[level-membership-for-orthopaedics-category]CHAPTER 7
THORACIC SPINE

SELECTED MOVEMENTS

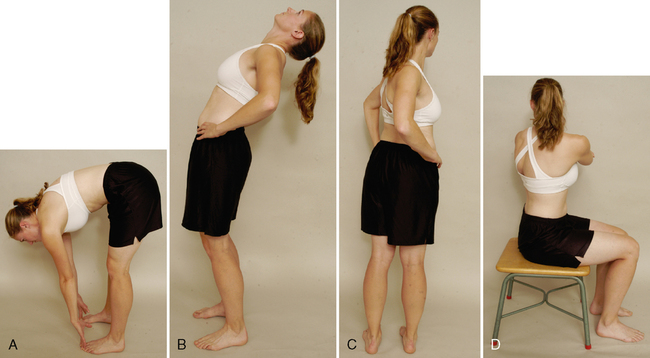
Method 1. Because the ROM at each vertebra is difficult to measure, the examiner can use a tape measure to derive an indication of overall movement. The examiner first measures the length of the spine from the C7 spinous process to the T12 spinous process with the patient in the normal standing posture. The patient then is asked to bend forward, and the spine is again measured.
Method 2. If the examiner wishes, the spine may be measured from the C7 to the S1 spinous processes with the patient in the normal standing position. The patient then is asked to bend forward, and the spine is again measured. In this case, the examiner is measuring movement in the lumbar spine as well as in the thoracic spine.
INDICATIONS OF A POSITIVE TEST
The normal ROM of forward flexion (forward bending) in the thoracic spine is 20° to 45°.
• An alternative test method involves having the patient bend forward and try to touch the toes while keeping the knees straight. The examiner then measures from the fingertips to the floor and records the distance. With this method, the examiner must keep in mind that, in addition to the thoracic spine movement, movement also may occur in the lumbar spine and hips; in fact, movement could occur totally in the hips.
• Each of the methods described is indirect. Measurement of the ROM at each vertebral segment requires a series of radiographs. The examiner can decide which method to use. It is of primary importance, however, to note on the patient’s chart how the measuring was done and which reference points were used.
• While the patient is flexed forward, the examiner can observe the spine from the “skyline” view. With nonstructural scoliosis, the scoliotic curve disappears on forward flexion; with structural scoliosis, it remains. With the skyline view, the examiner is looking for a hump on one side (convex side of the curve) and a hollow on the other side (concave side of the curve). This “hump and hollow” sequence is caused by vertebral rotation in idiopathic scoliosis, which pushes the ribs and muscles out on one side and causes the paravertebral valley on the opposite side. The vertebral rotation is most evident in the flexed position.
• When the patient flexes forward, the thoracic spine should curve forward in a smooth, even manner with no rotation or side flexion. The examiner should look for any apparent tightness or sharp angulation, such as a gibbus (hump) when the movement is performed. If the patient has an excessive kyphosis to begin with, very little forward flexion movement occurs in the thoracic spine.
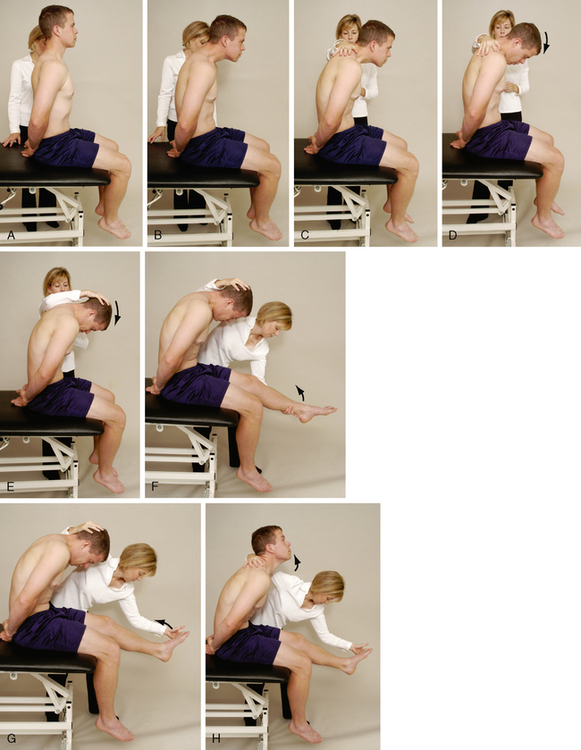
• McKenzie1 advocates testing flexion while the patient is sitting to reduce pelvic and hip movements. While sitting, the patient slouches forward, flexing the thoracic spine. The patient can put the hands around the neck to apply overpressure at the end of flexion. If symptoms arise from forward flexion on the spine with the neck flexed by the hands, the examiner should repeat the movement with the neck slightly extended and the hands removed. This can help differentiate between cervical and thoracic pain.
• Because extension occurs over 12 vertebrae, the movement between the individual vertebrae is difficult to detect visually.
• McKenzie1 advocates having the patient place the hands in the small of the back to add stability while performing the backward movement or to do extension while the patient is sitting or in the prone-lying (sphinx) position.
• As the patient extends, the thoracic curve should curve backward or at least straighten in a smooth, even manner with no rotation or side flexion.
• Lee2 advocates asking the patient to fully forward-flex the arms during extension to facilitate extension.
• The examiner should look for any apparent tightness or angulation when the movement is performed.
• If the patient shows excessive kyphosis, the kyphotic curvature remains on extension; that is, the thoracic spine remains flexed, whether the movement is tested while the patient is standing or lying prone.
• The test also may be done with the patient in the prone-lying position. If this position is used, the normal kyphotic posture should flatten. If it does not, the patient has a structural kyphosis.
• The examiner must remember that movement in the lumbar spine, as well as in the thoracic spine, is being measured with these movements.
• As the patient bends sideways, the spine should curve sideways in a smooth, even, sequential manner. The examiner should look for any tightness or abnormal angulation, which may indicate hypomobility or hypermobility at a specific segment when the movement is performed. On side flexion, if the ipsilateral paraspinal muscles tighten or their contracture is evident (Forestier’s bowstring sign), ankylosing spondylitis or a pathological condition causing muscle spasm should be considered.

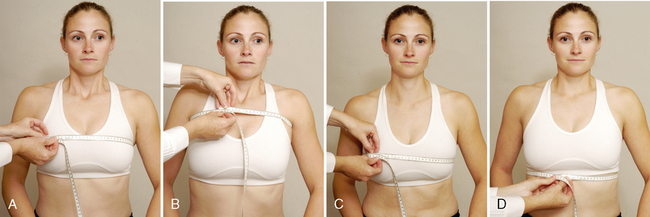
Method 1. Costovertebral joint movement usually is determined by measuring chest expansion. The examiner places the tape measure around the chest at the level of the fourth intercostal space. The patient is asked to exhale as much as possible, and the examiner takes a measurement. The patient then is asked to inhale as much as possible and to hold the breath while the second measurement is taken.
Method 2. Chest expansion also can be measured at three different levels. If this method is used, the examiner must take care to ensure that the levels of measurement are noted for consistency. The levels are (1) under the axillae for apical expansion, (2) at the nipple line or xiphisternal junction for midthoracic expansion, and (3) at the T10 rib level for lower thoracic expansion. The measurements are taken after expiration and inspiration.
INDICATIONS OF A POSITIVE TEST
The normal difference between inspiration and expiration is 3 to 7.5 cm (1 to 3 inches).
• After chest expansion has been measured, it is worthwhile to have the patient take a deep breath and cough so that the examiner can determine whether this action causes or alters any pain. If it does, the examiner may suspect a respiratory-related problem or a condition that is increasing intrathecal pressure in the spine.
• Evjenth and Gloeck3 have noted a way to differentiate thoracic spine and rib pain during movement. If pain is present on flexion, the patient is returned to neutral and asked to take a deep breath and hold it. While holding the breath, the patient flexes until pain is felt. At this point, the patient stops flexing and exhales. If further flexion can be accomplished after the exhale, the problem is more likely to be the ribs than the thoracic spine. Extension can be tested in a similar fashion.

Rib Movement During Respiration
• If a depressed rib is implicated, the highest restricted rib usually is the one that causes the greatest problem. If an elevated rib is present, the lowest restricted rib usually is the one that causes the greatest problem.
• Rib dysfunctions may be categorized as structural, torsional, or respiratory.
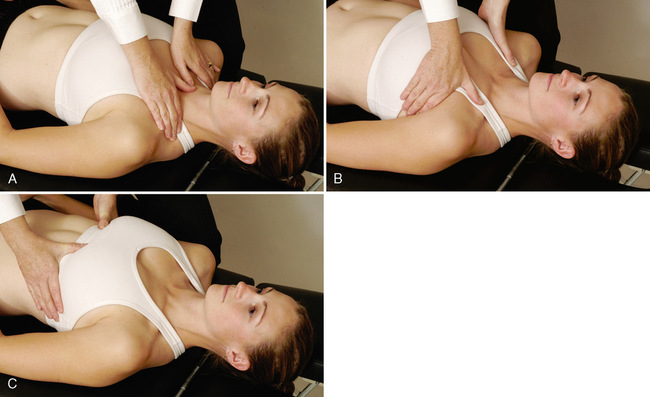
Rib Movement Relative to the Thoracic Spine
• Extension may be tested in a similar fashion, but the rib rotates posteriorly.
• To test lateral movement of the ribs, the examiner begins at the level of the axilla and works down the lateral aspect of the ribs, feeling the movement of the ribs during inspiration and expiration and noting any restriction.


Upper thoracic spine (C5-T3). The examiner places one hand on the patient’s forehead or on top of the head. With the other hand, the examiner palpates over and between the spinous processes of the lower cervical and upper thoracic spines, feeling for movement between the spinous processes. To test the movement properly, the examiner places the middle finger in the space (interspace) between two spinous processes. The index and ring fingers are placed over two adjacent spinous processes. The examiner then flexes, extends, side-flexes, and rotates the patient’s head while palpating for movement in the interspace. The examiner should feel the movement occurring, assess its quality, and note whether the movement is hypomobile or hypermobile relative to the adjacent vertebrae.
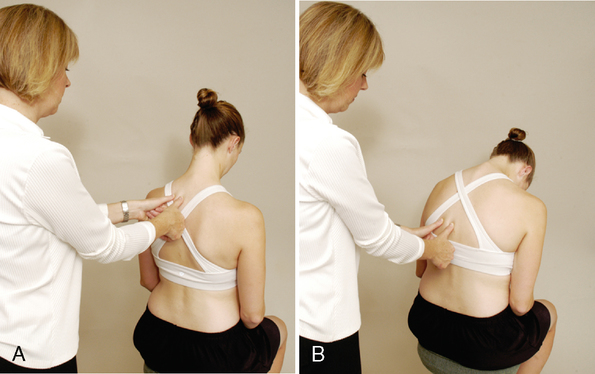
Lower thoracic spine (T3 and T11). The examiner places one hand and arm around the patient’s elbows while palpating over and between the spinous processes, as previously described. The examiner then flexes and extends the spine by lifting and lowering the patient’s elbows. Side flexion and rotation of the trunk may be performed in a similar fashion to test these movements. The patient sits with the hands clasped behind the head. The examiner uses the thumb on one side of the spinous process and/or the index finger and/or the middle finger on the other side to palpate just lateral to the interspinous space. For side flexion, the examiner moves the patient into right side flexion and then left side flexion and by palpation compares the amount and quality of right and left movement, including adjacent segments. For rotation, the examiner rotates the patient’s shoulders to the right or left, comparing by palpation the amount and quality of movement of each segment and that of adjacent segments.
• Because passive movements in the thoracic spine are difficult to perform in a gross fashion, the movement between each pair of vertebrae may be assessed.
• When the spinous processes are palpated, if one process appears to be out of alignment, the examiner can palpate the transverse processes on each side and compare them with the levels above and below to determine whether the vertebra is truly rotated or side-flexed. For example, if the spinous process of T5 is shifted to the right and if rotation has occurred at that level, the left transverse process would be more superficial posteriorly, whereas the right one would appear deeper. Spinous processes commonly are structurally abnormal, and as a result, the process may be deformed to the right or to the left. In this case the spinal segment would appear rotated, but in reality, the spinous process is structurally deformed. If the spinous process rotation is an anomaly, the transverse processes would be equal, as would the ribs.
• Palpating the transverse processes while the patient does passive or active movement of the spine helps indicate abnormal movement when the two sides are compared or when one level is compared with another. If the alignment is normal to begin with and becomes abnormal with movement or if it is abnormal to begin with and becomes normal with movement, this indicates a functional asymmetry rather than a structural one. Generally, a structural asymmetry remains through all movements.
SPECIAL TEST FOR NEUROLOGICAL DYSFUNCTION
Relevant Special Test
Slump test (sitting dural stretch test)
Epidemiology and Demographics
Thoracic disc herniation. The thoracic spine is reported to be the spinal region least likely to experience a disc herniation. The thoracic spine has been reported to account for 0.25% to 5% of intervertebral disc herniations. One in 1 million patients experiences symptoms of thoracic disc herniation every year. Of these patients, 2% have herniation at the lower thoracic spine (T11-T12), and 70% have herniation in a posterolateral direction. The age range for thoracic disc herniation has been reported to be 11 to 82 years, with a peak age of 40 to 50 years. The condition appears to occur more often in men than in women.6–9
Thoracic compression fracture. Spinal compression fractures occur in more than 750,000 people a year in the United States. About two thirds of spinal compression fractures are never diagnosed, because many patients and families think that back pain is merely a sign of aging and arthritis. Compression fractures are more prevalent in two groups of patients: the elderly, because of osteoporosis and an increased risk of falls; and young adults, as a result of trauma, such as motor vehicle accidents or a fall from a great height.10,11
T4 syndrome. The prevalence of this pathological condition is unknown. Those most prone to development of the syndrome are individuals over 35 years of age. The gender and cultural prevalence also are unknown.12–14
Relevant Signs and Symptoms
Thoracic disc herniation. Disc herniations in the thoracic spine may be asymptomatic. However, patients may complain of intermittent backache, thoracic root pain and paresthesia, and/or spinal cord compression symptoms.
Thoracic compression fracture. A patient with a thoracic compression fracture may complain of pain in the thoracic region over the affected vertebra. The symptoms may be described as severe, sharp, and exacerbated by motion. Pain is noted when the person lifts and carries objects or with breathing. The patient may or may not have signs of cord compression, depending on the magnitude of injury.
T4 syndrome. Patients with T4 syndrome complain of unilateral or bilateral paresthesia in all five hand digits, or in the whole hand, or in the forearm and hand (i.e., glove type [long/short]). The hands may feel hot or cold, swelling may be present, and the patient may complain that the arms feel heavy. Aches and pains may be present in a nondermatomal pattern. The patient may complain that the pain feels like a tight band around the arms. The person also may complain of a combination of neck, upper thoracic, and cranial pain, without abnormal neurological signs.
Mechanism of Injury
SLUMP TEST (SITTING DURAL STRETCH TEST)15–17 
• The uninvolved leg is always tested before the involved leg.
• Butler16 suggested that when the thoracic spine is tested with the patient in the slump position, trunk rotation left and right should be added to increase the stress on the intercostal nerves.
• With a positive test result, pain usually is produced at the site of the lesion.
• If bilateral symptoms are produced, the examiner must consider a myelopathy.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]CHAPTER 7
THORACIC SPINE
SELECTED MOVEMENTS
Method 1. Because the ROM at each vertebra is difficult to measure, the examiner can use a tape measure to derive an indication of overall movement. The examiner first measures the length of the spine from the C7 spinous process to the T12 spinous process with the patient in the normal standing posture. The patient then is asked to bend forward, and the spine is again measured.
Method 2. If the examiner wishes, the spine may be measured from the C7 to the S1 spinous processes with the patient in the normal standing position. The patient then is asked to bend forward, and the spine is again measured. In this case, the examiner is measuring movement in the lumbar spine as well as in the thoracic spine.
INDICATIONS OF A POSITIVE TEST
The normal ROM of forward flexion (forward bending) in the thoracic spine is 20° to 45°.
• An alternative test method involves having the patient bend forward and try to touch the toes while keeping the knees straight. The examiner then measures from the fingertips to the floor and records the distance. With this method, the examiner must keep in mind that, in addition to the thoracic spine movement, movement also may occur in the lumbar spine and hips; in fact, movement could occur totally in the hips.
• Each of the methods described is indirect. Measurement of the ROM at each vertebral segment requires a series of radiographs. The examiner can decide which method to use. It is of primary importance, however, to note on the patient’s chart how the measuring was done and which reference points were used.
• While the patient is flexed forward, the examiner can observe the spine from the “skyline” view. With nonstructural scoliosis, the scoliotic curve disappears on forward flexion; with structural scoliosis, it remains. With the skyline view, the examiner is looking for a hump on one side (convex side of the curve) and a hollow on the other side (concave side of the curve). This “hump and hollow” sequence is caused by vertebral rotation in idiopathic scoliosis, which pushes the ribs and muscles out on one side and causes the paravertebral valley on the opposite side. The vertebral rotation is most evident in the flexed position.
• When the patient flexes forward, the thoracic spine should curve forward in a smooth, even manner with no rotation or side flexion. The examiner should look for any apparent tightness or sharp angulation, such as a gibbus (hump) when the movement is performed. If the patient has an excessive kyphosis to begin with, very little forward flexion movement occurs in the thoracic spine.
• McKenzie1 advocates testing flexion while the patient is sitting to reduce pelvic and hip movements. While sitting, the patient slouches forward, flexing the thoracic spine. The patient can put the hands around the neck to apply overpressure at the end of flexion. If symptoms arise from forward flexion on the spine with the neck flexed by the hands, the examiner should repeat the movement with the neck slightly extended and the hands removed. This can help differentiate between cervical and thoracic pain.
• Because extension occurs over 12 vertebrae, the movement between the individual vertebrae is difficult to detect visually.
• McKenzie1 advocates having the patient place the hands in the small of the back to add stability while performing the backward movement or to do extension while the patient is sitting or in the prone-lying (sphinx) position.
• As the patient extends, the thoracic curve should curve backward or at least straighten in a smooth, even manner with no rotation or side flexion.
• Lee2 advocates asking the patient to fully forward-flex the arms during extension to facilitate extension.
• The examiner should look for any apparent tightness or angulation when the movement is performed.
• If the patient shows excessive kyphosis, the kyphotic curvature remains on extension; that is, the thoracic spine remains flexed, whether the movement is tested while the patient is standing or lying prone.
• The test also may be done with the patient in the prone-lying position. If this position is used, the normal kyphotic posture should flatten. If it does not, the patient has a structural kyphosis.
[/not-level-membership-for-orthopaedics-category]
