Similar lesion may represent a pulsion diverticulum, due to esophageal dysmotility
• Chest x-ray PA view: Calcified perihilar lymph nodes
• Videofluoroscopic esophagogram (barium studies)
Mid esophagus: Traction diverticulum
Tented or triangular in shape with pointed tip, wide mouth
Diverticulum tends to empty when esophagus is collapsed (because it contains all layers)
TOP DIFFERENTIAL DIAGNOSES
• Zenker diverticulum
Posterior hypopharyngeal diverticulum
• Pulsion diverticulum
Mid and distal esophageal pulsion diverticula tend to remain filled after most of barium is emptied (lack of muscle)
Associated with motility disorders
• Esophageal perforation
Sealed-off leak seen as self-contained extraluminal collection of contrast medium that communicates with adjacent esophagus
May be indistinguishable from traction diverticulum without history
PATHOLOGY
• Pathogenesis: Acutely inflamed, enlarged subcarinal nodes indent and adhere to esophageal walls
As inflammation subsides, nodes shrink and retract adherent esophagus
CLINICAL ISSUES
• Small diverticula: Usually asymptomatic
• Large diverticula: ± dysphagia or regurgitation
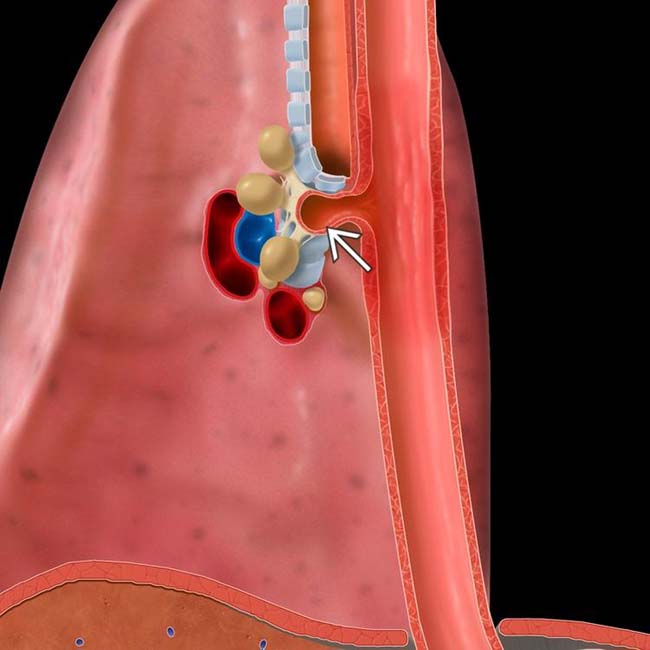
(Left) Graphic shows subcarinal lymph nodes that are adherent to the esophageal wall, resulting in a traction diverticulum .
(Right) Spot film from an esophagram shows a barium-filled tented outpouching from the mid esophagus. Calcified subcarinal lymph nodes were more evident on chest radiograph (not shown).
(Left) Oblique view from a barium esophagram demonstrates a saccular outpouching from the mid esophagus just below the tracheal carina, a typical appearance for a traction diverticulum.
(Right) Spot film from a barium esophagram shows a focal outpouching from the left mid esophagus. Although this may represent a traction diverticulum, it may rather be a normal outpouching of the esophageal wall between the extrinsic indentations by the aortic arch and the left mainstem bronchus.
Esophagram shows a mid esophageal diverticulum.
Esophagram shows outpouching at the subcarinal level.









 .
.
 from the mid esophagus. Calcified subcarinal lymph nodes
from the mid esophagus. Calcified subcarinal lymph nodes  were more evident on chest radiograph (not shown).
were more evident on chest radiograph (not shown).
 from the mid esophagus just below the tracheal carina, a typical appearance for a traction diverticulum.
from the mid esophagus just below the tracheal carina, a typical appearance for a traction diverticulum.
 from the left mid esophagus. Although this may represent a traction diverticulum, it may rather be a normal outpouching of the esophageal wall between the extrinsic indentations by the aortic arch and the left mainstem bronchus.
from the left mid esophagus. Although this may represent a traction diverticulum, it may rather be a normal outpouching of the esophageal wall between the extrinsic indentations by the aortic arch and the left mainstem bronchus.




