CHAPTER 47 Traditional inverted-T breast reduction
Physical evaluation
Technical steps
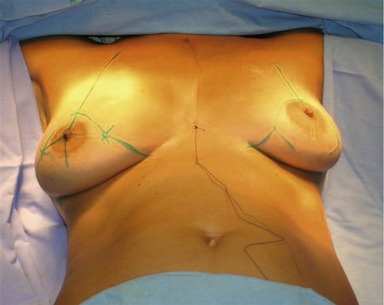
Patients are operated on under general anesthesia in a semi-seated position. Two sutures, one at the sternal notch and another at the xyphoid appendix, are placed. The hemiclavicular line is then marked. In this line, in the projection of the submammary crease, a point called “A” is marked (Figs 47.1 and 47.2). This point corresponds to the new site of the areola. From point A we mark points “B” and “C”, which will determine the new position of the breasts. These points depend on the relationship between skin and breast tissue. The lines A–B and A–C should not exceed 7 cm. The points B and C are then linked to the medial and lateral extremities of the breasts.
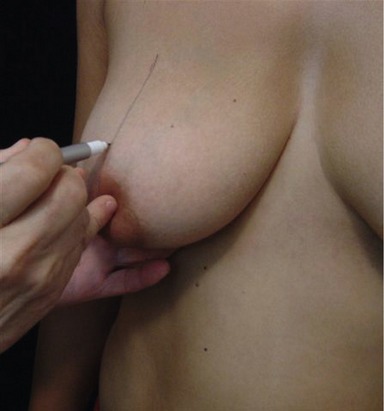


Fig. 47.3 Patient in the operating room. Semi-seated position. Rechecking height and position of points A.


Most of the sutures are intradermal. Sutures in the skin are removed around the tenth day after the operation.
Complications
• The most common complication of this operation is a slight dehiscence in the junction of the sutures in the median line.
• Hypertrophic scar may occur as in any surgical procedure.
• Hematoma, seroma, skin necrosis, dehiscence, and infection are extremely rare.
Summary of steps
1. Patients are operated on under general anesthesia in a semi-seated position.
2. Two sutures, one at the sternal notch and another at the xyphoid appendix, are placed.
3. The hemiclavicular line is then marked. In this line, in the projection of the submammary crease, a point called “A” is marked. This point corresponds to the new site of the areola.
4. From point A we mark points “B” and “C”, which will determine the new position of the breasts. These points depend on the relationship between skin and breast tissue.
5. The lines A–B and A–C should not exceed 7 cm. The points B and C are then linked to the medial and lateral extremities of the breasts.
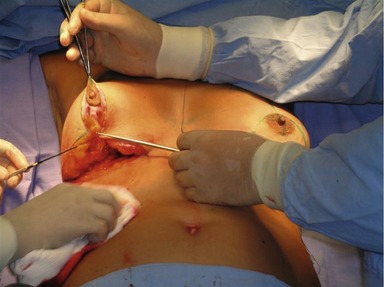
6. After the breasts are marked, an infiltration of a solution with adrenaline (epinephrine) 1/100,000 is placed in the areas that will be incised.
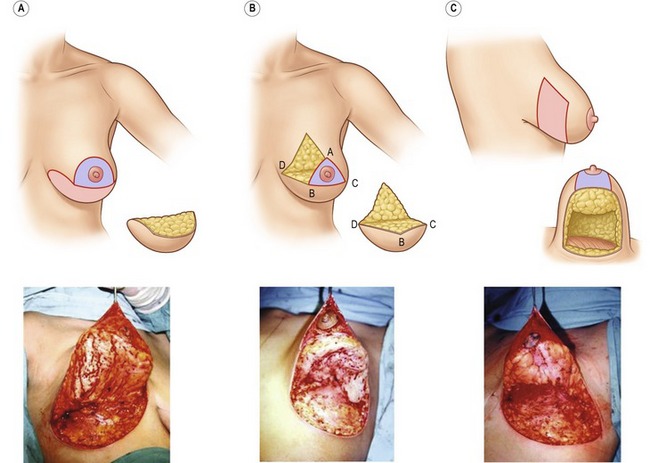
7. The incisions start at the areola with de-epithelialization of the surrounding areas in order to maintain innervation and vascularization.
8. Excess skin is then removed.
9. The breasts are then compared and sutured without tension so that after 8–18 months, the scars are largely inconspicuous.
10. Most of the sutures are intradermal. Sutures in the skin are removed around the tenth day after the operation.
Cardoso de Castro C. Mammaplasty with curved incisions. Plast Reconstr Surg. 1976;57:596.
Cardoso de Castro C. Late results after reduction mammaplasty with curved incisions. Plast Reconstr Surg. 1978;61:862.
Cardoso de Castro C. The value of non-prefixed marking in reduction mammaplasty. Aesthet Plast Surg. 1984;8:237.
Cardoso de Castro C. Mastopexy and breast reduction: breast shape and scar quality are most important. Aesthet Surg J. 2002;22:569.
Pontes R. Reduction mammaplasty – variations I and II. Ann Plast Surg. 1981;6:437.
Pitanguy I. Surgical treatment of breast hypertrophy. Br J Plast Surg. 1967;20:78.
Strombeck JO. Mammaplasty. Report of a new technique based on two pedicle procedure. Br J Plast Surg. 1960;13:79.
Wise RJ. A preliminary report on a method of planning the mammaplasty. Plast Reconstr Surg. 1956;17:367.





