CHAPTER 94 Thoracic Aortic Trauma
THORACIC AORTIC TRAUMA
Etiology and Pathophysiology
Blunt aortic trauma is caused by a severe deceleration injury. The aortic arch is relatively fixed to the thoracic inlet by the brachiocephalic vessels, whereas the ascending and descending aorta are relatively mobile. During deceleration, horizontal shear forces act unequally on the relatively fixed arch and mobile ascending and descending aorta, causing extreme stress on the points of attachment of the aorta, namely, the aortic root and aortic isthmus, rendering these sites susceptible to transection (Fig. 94-1).1 In addition, rapid deceleration may cause the vertebral column, sternum, first rib, and clavicle to compress the aorta in the region of the isthmus, contributing to the mechanism of injury.2

 FIGURE 94-1
FIGURE 94-1In clinical practice, the aortic isthmus is by far the most common site of aortic injury; the aortic root and ascending aorta represent 5% or less of cases (Fig. 94-2). However, in autopsy series, the ascending aorta is involved in 25% of cases.3 This discrepancy is explained by the fact that many patients with ascending aortic injury do not survive to reach the hospital or are not stable enough for imaging because of grave complications of ascending aortic trauma, such as hemopericardium with tamponade, disruption of the aortic valve, and coronary artery dissection.
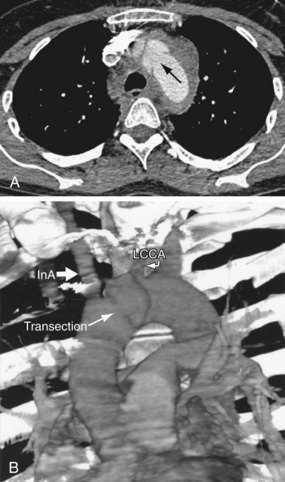
 FIGURE 94-2
FIGURE 94-2The degree of traumatic aortic injury depends on the nature of disruption of the aortic wall. Potential aortic injuries range from intimal hemorrhage, through intimal laceration and medial laceration, to complete laceration of the aorta.1 Disruption of the intima and media results in a pseudoaneurysm. Complete laceration, with disruption of the adventitia, usually results in immediate death.
Manifestations of Disease
Imaging Techniques and Findings
Radiography
Plain film findings associated with aortic trauma include a widened mediastinal contour, obscuration of the aortic arch or descending aortic margin, displacement of the trachea or of a nasogastric tube (if present) to the right, and left apical cap (Fig. 94-3). Fracture of the first or second ribs may be seen as a result of the causative trauma.4 However, each of these findings has been shown to have poor sensitivity or poor specificity. For example, in the trauma setting, a widened mediastinum is more commonly explained by anteroposterior positioning, lung contusion, hemothorax, and venous mediastinal bleeding, decreasing the specificity of these findings. Furthermore, in the majority of aortic injuries, the adventitia remains intact, resulting in only mild radiographic mediastinal findings, decreasing the sensitivity of plain radiography. In one study of aortic trauma, 44% of patients with subsequently proven aortic injury had a normal chest radiograph.5 Therefore, plain radiography is not sufficiently sensitive or specific for the evaluation of aortic injury, and in the correct clinical setting, the patient should proceed directly to other modes of imaging.
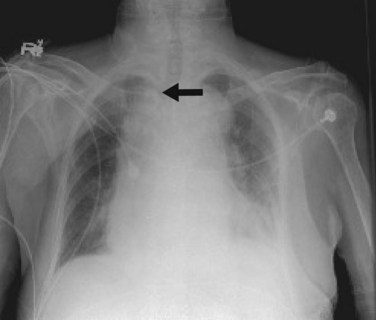
 FIGURE 94-3
FIGURE 94-3Computed Tomography
Multidetector computed tomography (MDCT) is the definitive modality for diagnosis of aortic trauma because of its speed, accuracy, postprocessing advantages, and ability to simultaneously evaluate the whole body for traumatic injury. CT angiography has been shown to have 100% sensitivity and 100% negative predictive value for traumatic aortic injury, at lower cost and with fewer complications than by catheter angiography.6
Aortic Pseudoaneurysm
Most patients with aortic trauma who survive to imaging will have a partial tear of the aortic wall. If the intima and media are torn but the adventitia remains intact, blood is forced between the layers, causing formation of a pseudoaneurysm. The imaging appearance is of a rounded bulge projecting from the aorta (Fig. 94-4). The margins are typically irregular, and there is often an intimal flap that forms a “collar” at the neck of the pseudoaneurysm. Note that the injury to the intima may extend several centimeters proximal or distal to the visualized pseudoaneurysm. The extent of the injury, especially the proximal extent, is crucial in the planning of repair because branch vessel involvement has a major influence on repair technique.
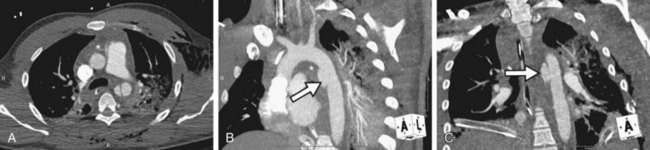
 FIGURE 94-4
FIGURE 94-4Periaortic Mediastinal Hemorrhage
Mediastinal hemorrhage is an indirect sign of thoracic aortic trauma, being attributable to aortic injury in only 12.5% of cases.7 Arterial disruption of one of the great thoracic vessels with active contrast extravasation from the vessel into the hematoma represents a potentially catastrophic injury in which the patient would be highly unstable. Traumatic mediastinal hemorrhage, however, is most commonly caused by rupture of small mediastinal veins.
The location of mediastinal hematoma is a guide to its cause. Hematoma abutting the sternum or vertebral body should suggest fracture. Likewise, hematoma surrounding the aorta should provoke a thorough evaluation of the aorta for direct signs of injury (Fig. 94-5). Nevertheless, an isolated finding of mediastinal hemorrhage, even if it is periaortic, is unlikely to be accompanied by aortic injury if no direct sign of aortic injury is seen.8 In addition, mediastinal hematoma can track inferiorly. The presence of retrocrural hematoma on an abdominal CT image should prompt careful evaluation of the thorax for vascular injury.

 FIGURE 94-5
FIGURE 94-5Contrast Agent Extravasation
On CT, the extravasation of contrast agent from an aortic injury is diagnosed by the presence of high-density streaks or puddles within a mediastinal hematoma, but it is a very rare finding. Such patients are extremely unstable. In one series of four patients with contrast agent extravasation from thoracic aortic trauma, none survived.9
Magnetic Resonance
MR can be used to depict the findings of aortic trauma (Fig. 94-6). However, the typically longer duration of the examination (relative to CT), difficulty of monitoring the patient, and relative lack of 24-hour emergent availability combine to exclude MR in most cases from evaluation for acute traumatic aortic injury. In equivocal or unusual cases, MR can be an effective problem-solving tool. The diagnosis of very small pseudoaneurysms and intimal flaps, moreover, can be challenging on MR because of the generally inferior spatial resolution compared with MDCT (Fig. 94-7).

 FIGURE 94-6
FIGURE 94-6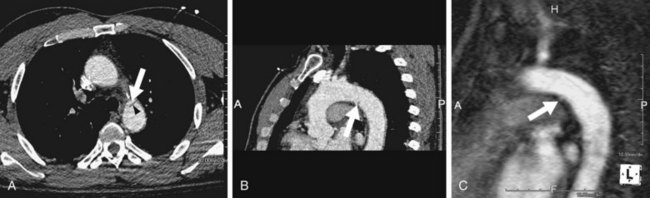
 FIGURE 94-7
FIGURE 94-7In rare patients, severe associated traumatic injuries preclude acute treatment of an aortic injury, and a chronic pseudoaneurysm develops that may be managed conservatively. MR is an appropriate modality for close imaging follow-up of these patients (Fig. 94-8). Key sequences include ECG-gated cine steady-state free precession, three-dimensional steady-state free precession MR angiography, and gadolinium-enhanced three-dimensional MR angiography of the chest. ECG gating is particularly helpful for evaluation of the aortic root.
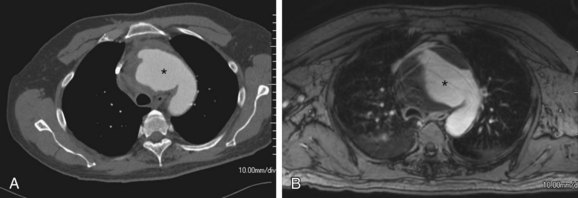
 FIGURE 94-8
FIGURE 94-8Nuclear Medicine/Positron Emission Tomography
Nuclear medicine/positron emission tomography has no role in evaluation of aortic trauma.
Differential Diagnosis
Ductus Diverticulum
The ligamentum arteriosum, the remnant of the ductus arteriosus, inserts along the anterior undersurface of the aortic isthmus. At this location, a common variant is a small anterior bulge of the aortic lumen, known as a ductus bump or ductus diverticulum. A ductus diverticulum (Fig. 94-9) demonstrates a smooth contour and obtuse angles with the aortic wall and is distinct from the appearance of an aortic intimal tear with pseudoaneurysm (Fig. 94-10), in which there are acute angles and often an irregular contour.

 FIGURE 94-9
FIGURE 94-9
 FIGURE 94-10
FIGURE 94-10Synopsis of Treatment Options
Medical
Identification of aortic injury is critical; 40% of patients who survive to reach the emergency department but are not diagnosed will die within 24 hours.6 There is no role for medical management of traumatic aortic injury. However, a patient will occasionally present with an enlarging aortic pseudoaneurysm years after a traumatic event (Fig. 94-11). This is due to either a rare case of survival of a missed minor traumatic aortic injury or a known injury that was not treated surgically because of severe concomitant injury. Over time, there is gradual progression from intimal tear to pseudoaneurysm. Intervention will usually be required. In other cases, the presenting feature of a missed aortic injury may be due to thrombus formation on the damaged intima, which introduces the potential complication of distal embolization.

 FIGURE 94-11
FIGURE 94-11Surgical/Interventional
The standard therapy for traumatic aortic injury is surgical repair. The surgical approach is commonly through a left lateral thoracotomy, although unusual sites of aortic injury may require an alternative approach. For example, a mid-arch dissection may be more easily approached through a median sternotomy.10 An open repair is associated with high morbidity and mortality, not least due to the usually extensive accompanying injuries. Emergent surgical repair carries a 15% to 50% mortality rate.11–13 The recent introduction of endovascular techniques to treat these patients has led to a reduced mortality rate and has also enabled the treatment of patients who are not candidates for open thoracic surgery. Recent data demonstrate that use of endovascular techniques in place of open repair in aortic trauma has increased from 0% to 64% of cases from 1997 to 2007, with concomitant reduction by more than 50% in mortality and paraplegia rates.14,15
Endovascular stent graft placement requires a proximal aortic neck of at least 15 mm for safe graft attachment (Fig. 94-12). In the case of aortic isthmus injury, the lesion is frequently too close to the left subclavian artery to provide a suitable attachment site (“landing zone”) for the stent graft. In this case, the left subclavian artery may be intentionally covered, provided patency of both vertebral arteries can be demonstrated before graft placement as the vertebral arteries enable collateral filling of the subclavian artery (i.e., left subclavian “steal” filling through left vertebral artery). In most patients, this will suffice. If vertebrobasilar or arm ischemia develops, a carotid-subclavian transposition or shunt can be performed.16
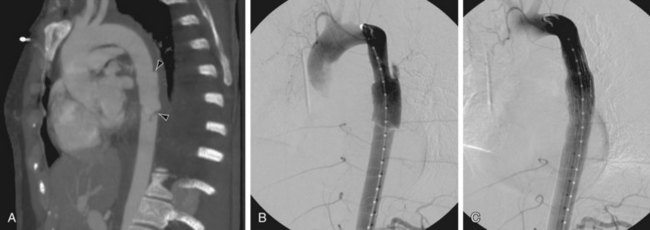
 FIGURE 94-12
FIGURE 94-12



Alkadhi H, Wildermuth S, Desbiolles L, et al. Vascular emergencies of the thorax after blunt and iatrogenic trauma: multi-detector row CT and three-dimensional imaging. Radiographics. 2004;24:1239-1255.
Brinkman WT, Szeto WY, Bavaria JE. Overview of great vessel trauma. Thorac Surg Clin. 2007;17:95-108.
Fattori R, Buttazzi K, Russo V, et al. Evolving concepts in the treatment of traumatic aortic injury. A review article. J Cardiovasc Surg (Torino). 2007;48:625-631.
Fisher RG, Sanchez-Torres M, Whigham CJ, et al. “Lumps” and “bumps” that mimic acute aortic and brachiocephalic vessel injury. Radioraphics. 1997;17:825-834.
Hoffer E, Forauer A, Silas A, Gemery JM. Endovascular stent-graft or open surgical repair for blunt thoracic aortic trauma: systematic review. J Vasc Interv Radiol. 2008;19:1153-1164. Epub 2008 Jun 27
Mirvis SE, Shanmuganathan K. Diagnosis of blunt traumatic aortic injury 2007: still a nemesis. Eur J Radiol. 2007;64:27-40.
Nzewi O, Slight RD, Zamvar V. Management of blunt thoracic aortic injury. Eur J Vasc Endovasc Surg. 2006;31:18-27.
Walsh SR, Tang TY, Sadat U, et al. Endovascular stenting versus open surgery for thoracic aortic disease: systematic review and meta-analysis of perioperative results. J Vasc Surg. 2008;47:1094-1098.
1 Parmley LF, Mattingly TW, Manion WC, et al. Non-penetrating traumatic injury of the aorta. Circulation. 1958;17:1086-1101.
2 Crass JR, Cohen AM, Motta AO, et al. A proposed new mechanism of traumatic aortic rupture: the osseous pinch. Radiology. 1990;176:645-649.
3 Groskin SA. Selected topics in chest trauma. Radiology. 1992;183:605-617.
4 Creasy JD, Chiles C, Routh WD, et al. Overview of traumatic injury of the thoracic aorta. Radiographics. 1997;17:27-45.
5 Demetriades D, Gomez H, Velmahos GC, et al. Routine helical computed tomographic evaluation of the mediastinum in high-risk blunt trauma patients. Arch Surg. 1998;133:1084-1088.
6 Dyer DS, Moore EE, Mestek MF, et al. Can chest CT be used to exclude aortic injury? Radiology. 1999;213:195-202.
7 Sandor F. Incidence and significance of traumatic mediastinal hematoma. Thorax. 1967;22:43-62.
8 Sammer M, Wang E, Blackmore CC, et al. Indeterminate CT angiography in blunt thoracic trauma: is CT angiography enough? AJR Am J Roentgenol. 2007;189:603-608.
9 Mirvis SE, Shanmuganathan K. Diagnosis of blunt traumatic aortic injury 2007: still a nemesis. Eur J Radiol. 2007;64:27-40.
10 Leshnower BG, Litt HI, Gleason TG. Anterior approach to traumatic mid aortic arch transection. Ann Thorac Surg. 2006;81:343-345.
11 Lamme B, de Jonge IC, Reekers JA, et al. Endovascular treatment of thoracic aortic pathology: feasibility and mid-term results. Eur J Vasc Endovasc Surg. 2003;25:532-539.
12 Kato N, Dake MD, Miller DC, et al. Traumatic thoracic aortic aneurysm: treatment with endovascular-stent grafts. Radiology. 1997;205:657-662.
13 Kasirajan K, Hefferman D, Langsfeld M. Acute thoracic aortic trauma: a comparison of endoluminal stent grafts with open repair and non-operative management. Ann Vasc Surg. 2003;17:589-595.
14 Hoffer E, Forauer A, Silas A, Gemery JM. Endovascular stent-graft or open surgical repair for blunt thoracic aortic trauma: systematic review. J Vasc Interv Radiol. 2008;19:1153-1164. Epub 2008 Jun 27
15 Demetriades D, Velmahos GC, Scalea TM, et al. Diagnosis and treatment of blunt thoracic aortic injuries: changing perspectives. J Trauma. 2008;64:1415-1418.
16 Gonzalo G, Fernández-Velilla M, Martí M, et al. Endovascular stent-graft treatment of thoracic aortic disease. Radiographics. 2005;25:S229-S244.
