KNEE
SELECTED MOVEMENTS



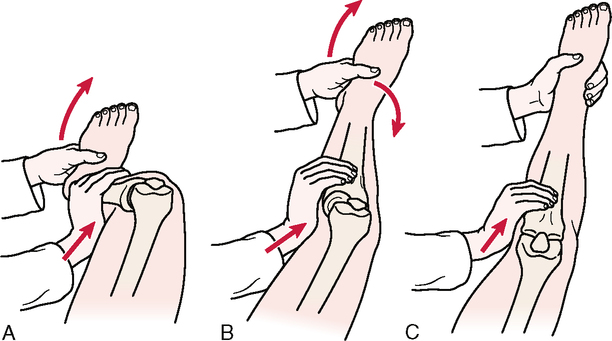
• When the patella is pushed medially or laterally, the examiner should note whether it stays parallel to the femoral condyles or tilts or rotates. For example, if the patella is pushed medially when the medial structures are tight, the lateral border of the patella tilts up. Likewise, with tight lateral structures, the medial border tilts up. If the lateral structures are tight superiorly, the inferior pole of the patella medially rotates. These are examples of dynamic tilt and rotation problems of the patella.
SPECIAL TESTS FOR ONE-PLANE MEDIAL INSTABILITY
Relevant Special Tests
Relevant Signs and Symptoms
• Mild to moderate knee pain is present.
• The patient reports feeling a tearing in the knee, not a “pop.”
• Bruising in the medial knee often is present, because the MCL/TCL is an extra-articular structure.
• Swelling builds up slowly over several days.
• The patient walks with a limp and has pain on knee extension, because extension stretches the ligament.
• Instability and “giving way” may be noted.
• Loss of knee motion and moderate stiffness may be present.
• Medial joint line pain or pain where the ligament attaches to the femur or tibia may be reported.
Mechanism of Injury
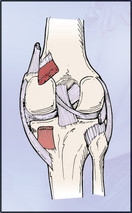
Avulsion of ligaments generally occurs between the unmineralized and mineralized fibrocartilage layers. MCL/TCL injury occurs most often at the femoral attachment (65% of cases).6–11
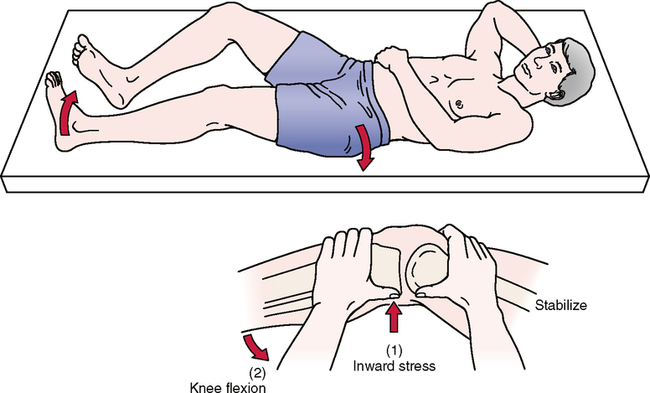
ABDUCTION (VALGUS STRESS) TEST12,13 

• A positive test result on full extension is classified as a major disruption of the knee. The examiner usually finds that one or more of the rotary tests also produce a positive result.
• If the examiner applies lateral rotation to the foot when performing the test in extension and finds excessive lateral rotation on the affected side, this is a sign of possible anteromedial rotary instability.
• The flexed part of the valgus stress test is considered the true test for one-plane medial instability, because the cruciates are eliminated.


SPECIAL TESTS FOR ONE-PLANE LATERAL INSTABILITY
Relevant Special Tests
Epidemiology and Demographics
Injury to the LCL/FCL is the least common knee ligament injury. Injuries to the LCL/FCL are rare, accounting for only 2% of all knee injuries. The LCL/FCL is the least likely knee ligament to be sprained, because most LCL/FCL injuries are caused by a blow to the inside of the knee, and that area usually is shielded by the opposite leg.6,7,9–11
Relevant Signs and Symptoms
• Mild to moderate knee pain is present.
• The patient may report feeling a pop in the knee.
• Loss of knee motion and moderate stiffness are present.
• Lateral joint line pain may be reported.
• Bruising in the lateral knee often is present, because the LCL/FCL is an extra-articular structure.
Mechanism of Injury
Avulsion of ligaments generally occurs between the unmineralized and mineralized fibrocartilage layers. LCL/FCL injury occurs most commonly at the fibular attachment (75% of cases).6,7,9–11

• The examiner may also find that one or more of the rotary instability tests produce a positive result, especially if the test is positive in extension.
• The flexed part of the varus stress test is classified as the true test for one-plane lateral instability.
• If Hughston’s valgus stress test is performed, the examiner can rest the patient’s thigh on the plinth, which often allows the patient to relax more and is likely to lead to less muscle spasm.
SPECIAL TESTS FOR ONE-PLANE POSTERIOR INSTABILITY
Relevant Special Tests
Posterior sag sign (gravity drawer test)
Drawer sign (see Special Tests for One-Plane Anterior Instability)
Active drawer test (see Special Tests for One-Plane Anterior Instability)
Relevant Signs and Symptoms
Mechanism of Injury
Hyperextension alone may lead to an avulsion injury of the PCL from the origin; this kind of injury may be amenable to repair. An anterior force to the anterior tibia in a hyperextended knee with the foot planted results in combined injury to the knee ligaments, along with knee dislocation.5–7,10,11,14–17
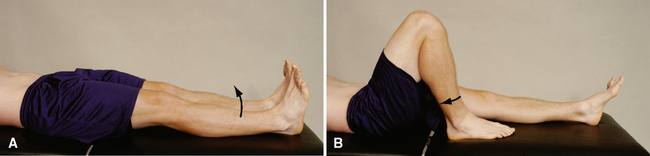
POSTERIOR SAG SIGN (GRAVITY DRAWER TEST)18–22 
• This test should always be done first when testing the cruciates to prevent a false positive test when doing the test for the anterior cruciate.
• If the patient tests positive for the posterior sag sign, the individual should carefully extend the knee while the examiner holds the hip in 90° to 100° of flexion. This action is sometimes called the voluntary anterior drawer sign, and the results are similar to those of the active anterior drawer test. As the patient slowly extends the knee, the tibial plateau moves or shifts forward to its normal position, indicating that the tibia previously was posteriorly subluxated (posterior cruciate tear) on the femur.


• The examiner should be cautious of a false-positive test result if the anterior cruciate ligament has been torn, because gravity may cause an anterior shift.
• This test is not as accurate for the posterior cruciate ligament as is the posterior drawer or sag test; when the posterior cruciate ligament is torn, the greatest posterior displacement is at 90°.
• In the case of acute trauma, swelling prevents the examiner from getting a true indication of the joint’s mobility. The best time to assess joint laxity is immediately after an injury, before swelling occurs, or in the chronic state. The examiner may need to allow time for the swelling to reduce before true joint mobility can be assessed.


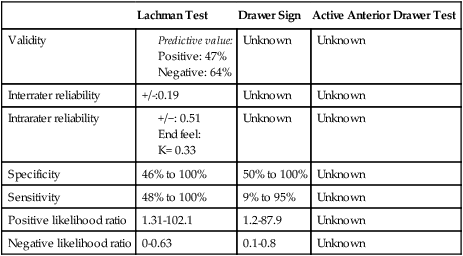
SPECIAL TESTS FOR ONE-PLANE ANTERIOR INSTABILITY
Relevant Special Tests

Adler and associates54 described a modification of this method, which they called the “drop leg Lachman test.” The patient lies supine. The test leg is abducted off the side of the examining table, and the knee is flexed to 25°. One of the examiner’s hands stabilizes the femur against the table while the patient’s foot is held between the examiner’s knees. The examiner’s other hand then is free to apply the anterior translation force. These researchers found that greater anterior laxity was demonstrated by this version of the test than by the classic version. The two legs are compared.
• Many contend that the Lachman test (also known as the Ritchie, Trillat, or Lachman-Trillat test), is the best indicator of injury to the anterior cruciate ligament, especially the posterolateral band, although this has been questioned.26
• The modification method that works for the examiner and that the examiner can use competently should be selected.
• Frank52 reported that to achieve the best results, the tibia should be slightly laterally rotated and the anterior tibial translation force should be applied from the posteromedial aspect. The hand on the tibia should apply the translation force.
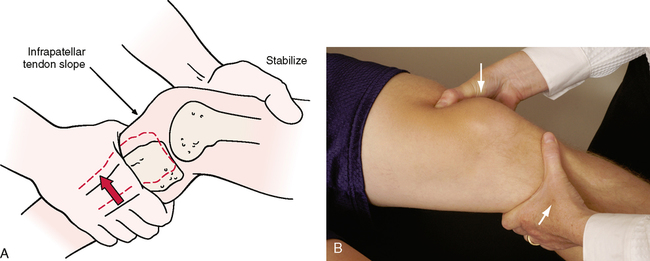
• The Lachman test can be done a number of ways. The key is to make sure the patient relaxes and the knee is held between full extension and 30º of flexion (see Orthopedic Physical Assessment, fifth edition, pages 767-770, for details).
• With acute trauma, swelling prevents the examiner from getting a true indication of the joint’s mobility. The best time to assess joint laxity is immediately after the injury, before swelling occurs, or in the chronic state. The examiner may need to allow time for swelling to reduce before true joint mobility can be assessed.
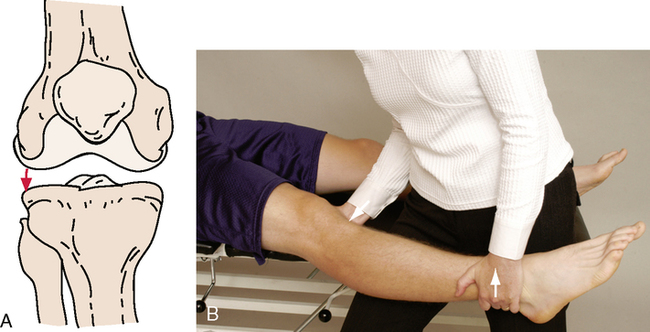
DRAWER SIGN12,23–25,27,28,30,33,34,37,39–47,55–59 

This part of the test assesses for one-plane anterior instability
INDICATIONS OF A POSITIVE TEST
The normal amount of anterior movement that should be present is approximately 6 mm.
• This examination must be performed with particular care, because the start position could result in a false-positive anterior drawer test result for the anterior cruciate ligament if a posterior sag (an indication of a posterior cruciate problem) goes unnoticed before the test is started. If minimal or no swelling is present, the sag is evident because of an obvious concavity distal to the patella.
• If only the anterior cruciate ligament is torn, the test result is negative, because other structures (posterior capsule and posterolateral and posteromedial structures) limit movement. In addition, hemarthrosis, a torn medial meniscus (posterior horn) wedged against the medial femoral condyle, or hamstring spasm may result in a false-negative test result. Hughston12 points out that tearing of the coronary or meniscotibial ligament can allow the tibia to translate forward more than normal, even with an intact anterior cruciate ligament. In this case, when the anterior drawer test is performed, anteromedial rotation (subluxation) of the tibia occurs.
• When the anterior drawer test is done, if an audible snap or palpable jerk (Finochietto jumping sign) occurs when the tibia is pulled forward, and the tibia moves forward excessively, a meniscal lesion is likely in addition to the torn anterior cruciate ligament.23
• Weatherwax58 described a modified means of testing the anterior drawer (90-90 anterior drawer test). The patient lies supine. The examiner flexes the patient’s hip and knee to 90° and supports the lower leg between the examiner’s trunk and forearm. The examiner places the hands around the tibia, as with the standard test, and applies sufficient force to slowly lift the patient’s buttock off the table.
• Feagin59 recommended that the drawer test be done with the patient sitting with the leg hanging relaxed over the end of the examining table (sitting anterior drawer test). The examiner places the hands as with the standardized test and slowly draws the tibia first forward and then backward to test the anterior and posterior drawer. The examiner uses the thumbs to palpate the tibial plateau movement relative to the femur. The examiner also may note any rotational deformity. The advantage of doing the test this way is that the posterior sag is eliminated, because the effect of gravity is eliminated.
This part of the test assesses one-plane posterior instability.
• The difficulty with this test is in determining the neutral starting position if the ligaments have been injured.
• As with the Lachman test, swelling in the joint affects the examiner’s ability to assess for joint laxity.
• If the arcuate-popliteus complex remains intact, a positive posterior drawer sign may not be elicited.
• When the tibia is pushed backward, if the examiner forcefully rotates it laterally and excessive movement occurs, the test result is positive for posterolateral instability. Warren57 calls this maneuver the arcuate spin test.


• A second part of the test may be done by having the patient contract the hamstrings isometrically so that the tibial plateau moves posteriorly. This part of the test accentuates the posterior sag for posterior cruciate insufficiency, if present, and ensures maximum movement for anterior cruciate insufficiency if a quadriceps contraction is tried a second time.
• The active drawer test is a better expression of posterior cruciate insufficiency than of anterior cruciate insufficiency.
• With the drawer sign or test, if the anterior or posterior cruciate ligament is torn (third-degree sprain), some rotary instability is evident when the appropriate ligamentous tests are performed.
SPECIAL TESTS FOR ANTEROLATERAL ROTARY INSTABILITY
Relevant Special Tests
• Lateral pivot shift maneuver (test of MacIntosh)
Mechanism of Injury
See the anterior cruciate injury.
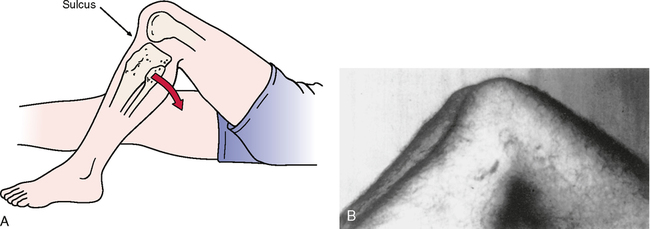
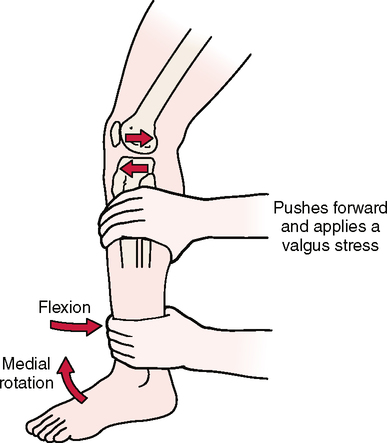
LATERAL PIVOT-SHIFT MANEUVER (TEST OF MACINTOSH)26,32,34,37,38,62–64 
• During the test, the tibia moves away from the femur on the lateral side (but rotates medially) and moves anteriorly in relation to the femur.
• Normally, the knee’s center of rotation changes constantly through its ROM because of the shape of the femoral condyles, ligamentous restraint, and muscle tension. The path of movement of the tibia on the femur is described as a combination of rolling and sliding, with rolling predominating when the instant center is near the joint line and sliding predominating when the instant center shifts distally from the contact area.
• The lateral pivot-shift maneuver (MacIntosh test) is a duplication of the anterior subluxation-reduction phenomenon that occurs during the normal gait cycle when the anterior cruciate ligament is torn. Therefore, the test illustrates a dynamic subluxation. This shift occurs between 20° and 40° of flexion (0° being full extension). This is the phenomenon that prompts patients to give the clinical description of feeling the knee “give way.”
• Like most provocative tests, the lateral pivot-shift test (MacIntosh test) does have a disadvantage. Because of the forces applied during the test, in an apprehensive patient protective muscle contraction may lead to a false-negative test result.
• Hoher et al.64 modified the original position (lateral pivot-shift test) to slight lateral rotation, because they believed that lateral tibial rotation gives a more pronounced pivot shift when the test result is positive. In slight flexion, the secondary restraints (i.e., hamstrings, lateral femoral condyle, lateral meniscus) are less efficient than in full flexion. It is important to realize that subluxation does not occur in full extension because of the “locking home” of the tibia on the femur. With slight flexion, however, the secondary restraints are less restrictive, and subluxation occurs. The examiner then applies a valgus stress to the knee while maintaining a medial rotation torque on the tibia at the ankle.