentation, and posterior esophageal indentation (Fig. 39-3). CT and MRI show the two arches arising from a single ascending aorta, with each arch giving rise to a subclavian and carotid artery before joining to form a single descending aorta, usually left-sided (Fig. 39-4).1-4,12-16 The right arch is commonly larger and more cephalad than the left arch. In rare cases, one limb, often the left, is atretic, with a fibrous band completing the ring (Fig. 39-5).17

 FIGURE 39-3
FIGURE 39-3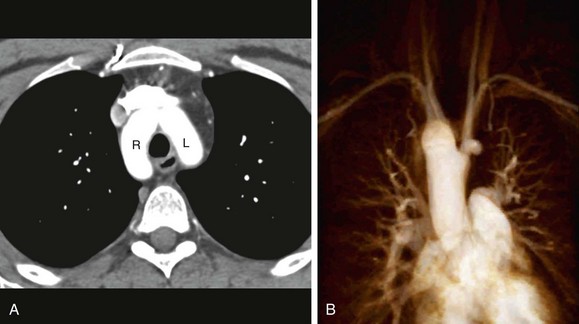
 FIGURE 39-4
FIGURE 39-4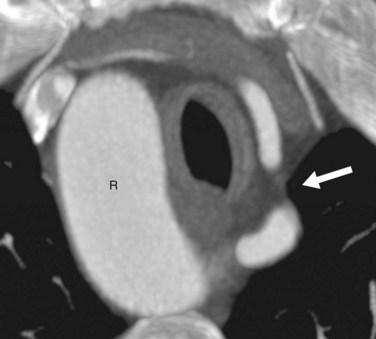
 FIGURE 39-5
FIGURE 39-5Right Aortic Arch with Aberrant Left Subclavian Artery
Chest radiographic findings include right-sided paratracheal opacity and tracheal indentation, posterior esophageal indentation, and absence of a normal left-sided aortic arch shadow (Fig. 39-6). CT and MRI findings are a right arch and left subclavian artery arising from the posterior aspect of the right arch (Fig. 39-7). A Kommerell diverticulum at the origin of the left subclavian artery from the aorta may be seen.1-4,12-16

 FIGURE 39-6
FIGURE 39-6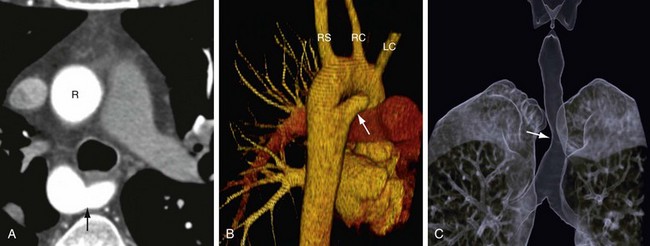
 FIGURE 39-7
FIGURE 39-7Left Aortic Arch with Aberrant Right Subclavian Artery
This is an arch anomaly but not a vascular ring. A frontal chest radiograph may show an abnormal mediastinal contour at the level of the aortic arch, representing dilation of the origin of the aberrant artery (i.e., diverticulum of Kommerell; Fig. 39-8). A lateral chest radiograph can show posterior esophageal indentation. CT and MRI can confirm the diagnosis of anomalous origin of the right subclavian artery, which arises as the last branch off the aorta, rather than the first.1-4,12-16 A Kommerell diverticulum and esophageal compression are other findings. Atherosclerotic changes and intramural thrombus formation can occur within this diverticulum (Fig. 39-9).
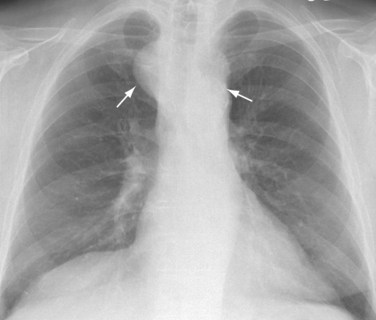
 FIGURE 39-8
FIGURE 39-8
 FIGURE 39-9
FIGURE 39-9Innominate Artery Compression
Chest radiographic CT and MRI findings are anterior compression of the trachea.1-4,12-16,18 The site of compression is usually at or just below the thoracic inlet (Fig. 39-10).
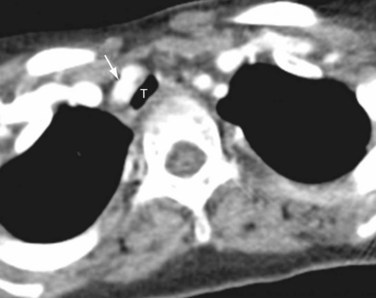
 FIGURE 39-10
FIGURE 39-10Anomalous Left Pulmonary Artery (Pulmonary Sling)
Chest radiographic findings include right-sided tracheal indentation and often hyperinflation of the right middle and lower lobes. CT and MRI show the left pulmonary artery arising from the right pulmonary artery, coursing over the right main bronchus, and crossing between the trachea and esophagus to reach the left hilum (Fig. 39-11).1-4,12-16,19-21 When there are associated cartilaginous rings, long segment tracheal narrowing and a horizontal course of the main bronchi (i.e., T-shaped carina) will be noted.22
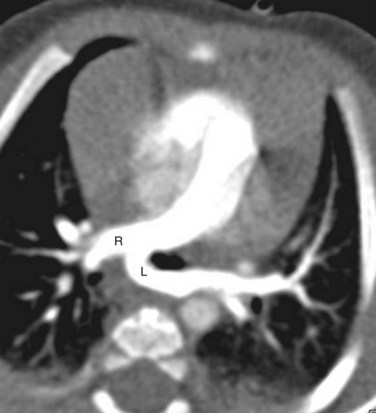
 FIGURE 39-11
FIGURE 39-11SYNOPSIS OF TREATMENT OPTIONS
Surgical and Interventional
Surgical repair is performed for symptomatic patients. Others are treated conservatively.







Berdon WE. Rings, slings, and other things: vascular compression of the infant trachea updated from the mid-century to the millennium—the legacy of Robert E. Gross, MD, and Edward B.D. Neuhauser, MD. Radiology. 2000;216:624-632.
Goo HW, Park I-S, Ko JK, et al. CT of congenital heart disease: normal anatomy and typical pathologic conditions. Radiographics. 2003;23:S147-S165.
Hernanz-Schulman M. Vascular rings: a practical approach to imaging diagnosis. Pediatr Radiol. 2005;35:961-979.
ED Lee, Siegel MJ, Hildebolt CF, et al. Multidetector CT evaluation of pediatric thoracic aortic anomalies: comparison of axial, multiplanar, and three-dimensional images. AJR Am J Roentgenol. 2004;182:777-784.
Oddone M, Granata C, Vercellino N, et al. Multi-modality evaluation of the abnormalities of the aortic arches in children: techniques and imaging spectrum with emphasis on MRI. Pedatric Radiol. 2005;35:947-960.
Predey TS, McDonald V, Demos TC, Moncada R. CT of congenital anomalies of the aortic arch. Semin Roentgenol. 1989;14:96-111.
1 Abrams D, Gerlis L, Daubeney P. Tracheoesophageal compression in congenital heart disease: vascular rings, pulmonary slings and other vascular abnormalities. In: Gatzoulis MA, Webb GD, Daubeney PEF, editors. Adult Congenital Heart Disease. Edinburgh: Churchill Livingstone; 2003:273-280.
2 Hernanz-Schulman M. Vascular rings: a practical approach to imaging diagnosis. Pediatr Radiol.. 2005;35:961-979.
3 Park MK. Vascular ring. In: Park MK, editor. Pediatric Cardiology for Practitioners. 5th ed. St. Louis: Mosby; 2008:303-308.
4 Weinberg PM. Aortic arch anomalies. In: Alan HD, Gutgesell HP, Clark EB, Driscoll DJ, editors. Heart Disease in Infants, Children, and Adolescents. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006:707-735.
5 Momma K, Matsuoka R, Takao A. Aortic arch anomalies associated with chromosome 22q11 deletion (CATCH 22). Pediatr Cardiol. 1999;20:97-102.
6 Edwards JE. Anomalies of the derivatives of the aortic arch system. Med Clin North Am. 1948;32:925-949.
7 Van Son JA, Julsrud PR, Hagler DJ, et al. Surgical treatment of vascular rings: the Mayo clinic experience. Mayo Clin Proc. 1993;68:1056-1063.
8 Pickhardt P, Siegel M, Gutierrez F. Vascular rings in symptomatic children: frequency of chest radiographic findings. Radiology. 1997;203:423-426.
9 Gilkeson RC, Ciancibello L, Zahka K. Multidetector CT evaluation of congenital heart disease in pediatric and adult patients. AJR. 2003;180:973-980.
10 Goo HW, Park I-S, Ko JK, et al. CT of congenital heart disease: normal anatomy and typical pathologic conditions. Radiographics. 2003;23:S147-S165.
11 Ed Lee, Siegel MJ, Hildebolt CF, et al. Multidetector CT evaluation of pediatric thoracic aortic anomalies: comparison of axial, multiplanar, and three-dimensional images. AJR. 2004;182:777-784.
12 Oddone M, Granata C, Vercellino N, et al. Multi-modality evaluation of the abnormalities of the aortic arches in children: techniques and imaging spectrum with emphasis on MRI. Pedatric Radiol. 2005;35:947-960.
13 Predey TS, McDonald V, Demos TC, Moncada R. CT of congenital anomalies of the aortic arch. Semin Roentgenol. 1989;14:96-111.
14 Remy-Jardin M, Remy J, Mayo JR, et al. Thoracic aorta. In: Remy-Jardin M, Remy J, Mayo JR, et al, editors. CT Angiography of the Chest. Philadelphia: Lippincott Williams & Wilkins; 2001:29-50.
15 Siegel MJ. Great vessels. In: Siegel MJ, editor. Pediatric Body CT. Philadelphia: Lippincott Williams & Wilkins; 2008:121-144.
16 Van Dyke CW, White RD. Congenital abnormalities of the thoracic aorta presenting in the adult. J Thorac Imaging. 1994;9:230-245.
17 Schlessinger AE, Krishnamurthy R, Sena LM, et al. Incomplete double aortic arch with atresia of the distal left arch: distinctive imaging appearance. AJR. 2005;184:1634-1639.
18 Adler SC, Isaacson G, Balsara RK. Innominate artery compression of the trachea: diagnosis and treatment by anterior suspension. A 25-year experience. Ann Otol Rhinol Laryngol. 1995;104:924-927.
19 Lee KH, Yoon CS, Choe KO, et al. Use of imaging for assessing anatomical relationships of tracheobronchial anomalies associated with left pulmonary artery sling. Pediatr Radiol. 2001;31:269-278.
20 Newman B, Meza MP, Towbin RB, Del Nido P. Left pulmonary artery sling: diagnosis and delineation of associated tracheobronchial anomalies with MR. Pediatr Radiol. 1996;26:661-668.
21 Park HS, Im JG, Jung JW, et al. Anomalous left pulmonary artery with complete cartilaginous ring. J Comput Assist Tomogr. 1997;21:478-480.
22 Berdon WE. Rings, slings, and other things: vascular compression of the infant trachea updated from the mid-century to the millennium—the legacy of Robert E. Gross, MD, and Edward B.D. Neuhauser, MD. Radiology. 2000;216:624-632.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
CHAPTER 39 Vascular Rings and Slings
Vascular rings and slings refer to a spectrum of arterial anomalies caused by abnormalities in development of the embryonic aortic arches.1–4 Complications arise from compression of the trachea, esophagus, or both, leading to respiratory distress and dysphagia. The vast majority of rings and slings are found in infants and young children, but the anomalies can be seen in adults. Computed tomography (CT) and magnetic resonance imaging (MRI) provide accurate anatomic delineation of the vascular anomalies and compressed structures and are the imaging studies of choice to establish the diagnosis. Treatment is surgical intervention for symptomatic patients.
Prevalence and Epidemiology
Vascular rings and slings represent approximately 1% of congenital cardiovascular anomalies,3 although this incidence may be underestimated because some lesions are asymptomatic. Most cases are sporadic, but there may be a genetic inheritance in some arch anomalies. Microdeletions of chromosome 22q11, in particular, have been associated with various arch anomalies.5
Etiology and Pathophysiology
Persistence of a segment of arch that should have regressed or regression of a segment that should have normally persisted explains the development of most arch anomalies. The theoretic embryonic double aortic arch model proposed by Edwards is most extensively used to demonstrate embryologic explanations for the variations in arch development.6 This model classifies vascular rings by the side of the ductus arteriosus and the site of dissolution of the double arches (Fig. 39-1).
Vascular rings may be complete (true) or incomplete (Fig. 39-2).3 In complete rings, the vascular structures entirely surround and compress the trachea and esophagus. These include the double aortic arch and right arch with aberrant retroesophageal left subclavian artery. In the double arch, an atretic segment of arch may complete the ring. With an aberrant left subclavian, a left ligamentum arteriosum connects the descending aorta and left pulmonary artery completing the ring.
In incomplete rings, the vascular anomalies do not entirely encircle the trachea and esophagus, but do cause mass effect on these structures. These include the left arch with aberrant right subclavian artery and anomalous innominate artery.3 In the case of an aberrant right subclavian, the vessel itself or an aortic diverticulum (Kommerell diverticulum) at the takeoff of the artery compresses the posterior aspect of the esophagus. In anomalous innominate artery, the right innominate artery arises too far to the left from the arch and compresses the trachea anteriorly as it crosses the midline.
MANIFESTATIONS
Clinical Presentation
Symptoms vary with the tightness of the ring around the trachea and/or esophagus, and hence the degree of tracheobronchial compression. Tight rings usually manifest in neonates or infants. Symptoms include stridor, cough, repeated pulmonary infections, cyanosis, and respiratory failure, and feeding difficulties.1–4 Looser rings may be discovered in older children or adults in whom mild dysphagia or choking on food prompts evaluation. Some asymptomatic rings will be discovered incidentally during an imaging study performed for other clinical indications. Rings that are asymptomatic early in life can become symptomatic later in life if the vascular structures become ectatic and compress the airway or esophagus.2 Double aortic arches tend have more severe symptoms and present earlier than other rings.7 Slings commonly manifest in neonates, producing respiratory compromise.
Imaging Studies
Techniques and Findings
Radiography
Chest radiography is used to show the side of the aortic arch and compression of adjacent structures. If a right arch is identified, the likelihood of a vascular ring is high. If only a left arch is identified, a vascular ring is less likely, but not excluded.2,8
Computed Tomography
Computed tomography can provide accurate anatomic detail of the vascular anomalies and compressed trachea or esophagus. CT is especially useful for the evaluation of the tracheobronchial tree, simulating the surgical view.1
[/not-level-membership-for-cardiovascular-category]
