CHAPTER 27 Trochanteric Distalization (Relative Femoral Neck Lengthening) for Legg-Calvé-Perthes Disease and Coxa Vara
Imaging and diagnostic studies
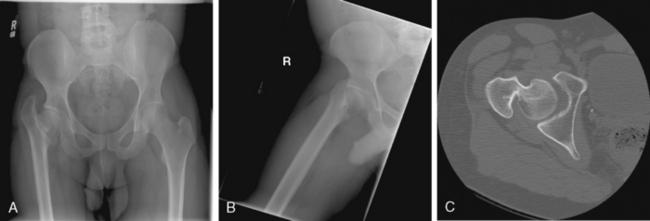
An anteroposterior pelvic view and frog-leg lateral view of the affected hip are required. In addition, an abduction view may be obtained if there is a question of bony impingement after looking at the radiographs (Figure 27-1). For the purposes of isolated distalization or lateralization of the trochanter, these studies will usually suffice.
Annotated references and suggested readings
Eilert R.E., Hill K., Back J. Greater trochanteric transfer for the treatment of coxa brevis. Clin Orthop Relat Res. 2005;434:92-101.
Free S.A., Delp S.L. Trochanteric transfer in total hip replacement: effects on the moment arms and force-generating capacities of the hip abductors. J Orthop Res. 1996;14:245-250.
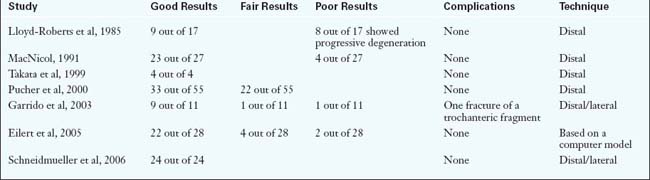
Garrido I.M., Molto F.J.L., Lluch D.B. Distal transfer of the greater trochanter in acquired coxa vara. Clinical and radiographic results. J Pediatr Orthop B. 2003;12:38-43.
Gore D.R., Murray M.P., Gardner G.M., Sepic S.B. Roentgenographic measurements after Muller total hip replacement: correlations among roentgenographic measurements and hip strength and mobility. J Bone Joint Sur Am. 1977;59:948-953.
Jani L. Die entwicklung des Schenkelhalses nach der trochanterversetsung. Arch orthop Unfallchirurgie. 1969;66:127-132.
Lloyd-Roberts G.C., Wetherill M.H., Fraser M. Trochanteric advancement for premature arrest of the femoral capital growth plate. J Bone Joint Surg (B). 1985;67–B:21-24.
MacNicol M.F., Makris D. Distal transfer of the greater trochanter. J Bone Joint Surg Br. 1991;73–B:838-841.
Pucher A., Ruszkowski K., Nowicki J., et al. Distal greater trochanteric transfer in the treatment of deformity of the proximal femur caused by avascular necrosis. Orthop Traumatol Rehabilitation. 2006;8:41-47.
Pucher A., Ruszkowski K., Bernardczyk K., Nowicki J. The value of distal greater trochanteric transfer in the treatment of deformity of the proximal femur owing to avascular necrosis. J Pediatr Orthop. 2000;20:311-316.
Schneidmueller D., Carstens C., Thomsen M. Surgical treatment of overgrowth of the greater trochanter in children and adolescents. J Pediatr Orthop. 2006;26:486-490.
Takata K., Maniwa S., Ochi M. Surgical treatment of high-standing greater trochanter. Arch Orthop Trauma Surg. 1999;119:461-463.