[level-membership-for-pediatrics-category]
Chapter 290 Toxocariasis (Visceral and Ocular Larva Migrans)
Clinical Manifestations
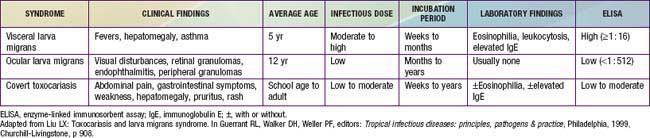
There are 3 major clinical syndromes associated with human toxocariasis: VLM, ocular larva migrans (OLM), and covert toxocariasis (Table 290-1). The classic presentation of VLM includes eosinophilia, fever, and hepatomegaly, and occurs most commonly in toddlers with a history of pica and exposure to puppies. The findings include fever, cough, wheezing, bronchopneumonia, anemia, hepatomegaly, leukocytosis, eosinophilia, and positive Toxocara serology. Cutaneous manifestations such as pruritis, eczema, and urticaria can be present. OLM tends to occur in older children without signs or symptoms of VLM. Presenting symptoms include unilateral visual loss, eye pain, white pupil, or strabismus that develops over a period of weeks. Granulomas occur on the posterior pole of the retina and may be mistaken for retinoblastoma. Serologic testing for Toxocara has allowed the identification of individuals with less obvious or covert symptoms of infection. These children may have nonspecific complaints that do not constitute a recognizable syndrome. Common findings include hepatomegaly, abdominal pain, cough, sleep disturbance, failure to thrive, and headache with elevated Toxocara antibody titers. Eosinophilia may be present in only 50-75% of cases. The prevalence of positive Toxocara serology in the general population supports the notion that most children with T. canis infection are asymptomatic and will not develop overt clinical sequelae over time. A correlation between positive Toxocara serology and allergic asthma has also been described.
Diagnosis
A presumptive diagnosis can be established in a young child with eosinophilia (>20%), leukocytosis, hepatomegaly, fevers, wheezing, and a history of geophagia and exposure to puppies or unrestrained dogs. Supportive laboratory findings include hypergammaglobulinemia and elevated isohemagglutinin titers to A and B blood group antigens. Most patients with VLM have an absolute eosinophil count of >500/µL. Eosinophilia is less common in subjects with OLM. Biopsy confirms the diagnosis. When biopsies cannot be obtained, an enzyme-linked immunosorbent assay using excretory-secretory proteins harvested from T. canis larvae maintained in vitro is the standard serologic test used to confirm toxocariasis. The sensitivity is approximately 78% and specificity 92% at a titer of 1 : 42. The sensitivity for OLM is significantly less. The diagnosis of OLM can be established in patients with typical clinical findings of a retinal or peripheral pole granuloma or endophthalmitis with elevated antibody titers. Vitreous and aqueous humor fluid anti-Toxocara titers are usually greater than serum titers. The diagnosis of covert toxocariasis should be considered in individuals with chronic weakness, abdominal pain, or allergic signs with eosinophilia and increased IgE. In temperate regions of the world, nonparasitic causes of eosinophilia that should be considered in the differential diagnosis include allergies, drug hypersensitivity, lymphoma, vasculitis, and the idiopathic hypereosinophilic syndrome (Chapter 123).
Gavignet B, Piarroux R, Aubin F, et al. Cutaneous manifestations of human toxocariasis. J Am Acad Dermatol. 2008;59:1031-1042.
Graeff-Teixeira CM, da Silva ACA, Yoshimura K. Update on eosinophilic meningoencephalitis and its clinical relevance. Clin Microbiol Rev. 2009;22:322-348.
Hotez PJ, Wlikins PP. Toxocariasis: America’s most common neglected infection of poverty and a helminthiasis of global importance? PLoS Negl Trop Dis. 2009;3:e400.
Litwin CM. Pet-transmitted infections: diagnosis by microbiologic and immunologic methods. Pediatr Infect Dis J. 2003;22:768-777.
Sabrosa NA, Zajdenweber M. Nematode infections of the eye: toxocariasis, onchocerciasis, diffuse unilateral subacute neuroretinitis, and cysticercosis. Ophthalmol Clin North Am. 2002;15:351-356.
Schantz PM, Glickman LT. Toxocaral visceral larva migrans. N Engl J Med. 1978;298:436-439.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
Chapter 290 Toxocariasis (Visceral and Ocular Larva Migrans)
[/not-level-membership-for-pediatrics-category]
