[level-membership-for-neurosurgery-category]
CHAPTER 31 Thorascopic Spine Surgery
The applications of endoscopic spine surgery have been expanded since the first publications spanning nearly two decades.1–6 Operating techniques have been standardized and unified and today are safe procedures with low complication rates that are comparable to those of open procedures, presuming the existence of adequate training and manual skills of the surgeon.7 Thus, endoscopic operations on the spinal column no longer represent exceptional interventions but have become standard procedures in spine surgery. Thoracoscopic techniques can be used to approach the anterior column of the spine in the area between the third thoracic vertebra and the third lumbar vertebra because endoscopic splitting of the diaphragm also allows the exposure of the upper sections of the lumbar spine. The application potential includes anterior release procedures, with incision and resection of ligaments and intervertebral disks; removal of fragmented disks or sections of vertebrae, including anterior decompression of the spinal canal; replacement of vertebral bodies with biologic or alloplastic materials; and ventral stabilization procedures with implants designed for use in endoscopic spine surgery. In addition, percutaneous endoscopic techniques are used for minimally invasive treatment of degenerative disk disease of the thoracic and lumbar spine.
Indications
Overall, the range of indications for the technique described here can be defined as follows:
Technical Requirements
Image Transmission
The key to any endoscopic technique is image recording and transmission. “You will do what you can see,” and therefore true high-definition video technique has also revolutionized the endoscopic technique, which now provides an endoscopic view comparable to images that the microscope is able to provide. A high-intensity xenon light source is required to illuminate the thoracic cavity. A rigid, long, 30-degree scope enables positioning of the camera far away from the working portal, thus facilitating undisturbed working and variable adjustment of the angle of vision. The intraoperative view is transmitted onto two or three flat screens (Fig. 31-1).

Instruments
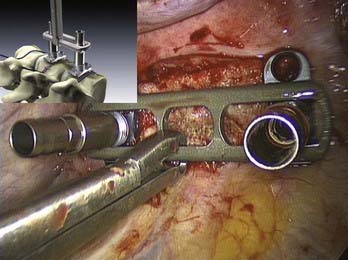
 Complete sets of instruments for soft tissue and bone preparation are manufactured by contemporary instrument manufacturers (Fig. 31-2). Instruments should have a nonreflective surface and a depth scale on both sides and be ergonomically designed with big handles for safe control and handling. The technique by which they are used is called the three-point anchoring technique, which means that every sharp and potentially dangerous instrument is guided by both hands; one hand is based on the chest wall, always controlling and sometimes neutralizing unexpected forces and movements of the instrument (see Video 31-9).
Complete sets of instruments for soft tissue and bone preparation are manufactured by contemporary instrument manufacturers (Fig. 31-2). Instruments should have a nonreflective surface and a depth scale on both sides and be ergonomically designed with big handles for safe control and handling. The technique by which they are used is called the three-point anchoring technique, which means that every sharp and potentially dangerous instrument is guided by both hands; one hand is based on the chest wall, always controlling and sometimes neutralizing unexpected forces and movements of the instrument (see Video 31-9).

Implants
Several implants for anterior instrumentation that can be used for endoscopic, mini-open, or open spine surgery are now available. Most of them are based on the principle of a cannulated screw and plate system, first allowing the implantation of K wires under fluoroscopic control to be used as landmarks, followed by the insertion of screws. Biomechanically tested four-point fixation implants provide adequate angular stability, which is necessary for single anterior instrumentation (Fig. 31-3).13
For vertebral body replacement, bone graft (autograft or allograft) or mechanical devices can be used and filled or surrounded with the autologous bone harvested from the corpectomy site. A wide variety of expandable titanium cages is currently available.14
Preoperative Requirements
Education of the Patient
The patient should be informed about the following approach-specific risks and hazards:
 All endoscopic operations at the anterior column of the thoracic spine and the thoracolumbar junction are performed with the patient lying on his or her side (Video 31-1). The approach side is determined by the preoperative computed tomographic (CT) scans and depends on the position of the major vessels shown in the scans and the surgery that is planned. Because of the great variability of the vascular anatomy, firm rules are no longer set for selection of the approach side by the height of the lesion.
All endoscopic operations at the anterior column of the thoracic spine and the thoracolumbar junction are performed with the patient lying on his or her side (Video 31-1). The approach side is determined by the preoperative computed tomographic (CT) scans and depends on the position of the major vessels shown in the scans and the surgery that is planned. Because of the great variability of the vascular anatomy, firm rules are no longer set for selection of the approach side by the height of the lesion.Marking the Portals
 As a routine, four portals are used: scope portal, working portal, suction-irrigation portal, and retractor portal (Video 31-2). Their location and, in particular, the position of the working portal are crucial for the endoscopic operation to proceed in the optimal fashion. For this reason, the lesion is first displayed in the lateral projection (with reference to the patient’s body) under precise adjustment of the image intensifier, and a marker is used to draw the injured spinal section onto the lateral thoracic wall (Fig. 31-4). The working portal is drawn in directly above the lesion. The trocar for the endoscope is marked either caudal or cranial to the working portal, depending on the height of the lesion, and following the axis of the spine. The distance from the working portal is approximately two intercostal spaces. The entry points for suction and irrigation and for the retractor are then located ventral from these portals.
As a routine, four portals are used: scope portal, working portal, suction-irrigation portal, and retractor portal (Video 31-2). Their location and, in particular, the position of the working portal are crucial for the endoscopic operation to proceed in the optimal fashion. For this reason, the lesion is first displayed in the lateral projection (with reference to the patient’s body) under precise adjustment of the image intensifier, and a marker is used to draw the injured spinal section onto the lateral thoracic wall (Fig. 31-4). The working portal is drawn in directly above the lesion. The trocar for the endoscope is marked either caudal or cranial to the working portal, depending on the height of the lesion, and following the axis of the spine. The distance from the working portal is approximately two intercostal spaces. The entry points for suction and irrigation and for the retractor are then located ventral from these portals.

 After skin disinfection and sterile draping, single-lung ventilation is begun in consultation with the anesthetist. As the first approach, the portal in the farthest cranial position is always selected because the risk of injury to the liver, spleen, and diaphragm is comparatively minor in this position. The approach is made by the mini-thoracotomy technique, providing the possibility of examining the immediate surroundings of the insertion site with the fingers before the trocar is introduced (Video 31-3). The rigid 30-degree endoscope is then carefully inserted, and the thoracic cavity is first inspected to rule out the existence of adhesions or parenchymal lesions. The other three trocars and then the instruments are subsequently introduced under endoscopic control.
After skin disinfection and sterile draping, single-lung ventilation is begun in consultation with the anesthetist. As the first approach, the portal in the farthest cranial position is always selected because the risk of injury to the liver, spleen, and diaphragm is comparatively minor in this position. The approach is made by the mini-thoracotomy technique, providing the possibility of examining the immediate surroundings of the insertion site with the fingers before the trocar is introduced (Video 31-3). The rigid 30-degree endoscope is then carefully inserted, and the thoracic cavity is first inspected to rule out the existence of adhesions or parenchymal lesions. The other three trocars and then the instruments are subsequently introduced under endoscopic control.Operative Techniques
Approach to the Thoracolumbar Junction
 This operation is also performed using single-lung ventilation (Video 31-4).8,11,15,16 Here, too, the approach side is decided by the location of the major vessels, which can be identified from the preoperative computed tomographic scan. In most cases, the best approach to the thoracolumbar junction is from the left. Placement of the trocars and instruments is illustrated in Figure 31-5.
This operation is also performed using single-lung ventilation (Video 31-4).8,11,15,16 Here, too, the approach side is decided by the location of the major vessels, which can be identified from the preoperative computed tomographic scan. In most cases, the best approach to the thoracolumbar junction is from the left. Placement of the trocars and instruments is illustrated in Figure 31-5.
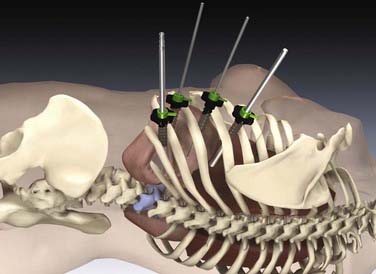
FIGURE 31-5 Placement of the trocars and instruments for an endoscopic intervention at the thoracolumbar spine.
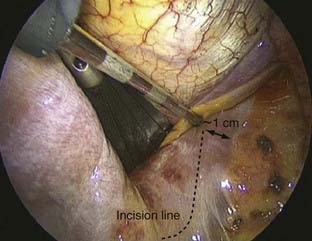
The dome-like diaphragm is firmly connected at its margins with the sternum, ribs, and spine and arches up into the thoracic cavity. Topographically speaking, the attachment sites of the diaphragm to the spine are at the level of the first lumbar vertebra, whereas the lowest point of the thoracic cavity projects with the phrenicocostal sinus at the level of the baseplate of the second lumbar vertebra (Fig. 31-6). This makes it possible to place a trocar intrathoracically in the phrenicocostal sinus, which, after incision of the diaphragm attachment to the spine, provides access to the retroperitoneal section of the thoracolumbar junction down to the baseplate of the second lumbar vertebra. This requires a 4- to 5-cm–long incision following the attachment of the diaphragm; access to the L1-2 intervertebral disk can be obtained with a shorter incision of 2 to 3 cm (Fig. 31-7).15–17

Endoscopic Treatment of Spinal Trauma (Anterior Reconstruction)
 As a first step, landmarks are set under image intensifier control to serve as orientation points for the surgeon and camera operator during the subsequent course of the operation (Video 31-5). For this, the K wires associated with the implant are used; these are then replaced by cannulated screws with integrated clamping elements. If no implant is used, marker points can be set onto the parietal pleura under fluoroscopic control by use of the cautery or ultrasonic knife. Thus, these K wires also define the later position of the screws, and they are placed near the end plates between the posterior and central thirds of the vertebra. To achieve this in the thoracolumbar junction region, the psoas muscle must be mobilized ventrad to dorsad, thus avoiding irritation of the fibers of the lumbar plexus. Through positioning of the K wires near the end plates, injury to the segment vessels is avoided, and the screws are anchored in a region of higher bone density.
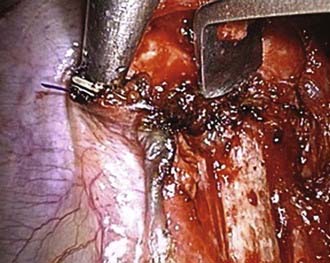
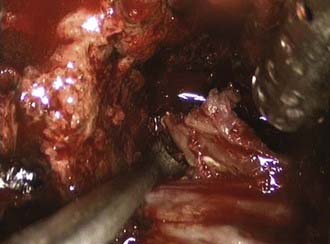
As a first step, landmarks are set under image intensifier control to serve as orientation points for the surgeon and camera operator during the subsequent course of the operation (Video 31-5). For this, the K wires associated with the implant are used; these are then replaced by cannulated screws with integrated clamping elements. If no implant is used, marker points can be set onto the parietal pleura under fluoroscopic control by use of the cautery or ultrasonic knife. Thus, these K wires also define the later position of the screws, and they are placed near the end plates between the posterior and central thirds of the vertebra. To achieve this in the thoracolumbar junction region, the psoas muscle must be mobilized ventrad to dorsad, thus avoiding irritation of the fibers of the lumbar plexus. Through positioning of the K wires near the end plates, injury to the segment vessels is avoided, and the screws are anchored in a region of higher bone density. Following the connecting line between the K wires, the pleura is opened, and the segment vessels are exposed with a Cobb raspatory. These vessels are mobilized subperiosteally from both sides, ligated twice with titanium clips ventrally and dorsally, and raised slightly with a nerve hook. The vessels are dissected with the endoscopic hook scissors. The lateral aspects of the vertebral body and the disks are exposed with the raspatory (Video 31-6).
Following the connecting line between the K wires, the pleura is opened, and the segment vessels are exposed with a Cobb raspatory. These vessels are mobilized subperiosteally from both sides, ligated twice with titanium clips ventrally and dorsally, and raised slightly with a nerve hook. The vessels are dissected with the endoscopic hook scissors. The lateral aspects of the vertebral body and the disks are exposed with the raspatory (Video 31-6). The K wires are now overdrilled with a cannulated broach, and the lateral cortex of the vertebral body is opened (Video 31-7). The working trocar is exchanged for a speculum through a switching stick, and the clamping element is tightened with a screw. The length of the screw has been previously measured against the preoperative computed tomographic scan and subsequently defines whether a monocortical or bicortical screw fixation is to be attempted. The direction of the screw can be altered after removal of the K wire and checked in both planes under C-arm monitoring. The connecting line between the screws and the anterior boundary of the clamping elements now defines an area of safety within which the partial removal of the vertebral body and the disks is performed. The ventral and dorsal extent of the partial corpectomy thus defined also then corresponds to the dimensions of the planned vertebral body replacement, which has a transverse diameter between 16 mm (thoracic) and 20 mm (lumbar).
The K wires are now overdrilled with a cannulated broach, and the lateral cortex of the vertebral body is opened (Video 31-7). The working trocar is exchanged for a speculum through a switching stick, and the clamping element is tightened with a screw. The length of the screw has been previously measured against the preoperative computed tomographic scan and subsequently defines whether a monocortical or bicortical screw fixation is to be attempted. The direction of the screw can be altered after removal of the K wire and checked in both planes under C-arm monitoring. The connecting line between the screws and the anterior boundary of the clamping elements now defines an area of safety within which the partial removal of the vertebral body and the disks is performed. The ventral and dorsal extent of the partial corpectomy thus defined also then corresponds to the dimensions of the planned vertebral body replacement, which has a transverse diameter between 16 mm (thoracic) and 20 mm (lumbar).
 The intervertebral disks are incised laterally with a knife, and the disk space is opened with a slightly offset osteotome (Video 31-8). The posterior osteotomy is then performed with a straight osteotome from disk space to disk space on the connecting line between the screws. The scale on the osteotome shows the corresponding depth, which in the anterior direction should be about two thirds of the diameter of the vertebra. The line of the anterior osteotomy runs along the anterior boundary of the clamping elements; to be sure of avoiding unintentional perforation of the anterior vertebral wall (and adjacent vessels), an osteotome that is slightly angled to the rear is used. The central section of the vertebral body is now removed with a rongeur, and the removed cancellous bone is preserved for later implantation adjacent to the vertebral body replacement (Video 31-9). Using a curet and rongeurs, the intervertebral disks are then resected and the end plates are freshened up. When titanium cages are implanted, any weakening of the load-bearing end plates must be avoided. In monosegmental fusion with a tricortical pelvic crest graft, the subchondral bone lamella on the cranial end plate is removed to assist healing of the bone graft.
The intervertebral disks are incised laterally with a knife, and the disk space is opened with a slightly offset osteotome (Video 31-8). The posterior osteotomy is then performed with a straight osteotome from disk space to disk space on the connecting line between the screws. The scale on the osteotome shows the corresponding depth, which in the anterior direction should be about two thirds of the diameter of the vertebra. The line of the anterior osteotomy runs along the anterior boundary of the clamping elements; to be sure of avoiding unintentional perforation of the anterior vertebral wall (and adjacent vessels), an osteotome that is slightly angled to the rear is used. The central section of the vertebral body is now removed with a rongeur, and the removed cancellous bone is preserved for later implantation adjacent to the vertebral body replacement (Video 31-9). Using a curet and rongeurs, the intervertebral disks are then resected and the end plates are freshened up. When titanium cages are implanted, any weakening of the load-bearing end plates must be avoided. In monosegmental fusion with a tricortical pelvic crest graft, the subchondral bone lamella on the cranial end plate is removed to assist healing of the bone graft. In monosegmental reconstructions and fusion, a tricortical bone graft taken from the iliac crest is used. After the corpectomy defect has been measured, the iliac crest is prepared and exposed. Using an oscillating saw and chisel, the bone graft is harvested and firmly connected to a graft holder. The graft is inserted in a centered position into the defect, which has to be fluoroscopically checked in both planes (Video 31-10).
In monosegmental reconstructions and fusion, a tricortical bone graft taken from the iliac crest is used. After the corpectomy defect has been measured, the iliac crest is prepared and exposed. Using an oscillating saw and chisel, the bone graft is harvested and firmly connected to a graft holder. The graft is inserted in a centered position into the defect, which has to be fluoroscopically checked in both planes (Video 31-10).Ventral Instrumentation with a Constraint Plate Implant
 Because the screws and so-called clamping elements belonging to the implant were placed into position as a first step before the beginning of the partial corpectomy, now the plate just has to be fastened and the ventral screws of the four-point fixation inserted (Video 31-11).
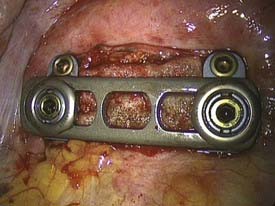
Because the screws and so-called clamping elements belonging to the implant were placed into position as a first step before the beginning of the partial corpectomy, now the plate just has to be fastened and the ventral screws of the four-point fixation inserted (Video 31-11).The distance between the screws is defined with a special measuring instrument to select a plate of the correct length. This is introduced lengthwise into the thoracic cavity through the incision for the working portal, laid onto the clamping elements with a holding forceps, and there definitively fixed with nuts with a starting torque of 15 Nm. The plate can be brought into direct bone contact with the lateral vertebral body wall by tightening the bone screws. The ventral screws are inserted after temporary fixation of a targeting device and opening of the cortex. Because of the heart shape of the vertebral body, the ventral screws are usually 5 mm shorter than the dorsal screws. The fixation of the angle-stable implant ends with the insertion of a locking screw that locks the polyaxial mechanism of the dorsal screws (Fig. 31-8).
 In every case, radiographs are taken in both planes with the C-arm to check the position of the implant before the operation is concluded (Video 31-12). For operations on the thoracolumbar junction that include incision of the diaphragmatic attachment, an incision longer than 2 cm should be closed with endoscopic suturing. Two or three adapting sutures are sufficient, depending on the extent of the incision. The suture does not need to be watertight.
In every case, radiographs are taken in both planes with the C-arm to check the position of the implant before the operation is concluded (Video 31-12). For operations on the thoracolumbar junction that include incision of the diaphragmatic attachment, an incision longer than 2 cm should be closed with endoscopic suturing. Two or three adapting sutures are sufficient, depending on the extent of the incision. The suture does not need to be watertight.Special Indications
Removal of Posterior Wall Fragments: Endoscopic Anterior Decompression9
Operative Technique
Case Report
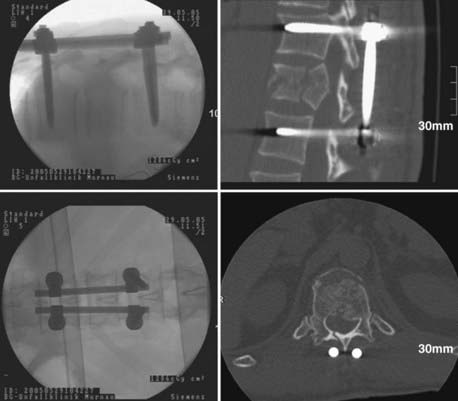
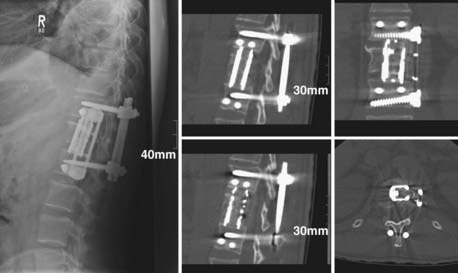
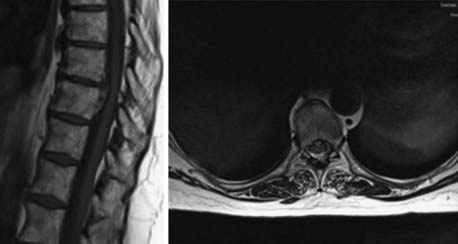
A 43-year-old man was referred to our hospital demonstrating severe back pain at the thoracolumbar junction, weakness of the lower extremities below T12, and moderate bowel and bladder dysfunction. After radiologic diagnostics and neurological examination, the patient was brought to the operating room for dorsal reduction and stabilization by internal fixator followed by thoracoscopic anterior decompression and reconstruction (Figs. 31-9 to 31-11).

Removal of Protruded Herniated Disk: Endoscopic Treatment of Degenerative Disk Disease
Only 0.15% to 1% of all operative procedures due to degenerative disk disease are done to treat thoracic disk protrusion.18–20 As a specialty of the thoracic region, there is a “calcified disk” and an “intradural disk herniation” (Fig. 31-12). These removal procedures are technically demanding. Because of a smaller diameter of the thoracic spinal canal in conjunction with a spinal cord of bigger volume at these levels, there is little space to accommodate disk herniation. In consequence, small disk protrusions might cause significant symptoms. Depending on the localization and expansion of herniation—medial, mediolateral, intraforaminal, or extraforaminal—typical symptoms of thoracic disk herniation can be described.
Operative Treatment Options
The following procedures21 are available, fitting the needed level and herniation site:
 Because of the high morbidity of the open transthoracic approach, indications were few. The advent of a tissue-preserving thoracoscopic approach6,12,24 led to greater numbers of indications, centrolateral and lateral disk herniations remaining to be approached posterolaterally. The thoracoscopic approach and operative technique are described here (Video 31-13).
Because of the high morbidity of the open transthoracic approach, indications were few. The advent of a tissue-preserving thoracoscopic approach6,12,24 led to greater numbers of indications, centrolateral and lateral disk herniations remaining to be approached posterolaterally. The thoracoscopic approach and operative technique are described here (Video 31-13).
Operating Room Setup
Positioning the Patient
The side for the approach has to be chosen primarily by the localization of the disk herniation and the adjacent great vessels. In cases of centromedial and right lateral herniation, the approach from the right side is preferred (Fig. 31-13).

Confirmation of the Operative Site
Verification of the level of disease can be demanding before the main procedure is started. Several methods are recommended to ensure that the right intervertebral disk space is addressed. Dickman and Rosenthal12 recommend a preoperative radiograph of the chest to localize the level. Large osteophytes seen on computed tomographic scans or plain radiographs can be used as surgical or radiographic landmarks. After the endoscopic procedure has started, it is recommended that the ribs be counted with use of the C-arm, beginning caudally at the 12th rib. Rib identification should be repeated several times to ensure accuracy. The pleura over the identified rib head is then cauterized. Attention must be paid to the patient with an abnormal number of ribs, because the spinal level could be misidentified.
Operative Technique
The general principle of the procedure is to resect the rib head of the adjacent rib and expose the pedicle and the affected intervertebral disk (Fig. 31-14). A block-shaped defect will then be created in the adjacent vertebral bodies for removal of soft and calcified disk material away from the dura into the defect. Afterward, the rib head, which usually fits into the defect, is used for a monosegmental fusion procedure to be accomplished by ventral instrumentation.
Technical and Operative Details
Partial corpectomy is performed with a high-speed diamond bur or an osteotome, creating a well-defined, block-shaped central defect involving the upper and lower thirds of the adjacent vertebral bodies. Initially, the posterior vertebral body wall is preserved (Fig. 31-15).
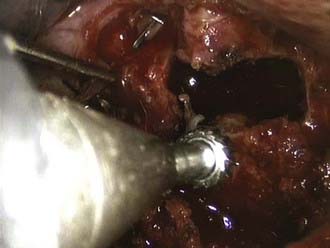
FIGURE 31-15 Partial corpectomy T9 and T10 with a high-speed bur to create a defect in the vertebral bodies in front.
Once the base of the pedicle caudal to the intervertebral disk space is identified, the thickness can be reduced with a diamond bur to weaken the pedicle and to facilitate the transection with Kerrison rongeurs. Dickman12 recommends starting at the upper rim of the pedicle because of less bleeding from the epidural venous plexus. Under direct endoscopic view of the dura, the posterior wall is then dissected off the dura and carefully pushed into the corpectomy site or thinned out with a high-speed diamond bur. The sequestered part of the disk is then removed with dissectors and rongeurs. If there is an intradural calcified herniated disk, the intradural part of the sequestrated disk has to be carefully separated from the arachnoid mater with microdissection (Fig. 31-16). Even if this is not possible without tearing the dura, the base of the calcified disk can be thinned with the diamond bur, leaving only a shell of calcification attached to the dura free to move without bone or soft tissue impingement. Complete decompression of the dural sac across the vertebral body to the level of the contralateral pedicle is confirmed by direct endoscopic view and radiologically by fluoroscopy with use of a nerve hook in an anteroposterior projection. After decompression, the dura is covered with Gelfoam. The corpectomy defect is reconstructed with the rib head harvested at the first step. The size of the graft is determined with an endoscopic measurement of the defect.
Alberico AM, Sahni KS, Hall JAJr, et al. High thoracic disc herniation. Neurosurgery. 1986;19:449-451.
Albrand OW, Corkill G. Thoracic disc herniation. Treatment and prognosis. Spine. 1979;4:41-46.
Awwad EE, Martin DS, Smith KRJr, et al. Asymptomatic versus symptomatic herniated thoracic discs: their frequency and characteristics as detected by computed tomography after myelography. Neurosurgery. 1991;28:180-186.
Beisse R. Video-assisted techniques in the management of thoracolumbar fractures. Orthop Clin North Am. 2007;38:419-429.
Beisse R. Endoscopic surgery on the thoracolumbar junction of the spine. Eur Spine J. 2006;15:687-704.
Beisse R, Muckley T, Schmidt MH, et al. Surgical technique and results of endoscopic anterior spinal canal decompression. J Neurosurg Spine. 2005;2:128-136.
Beisse R, Potulski M, Beger J, et al. Development and clinical application of a thoracoscopic implantable frame plate for the treatment of thoracolumbar fractures and instabilities. Orthopäde. 2002;31:413-422.
Beisse R, Potulski M, Bühren V. Endoscopic techniques for the management of spinal trauma. Eur J Trauma. 2001;27:275-291.
Beisse R, Potulski M, Temme C, et al. [Endoscopically controlled division of the diaphragm. A minimally invasive approach to ventral management of thoracolumbar fractures of the spine.]. Unfallchirurg. 1998;101:619-627.
Beisse R, Trapp O. Thoracoscopic management of spinal trauma. Oper Tech Neurosurg. 2006;8:205-213.
Dickman CA, Rosenthal DJ, Perin NI. Thoracoscopic Spine Surgery. New York: Thieme; 1999.
Horowitz MB, Moossy JJ, Julian T, et al. Thoracic discectomy using video assisted thoracoscopy. Spine. 1994;19:1082-1086.
Kim DH, Jahng TA, Balabhadra RS, et al. Thoracoscopic transdiaphragmatic approach to thoracolumbar junction fractures. Spine J. 2004;4:317-328.
Knop C, Bastian L, Lange U, et al. Complications in surgical treatment of thoracolumbar injuries. Eur Spine J. 2002;11:214-226.
Knop C, Lange U, Bastian L, et al. Biomechanical compression tests with a new implant for thoracolumbar vertebral body replacement. Eur Spine J. 2001;10:30-37.
Le Roux PD, Haglund MM, Harris AB. Thoracic disc disease: experience with the transpedicular approach in twenty consecutive patients. Neurosurgery. 1993;33:58-66.
Mack MJ, Aronoff RJ, Acuff TE, et al. Present role of thoracoscopy in the diagnosis and treatment of diseases of the chest. Ann Thorac Surg. 1992;54:403-408.
Mack MJ, Regan J, Bobechko WP, et al. Applications of thoracoscopy for diseases of spine. Ann Thorac Surg. 1993;56:736-738.
Maiman DJ, Larson SJ, Luck E, et al. Lateral extracavitary approach to the spine for thoracic disc herniation: report of 23 cases. Neurosurgery. 1984;14:178-182.
McAfee PC, Regan JR, Zdeblick T, et al. The incidence of complications in endoscopic anterior thoracolumbar spinal reconstructive surgery. A prospective multicenter study comprising the first 100 consecutive cases. Spine. 1995;20:1624-1632.
Regan JJ, McAfee P, Mack M. Atlas of Endoscopic Spine Surgery. St. Louis: Quality Medical; 1995.
Rosenthal D, Marquardt G, Lorenz R, et al. Anterior decompression and stabilization using a microsurgical endoscopic technique for metastatic tumors of the thoracic spine. J Neurosurg. 1996;8:565-572.
Rosenthal D, Rosenthal R, Simone A. Removal of a protruded disc using microsurgery endoscopy. Spine. 1994;19:1087-1091.
Stillerman CB, Chen TC, Day JD, et al. The transfacet pedicle-sparing approach for thoracic disc removal: cadaveric morphometric analysis and preliminary clinical experience. J Neurosurg. 1995;83:971-976.
1 Mack MJ, Aronoff RJ, Acuff TE, et al. Present role of thoracoscopy in the diagnosis and treatment of diseases of the chest. Ann Thorac Surg. 1992;54:403-408.
2 Mack MJ, Regan J, Bobechko WP, et al. Applications of thoracoscopy for diseases of spine. Ann Thorac Surg. 1993;56:736-738.
3 McAfee PC, Regan JR, Zdeblick T, et al. The incidence of complications in endoscopic anterior thoracolumbar spinal reconstructive surgery. A prospective multicenter study comprising the first 100 consecutive cases. Spine. 1995;20:1624-1632.
4 Regan JJ, McAfee P, Mack M. Atlas of Endoscopic Spine Surgery. St. Louis: Quality Medical; 1995.
5 Rosenthal D, Marquardt G, Lorenz R, et al. Anterior decompression and stabilization using a microsurgical endoscopic technique for metastatic tumors of the thoracic spine. J Neurosurg. 1996;8:565-572.
6 Rosenthal D, Rosenthal R, Simone A. Removal of a protruded disc using microsurgery endoscopy. Spine. 1994;19:1087-1091.
7 Knop C, Bastian L, Lange U, et al. Complications in surgical treatment of thoracolumbar injuries. Eur Spine J. 2002;11:214-226.
8 Beisse R. Video-assisted techniques in the management of thoracolumbar fractures. Orthop Clin North Am. 2007;38:419-429.
9 Beisse R, Muckley T, Schmidt MH, et al. Surgical technique and results of endoscopic anterior spinal canal decompression. J Neurosurg Spine. 2005;2:128-136.
10 Beisse R, Trapp O. Thoracoscopic management of spinal trauma. Oper Tech Neurosurg. 2006;8:205-213.
11 Beisse R. Endoscopic surgery on the thoracolumbar junction of the spine. Eur Spine J. 2006;15:687-704.
12 Dickman CA, Rosenthal DJ, Perin NI. Thoracoscopic Spine Surgery. New York: Thieme; 1999.
13 Beisse R, Potulski M, Beger J, et al. [Development and clinical application of a thoracoscopy implantable plate frame for treatment of thoracolumbar fractures and instabilities.]. Orthopade. 2002;31:413-422.
14 Knop C, Lange U, Bastian L, et al. Biomechanical compression tests with a new implant for thoracolumbar vertebral body replacement. Eur Spine J. 2001;10:30-37.
15 Beisse R, Potulski M, Temme C, et al. [Endoscopically controlled division of the diaphragm. A minimally invasive approach to ventral management of thoracolumbar fractures of the spine.]. Unfallchirurg. 1998;101:619-627.
16 Kim DH, Jahng TA, Balabhadra RS, et al. Thoracoscopic transdiaphragmatic approach to thoracolumbar junction fractures. Spine J. 2004;4:317-328.
17 Beisse R, Potulski M, Bühren V. Endoscopic techniques for the management of spinal trauma. Eur J Trauma. 2001;27:275-291.
18 Alberico AM, Sahni KS, Hall JAJr, et al. High thoracic disc herniation. Neurosurgery. 1986;19:449-451.
19 Albrand OW, Corkill G. Thoracic disc herniation. Treatment and prognosis. Spine. 1979;4:41-46.
20 Awwad EE, Martin DS, Smith KRJr, et al. Asymptomatic versus symptomatic herniated thoracic discs: their frequency and characteristics as detected by computed tomography after myelography. Neurosurgery. 1991;28:180-186.
21 Stillerman CB, Chen TC, Day JD, et al. The transfacet pedicle-sparing approach for thoracic disc removal: cadaveric morphometric analysis and preliminary clinical experience. J Neurosurg. 1995;83:971-976.
22 Maiman DJ, Larson SJ, Luck E, et al. Lateral extracavitary approach to the spine for thoracic disc herniation: report of 23 cases. Neurosurgery. 1984;14:178-182.
23 Le Roux PD, Haglund MM, Harris AB. Thoracic disc disease: experience with the transpedicular approach in twenty consecutive patients. Neurosurgery. 1993;33:58-66.
24 Horowitz MB, Moossy JJ, Julian T, et al. Thoracic discectomy using video assisted thoracoscopy. Spine. 1994;19:1082-1086.
25 Beisse R, Potulski M, Beger J, et al. Development and clinical application of a thoracoscopic implantable frame plate for the treatment of thoracolumbar fractures and instabilities. Orthopade. 2002;31:413-422.
[/level-membership-for-neurosurgery-category][not-level-membership-for-neurosurgery-category]
CHAPTER 31 Thorascopic Spine Surgery
The applications of endoscopic spine surgery have been expanded since the first publications spanning nearly two decades.1–6 Operating techniques have been standardized and unified and today are safe procedures with low complication rates that are comparable to those of open procedures, presuming the existence of adequate training and manual skills of the surgeon.7 Thus, endoscopic operations on the spinal column no longer represent exceptional interventions but have become standard procedures in spine surgery. Thoracoscopic techniques can be used to approach the anterior column of the spine in the area between the third thoracic vertebra and the third lumbar vertebra because endoscopic splitting of the diaphragm also allows the exposure of the upper sections of the lumbar spine. The application potential includes anterior release procedures, with incision and resection of ligaments and intervertebral disks; removal of fragmented disks or sections of vertebrae, including anterior decompression of the spinal canal; replacement of vertebral bodies with biologic or alloplastic materials; and ventral stabilization procedures with implants designed for use in endoscopic spine surgery. In addition, percutaneous endoscopic techniques are used for minimally invasive treatment of degenerative disk disease of the thoracic and lumbar spine.
Indications
Overall, the range of indications for the technique described here can be defined as follows:
Technical Requirements
Image Transmission
The key to any endoscopic technique is image recording and transmission. “You will do what you can see,” and therefore true high-definition video technique has also revolutionized the endoscopic technique, which now provides an endoscopic view comparable to images that the microscope is able to provide. A high-intensity xenon light source is required to illuminate the thoracic cavity. A rigid, long, 30-degree scope enables positioning of the camera far away from the working portal, thus facilitating undisturbed working and variable adjustment of the angle of vision. The intraoperative view is transmitted onto two or three flat screens (Fig. 31-1).
Instruments
Complete sets of instruments for soft tissue and bone preparation are manufactured by contemporary instrument manufacturers (Fig. 31-2). Instruments should have a nonreflective surface and a depth scale on both sides and be ergonomically designed with big handles for safe control and handling. The technique by which they are used is called the three-point anchoring technique, which means that every sharp and potentially dangerous instrument is guided by both hands; one hand is based on the chest wall, always controlling and sometimes neutralizing unexpected forces and movements of the instrument (see Video 31-9).
Implants
Several implants for anterior instrumentation that can be used for endoscopic, mini-open, or open spine surgery are now available. Most of them are based on the principle of a cannulated screw and plate system, first allowing the implantation of K wires under fluoroscopic control to be used as landmarks, followed by the insertion of screws. Biomechanically tested four-point fixation implants provide adequate angular stability, which is necessary for single anterior instrumentation (Fig. 31-3).13
For vertebral body replacement, bone graft (autograft or allograft) or mechanical devices can be used and filled or surrounded with the autologous bone harvested from the corpectomy site. A wide variety of expandable titanium cages is currently available.14
Preoperative Requirements
Education of the Patient
The patient should be informed about the following approach-specific risks and hazards:
Marking the Portals
As a routine, four portals are used: scope portal, working portal, suction-irrigation portal, and retractor portal (Video 31-2). Their location and, in particular, the position of the working portal are crucial for the endoscopic operation to proceed in the optimal fashion. For this reason, the lesion is first displayed in the lateral projection (with reference to the patient’s body) under precise adjustment of the image intensifier, and a marker is used to draw the injured spinal section onto the lateral thoracic wall (Fig. 31-4). The working portal is drawn in directly above the lesion. The trocar for the endoscope is marked either caudal or cranial to the working portal, depending on the height of the lesion, and following the axis of the spine. The distance from the working portal is approximately two intercostal spaces. The entry points for suction and irrigation and for the retractor are then located ventral from these portals.
Operative Techniques
Approach to the Thoracolumbar Junction
This operation is also performed using single-lung ventilation (Video 31-4).8,11,15,16 Here, too, the approach side is decided by the location of the major vessels, which can be identified from the preoperative computed tomographic scan. In most cases, the best approach to the thoracolumbar junction is from the left. Placement of the trocars and instruments is illustrated in Figure 31-5.
FIGURE 31-5 Placement of the trocars and instruments for an endoscopic intervention at the thoracolumbar spine.
The dome-like diaphragm is firmly connected at its margins with the sternum, ribs, and spine and arches up into the thoracic cavity. Topographically speaking, the attachment sites of the diaphragm to the spine are at the level of the first lumbar vertebra, whereas the lowest point of the thoracic cavity projects with the phrenicocostal sinus at the level of the baseplate of the second lumbar vertebra (Fig. 31-6). This makes it possible to place a trocar intrathoracically in the phrenicocostal sinus, which, after incision of the diaphragm attachment to the spine, provides access to the retroperitoneal section of the thoracolumbar junction down to the baseplate of the second lumbar vertebra. This requires a 4- to 5-cm–long incision following the attachment of the diaphragm; access to the L1-2 intervertebral disk can be obtained with a shorter incision of 2 to 3 cm (Fig. 31-7).15–17
