[level-membership-for-opthalmology-category]18.2
Tuberculosis
Clinical Features:
Ocular manifestations include choroidal granuloma, choroiditis, chorioretinitis, optic nerve infiltration, and uveitis (Figs 18.2.1 and 18.2.2). Choroidal involvement can cause a large plaque in the posterior pole, similar to that seen in serpiginous choroiditis, or can be multifocal in nature. Multiple old, inactive associated chorioretinal scars are suggestive of tuberculosis.

OCT Features:
OCT is particularly useful to image tuberculosis involvement of the retina and choroid. Infiltration in the subretinal space and choroid by a homogeneous material of medium to high reflectivity are typical early in the disease course (Fig. 18.2.3). There can be associated subretinal fluid. Resolving chorioretinitis can leave retinal and choroidal atrophy (Fig. 18.2.4).
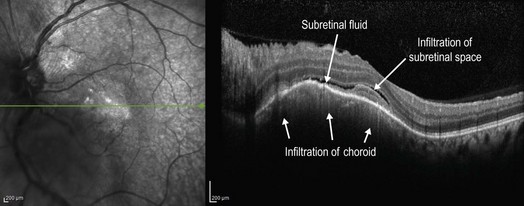
Figure 18.2.3 OCT (corresponding to Figure 18.2.1) shows homogeneous infiltration of the choroid causing an irregular, dome-shaped elevation of the overlying retinal pigment epithelium and retina. There is also infiltration of the subretinal space with a homogeneous material of medium reflectivity and associated subretinal fluid. (Courtesy of Alay S. Banker, MD.)
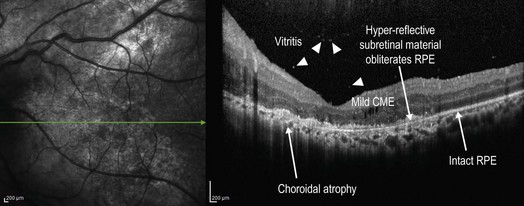
Figure 18.2.4 OCT (corresponding to Figure 18.2.2) of resolving tubercular chorioretinitis shows atrophy of the choroid. The subretinal space has a thin layer of hyper-reflective material that seems to have destroyed the RPE because there is negative shadowing that ends abruptly where the retinal pigment epithelium is intact. Other features include mild CME and small hyper-reflective deposits in the vitreous (arrowheads), which likely represent vitreous infiltration by tuberculosis organisms or secondary inflammation. (Courtesy of Alay S. Banker, MD.)
[/level-membership-for-opthalmology-category][not-level-membership-for-opthalmology-category]18.2
Tuberculosis
Clinical Features:
Ocular manifestations include choroidal granuloma, choroiditis, chorioretinitis, optic nerve infiltration, and uveitis (Figs 18.2.1 and 18.2.2). Choroidal involvement can cause a large plaque in the posterior pole, similar to that seen in serpiginous choroiditis, or can be multifocal in nature. Multiple old, inactive associated chorioretinal scars are suggestive of tuberculosis.

Figure 18.2.1 Color photograph of active tubercular chorioretinitis involving the macula and optic nerve. (Courtesy of Alay S. Banker, MD.)
[/not-level-membership-for-opthalmology-category]
