Chapter 18 Use of the Transtibial Technique to Avoid Posterior Cruciate Ligament and Roof Impingement of an Anterior Cruciate Ligament Graft
Definition, Complications, and Diagnosis of Posterior Cruciate Ligament Impingement
PCL impingement occurs when the ACL graft wraps around the PCL as the knee is flexed. Impingement of the ACL graft around the PCL causes a tension rise in flexion that either limits flexion or stretches the ACL graft, resulting in anterior instability. Not widening the notch and malplacement of the ACL graft in the coronal plane cause PCL impingement in the transtibial technique.1–3
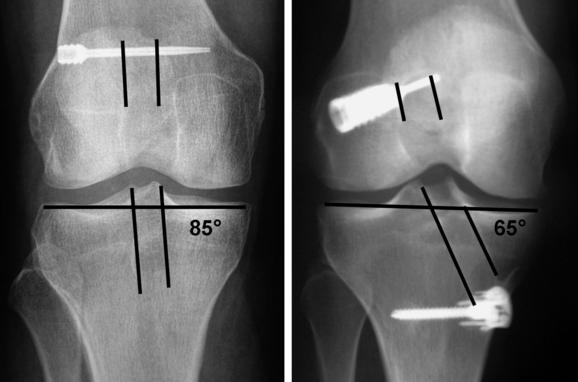
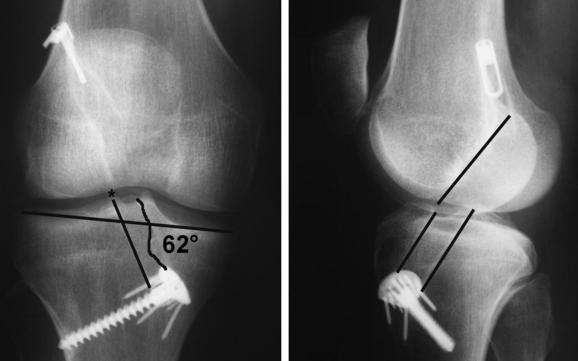
PCL impingement can be suspected if bone was not removed from the lateral femoral condyle (i.e., a wallplasty) until the space between the PCL and lateral femoral condyle exceeded the width of the ACL graft by 1 mm. An anteroposterior (AP) radiograph is diagnostic of PCL impingement when the tibial tunnel is at an angle greater than 70 degrees with respect to the medial joint line or when the lateral edge of the tibial tunnel is medial to the apex of the lateral tibial spine2 (Fig. 18-1). Magnetic resonance imaging (MRI) with three-dimensional (3D) reconstruction is diagnostic of PCL impingement when there is no space between the ACL graft and PCL or when the ACL graft does not run straight and is deformed by the PCL.1 Arthroscopy is diagnostic of PCL impingement when there is no space between the ACL graft and PCL at the apex of the notch and when the ACL graft is slack and bows laterally with the knee in 30 degrees of flexion.3 Surgeons who avoid PCL impingement will find that their patients have better knee flexion and better anterior and rotatory stability.1,2
Definition, Complications, and Diagnosis of Roof Impingement
Roof impingement occurs when the intercondylar roof contacts the ACL graft before the knee reaches full extension. Impingement of the ACL graft against the intercondylar roof causes either a loss of extension or a stretching out of the graft from abrasion, resulting in anterior instability. The cause of roof impingement is malplacement of the ACL graft in the sagittal plane. Placing the tibial tunnel anterior to the intercondylar roof with the knee in maximal extension causes roof impingement.4–7
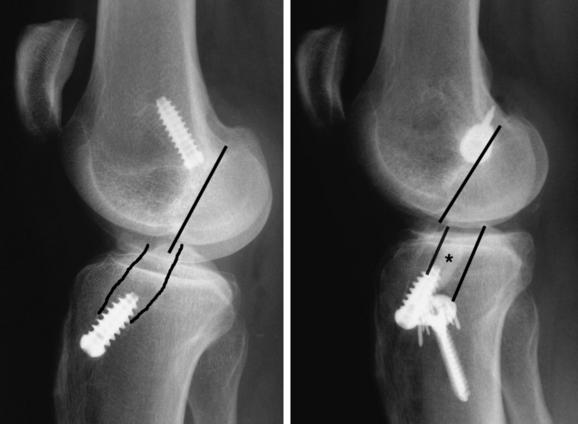
A lateral radiograph of the knee in maximal extension is diagnostic of roof impingement when the tibial tunnel is anterior to the intercondylar roof (Fig. 18-2). The lateral radiograph is less helpful in evaluating a bone–patellar tendon–bone graft than a soft tissue graft because the bone plug may obscure the wall and orientation of the tibial tunnel and because the tendon does not fill the bone tunnel.7 An MRI is diagnostic of roof impingement when the pathognomonic regionalized signal increase occurs in the graft, which is confined to the distal two-thirds of the ligament within the intercondylar notch. The portion of the ACL graft in the tibial and femoral tunnel and the portion of the graft that exits the femoral tunnel retain a low signal, which is identical to the PCL and patellar tendon.8–10 Arthroscopy is diagnostic of roof impingement when the ACL graft is frayed or a fibrous nodule is formed at the entrance of the tibial tunnel into the notch.11 Surgeons who avoid roof impingement will find that their patients have better knee extension and stability.7,12
The Tibial Tunnel: The Key Tunnel in the Transtibial Technique
The advantage of the transtibial technique is that when the notch is widened and the tibial tunnel is placed correctly in the coronal and sagittal plane, the correct placement of the femoral tunnel is automatic. The reason for this is that the position of the over-the-top femoral aimer and the position of the reamer are both controlled by the tibial tunnel.3 If the notch is not widened and the tibial tunnel is placed incorrectly in either the coronal or sagittal plane, then the femoral tunnel will be placed incorrectly and the patient will suffer from motion loss or instability.1,2,7
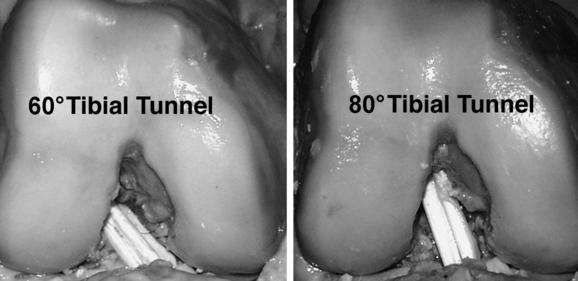
The feasibility of the transtibial technique to replicate the tension pattern of the intact ACL was determined by a cadaveric study that analyzed the effect of varying the angle of the tibial tunnel (and femoral tunnel) in the coronal plane on the tension pattern of the ACL graft (Fig. 18-3). Drilling the tibial tunnel at an angle of 60 degrees in the coronal plane placed the ACL graft far down the side wall of the notch away from the PCL, and the tension in the graft matched the intact ACL. Drilling the tibial tunnel at 70 and 80 degrees placed the ACL graft near the apex of the notch and the PCL, and the tension increase in the ACL graft with knee flexion was subsequently abolished by incremental excision of 2 to 6 mm of the lateral edge of the PCL. Therefore, the cause of the abnormal tension rise in flexion is the premature mechanical impingement of the ACL graft on the PCL during flexion and is avoided by placing the tibial tunnel at an angle less than 70 degrees.3
Rationale for Widening the Notch to Prevent Posterior Cruciate Ligament Impingement
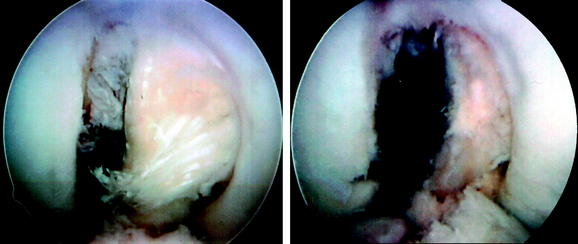
The surgeon must recognize that a soft tissue ACL graft is bigger than the intact ACL. Women of the same height and weight as men have significantly narrower notches, which means that women require more of a wallplasty than males for the same-diameter graft.13 An MRI study of the cross-section of the intercondylar notch has shown that the intact ACL is thin and elongated and fits snugly between the lateral edge of the PCL and the medial edge of the lateral femoral condyle.1 The use of a soft tissue ACL graft that is rounder and larger in a cross-sectional area than the intact ACL requires widening the notch until the space between the lateral femoral condyle and PCL exceeds the width of the graft by 1 mm. Arthroscopy has shown that the portion of the notch occupied by the PCL and intact ACL varies widely. Most notches are “PCL dominant,” in which the PCL occupies a larger cross-sectional area than the ACL (Fig. 18-4). Because surgeons prefer an ACL graft with a diameter of 8 to 10 mm, a wallplasty is required to make room for the larger ACL graft in almost every ACL reconstruction, especially in females.
Principle for Avoiding Posterior Cruciate Ligament and Roof Impingement
The principle for avoiding PCL and roof impingement is to widen the notch and correctly place the tibial tunnel in the coronal and sagittal planes (Fig. 18-5). In the coronal plane, the angle of the tibial tunnel should be 60 to 65 degrees with respect to the medial joint line of the tibia, and the lateral edge of the tibial tunnel should pass through the tip of the lateral spine.3 In the sagittal plane, the position of the tibial tunnel should be posterior and parallel to the intercondylar roof with the knee in extension, and the position should be customized based on variability in knee extension and roof angle so that a roofplasty is not required.6,14,15
Customized placement of the tibial tunnel in the sagittal plane is necessary because the sagittal depth of the insertion of the ACL is variable, the roof angle varies from 23 to 60 degrees, and knee extension varies from 5 to 15 degrees of hyperextension.14 The variability in the sagittal depth of the ACL insertion from 11 to 30 mm makes it a poor landmark for a point-and-shoot guide to select the position for an ACL graft with a diameter of 8, 9, or 10 mm.6 Customizing the placement of the tibial tunnel in the sagittal plane requires a tibial guide that registers the intercondylar roof with the knee in maximal hyperextension.16,17 The advantage of customizing the tibial tunnel is that roof impingement is avoided without a roofplasty, which has been shown to increase the graft tension at midrange of flexion and increase anterior laxity as the knee is flexed.15
Surgical Technique for Avoiding Posterior Cruciate Ligament and Roof Impingement and Replicating the Tension Pattern of the Intact Anterior Cruciate Ligament
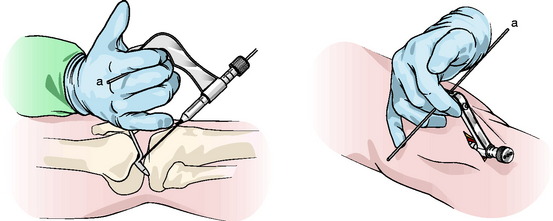
This surgical technique requires the use of a tibial guide that registers the intercondylar roof and a coronal alignment rod placed in the handle of the guide that allows the angle of the tibial tunnel in the coronal plane to be visually adjusted by the surgeon at the time of reconstruction (Howell 65°, Howell Tibial Guide, Arthrotek, Warsaw, IN)18 (Fig. 18-6). The use of a coronal alignment guide reduces the need for inoperative radiography to check the positioning of the tibial tunnel.
The initial arthroscopic examination of the notch should focus on removing the remnant of the torn ACL and clearly visualizing the lateral edge of the PCL. The tip of the guide, which is 9.5 mm wide, is passed between the PCL and the lateral femoral condyle. The knee is then gradually extended to examine whether enough space exists between the lateral femoral condyle and the PCL. The notch is then widened from its base to the apex until the 9.5-mm-wide tip of the guide easily passes between the lateral femoral condyle and the PCL (Fig. 18-7). A roofplasty is not performed.

The tibial guide is then reinserted, and the knee is placed in full hyperextension (see Fig. 18-6). The heel of the patient’s leg is placed on the Mayo stand to maintain the knee in maximal hyperextension. The coronal alignment guide is inserted into the guide, the knee is brought into full hyperextension so that it is parallel to the roof, and the coronal alignment rod is adjusted so that it is parallel to the joint line and perpendicular to the tibia. The guidewire is drilled through the lateral hole in the bullet, which moves the guidewire laterally away from the PCL. The position of the guidewire is then checked arthroscopically. In the AP view the guidewire should enter midway between the lateral edge of the PCL and lateral femoral condyle. In full extension a probe can be placed between the anterior surface of the guidewire and the roof, and there should be 2 to 3 mm of clearance, which indicates that the guidewire is not placed too far posterior.
Once the graft is passed, a triangular space should be seen between the PCL and the ACL graft at the apex of the notch (Fig. 18-8).

Validation of Tibial Guide
One advantage of drilling the tibial tunnel with the knee in full hyperextension using the 65-degree tibial guide is that no manipulation of the knee is required to reduce the knee and drill the guidewire anatomically. Simply extending the knee and placing the heel on the Mayo stand suspends the knee and allows gravity to reduce the tibia on the femur.17
The 65-degree tibial guide was shown to place the tibial tunnel on the posterior half of the ACL footprint and avoid roof impingement without a roofplasty in a cadaveric study of 21 knees.13 Mapping demonstrated a wide variety in width, depth, and shape of the footprint of the intact ACL insertion, which emphasizes the difficulty in selecting the location of the tibial tunnel with use of a point-and-shoot guide and using the ACL insertion as a target. The consistency of the relationship of the ACL to the intercondylar roof and the inconsistency of the footprint substantiate the principle of using a tibial guide that registers the intercondylar roof with the knee in full hyperextension to select the position of the tibial guidewire.19
1 Fujimoto E, Sumen Y, Deie M, et al. Anterior cruciate ligament graft impingement against the posterior cruciate ligament: diagnosis using MRI plus three-dimensional reconstruction software. Magn Reson Imaging. 2004;22:1125-1129.
2 Howell SM, Gittins ME, Gottlieb JE, et al. The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med. 2001;29:567-574.
3 Simmons R, Howell SM, Hull ML. Effect of the angle of the femoral and tibial tunnels in the coronal plane and incremental excision of the posterior cruciate ligament on tension of an anterior cruciate ligament graft: an in vitro study. J Bone Joint Surg Am. 2003;85A:1018-1029.
4 Goss BC, Howell SM, Hull ML. Quadriceps load aggravates and roofplasty mitigates active impingement of anterior cruciate ligament grafts against the intercondylar roof. J Orthop Res. 1998;16:611-617.
5 Goss BC, Hull ML, Howell SM. Contact pressure and tension in anterior cruciate ligament grafts subjected to roof impingement during passive extension. J Orthop Res. 1997;15:263-268.
6 Howell SM, Clark JA, Farley TE. A rationale for predicting anterior cruciate graft impingement by the intercondylar roof. A magnetic resonance imaging study. Am J Sports Med. 1991;19:276-282.
7 Howell SM, Taylor MA. Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof. J Bone Joint Surg Am. 1993;75:1044-1055.
8 Howell SM, Berns GS, Farley TE. Unimpinged and impinged anterior cruciate ligament grafts: MR signal intensity measurements. Radiology. 1991;179:639-643.
9 Howell SM, Clark JA, Blasier RD. Serial magnetic resonance imaging of hamstring anterior cruciate ligament autografts during the first year of implantation. A preliminary study. Am J Sports Med. 1991;19:42-47.
10 Howell SM, Clark JA, Farley TE. Serial magnetic resonance study assessing the effects of impingement on the MR image of the patellar tendon graft. Arthroscopy. 1992;8:350-358.
11 Watanabe BM, Howell SM. Arthroscopic findings associated with roof impingement of an anterior cruciate ligament graft. Am J Sports Med. 1995;23:616-625.
12 Howell SM, Taylor MA. Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am. 1996;78:814-825.
13 Shelbourne KD, Kerr B. The relationship of femoral intercondylar notch width to height, weight, and sex in patients with intact anterior cruciate ligaments. Am J Knee Surg. 2001;14:92-96.
14 Howell SM, Barad SJ. Knee extension and its relationship to the slope of the intercondylar roof. Implications for positioning the tibial tunnel in anterior cruciate ligament reconstructions. Am J Sports Med. 1995;23:288-294.
15 Markolf KL, Hame SL, Hunter DM, et al. Biomechanical effects of femoral notchplasty in anterior cruciate ligament reconstruction. Am J Sports Med. 2002;30:83-89.
16 Howell SM. Principles for placing the tibial tunnel and avoiding roof impingement during reconstruction of a torn anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 1998;6:S49-S55.
17 Howell SM, Lawhorn KW. Gravity reduces the tibia when using a tibial guide that targets the intercondylar roof. Am J Sports Med. 2004;32:1702-1710.
18 www.drstevehowell.com/ezloc_video.cfm.
19 Cuomo P, Edwards A, Giron F, et al. Validation of the 65 degrees Howell guide for anterior cruciate ligament reconstruction. Arthroscopy. 2006;22:70-75.






