CHAPTER 2 Theoretical Foundations of Developmental-Behavioral Pediatrics
What is the role of “theory” in the field of developmental-behavioral pediatrics? To answer this question, it is useful to imagine how clinical work and research endeavors would be affected if there were no theoretical or conceptual models to explain observed phenomena in practice or in research. Without conceptual models, practitioners would have no basis for suggesting specific interventions or understanding why some interventions are successful and why others fail. More to the point, practitioners would not be able to explain to families why certain recommendations are indicated or why the suggested interventions are likely to be helpful. In discussing nonadherence to treatments for chronic illness, Riekert and Drotar1 argued that conceptual models serve several purposes for the practitioner. Specifically, these models (1) guide the practitioner in the information gathering process, (2) guide communications between patients and practitioners, (3) aid the practitioner in determining the goals and targets of interventions, and (4) help the practitioner anticipate potential barriers to treatment success.
In the absence of theory, pediatricians may be inclined to develop new interventions for each specific physical condition and may assume that mechanisms that underlie certain difficulties are unique for each illness group. For example, without a general guiding theory, medical adherence issues for asthma may be treated entirely differently from medical adherence issues for type 1 diabetes. Alternatively, available developmentally oriented, family-based theories of medical adherence would indicate that similar processes underlie medical adherence across populations and that an intervention that works well for one illness may also work well for a different population. For example, on the basis of theory, a developmental-behavioral pediatrician may suggest that families make developmentally gauged changes in how responsibilities for adherence to aspects of the medical regimen are shared between parent and child, particularly as the child begins to transition into early adolescence.2
With theoretical frameworks, researchers would be more able to generate testable hypotheses or determine which variables are critical and should be examined in the context of their research programs. Indeed, a conceptual model facilitates the development of a program of research (as opposed to a set of unrelated studies), and it drives all aspects of the research endeavor, including participant selection, the design of the study, specification of independent and dependent variables, specification of relationships between variables, data-analytic strategies, and potential recommendations for clinical practice.1,3
The goal of this chapter is to demonstrate the importance of theory development and the role of conceptual models in the field of developmental-behavioral pediatrics. Throughout, we take the “developmental” aspect of developmental-behavioral pediatrics very seriously. Indeed, an exciting but also challenging aspect of studying and providing clinical services to children is that they are developmental “moving targets.” Moreover, the course of developmental change varies across individuals, so that two children who are the same age may differ dramatically with regard to neurological, physical, cognitive, emotional, and social functioning.4 For example, two 12-year-old boys may differ dramatically with regard to pubertal status, one boy being prepubertal and the other experiencing the latter stages of pubertal development; such interindividual differences have significant effects on their physical and social functioning. Similarly, consider two 9-year-old girls, one of whom is functioning at a lower level of cognitive ability. The child with more cognitive impairment may misinterpret social cues from her peers and fail to express her emotions verbally, which results in aggression with peers. The other 9-year-old child may respond to challenging social situations by questioning her peer and verbally expressing her feelings in a socially appropriate manner. It is also the case that the same behaviors that are developmentally normative at a younger age are often developmentally atypical at a later age.5 For example, temper tantrums may be an expected outcome when a young child lacks the language abilities to express his or her frustration. In older children, and after language skills develop, tantrums are expected to be less likely. Frequent tantrums in an older child would be considered atypical.
In attempting to understand better such developmental variation and change, theories have been advanced to explain both the general rules of development, as well as individual variation.6 In general, developmental-behavioral pediatricians may have the opportunity to educate primary care pediatricians, who would benefit greatly from attention to and extensive knowledge of the theory and research focused on these developmental issues. In their work, developmental-behavioral pediatricians have opportunities to observe the same children frequently and repeatedly over the course of individual development. Thus, if pediatricians are equipped with the proper knowledge, they are in a unique position to identify early risk factors that portend later, more serious difficulties. Moreover, they can intervene early while the difficulties are still manageable. They also have opportunities to follow up with these same children to determine whether a particular early intervention had a sustained and positive impact.
Since the appearance of a similar volume on developmental-behavioral pediatrics in the late 1990s,7 the field of developmental-behavioral pediatrics has witnessed extensive progress in theory development across several areas (e.g., biological bases of behavior, behavioral genetics and gene-environment interactions, developmental psychopathology). Concurrent with these developments, both the quantity and quality of research focused on such issues have increased as well. The purpose of this chapter is to review current theories relevant to the field of developmental-behavioral pediatrics. We begin with a discussion of “What makes a good theory?” in which we discuss features of theories that have had a major influence on the field. Second, we provide an historical perspective on theories in the field of developmental-behavioral pediatrics, followed by a discussion of more contemporary theoretical and empirical work. Finally, we conclude with a discussion of directions for future theory development.
WHAT MAKES A GOOD THEORY?
Before a discussion of components of useful theories, it is important to define our use of the term theory and to note similarities between our use of this term and other related terms, such as framework and model. A strict (but also ideal) definition of theory is as follows:8–10 “[A theory is] a set of interconnected statements-definitions, axioms, postulates, hypothetical constructs, intervening variables, laws, hypotheses… usually expressed in verbal or mathematical terms.…[The theory] should be internally consistent… testable and parsimonious… [and] not contradicted by scientific observations” (Miller, 1983, pp 3-4).11 In general, most scientific theories fall short of this ideal definition. For this book, we have chosen a “soft” definition of theory. In our view, a theory is a model or framework that guides clinical work or research endeavors. It could be considered a metaphor for how two or more variables are related or how a causal process is likely to unfold over time (e.g., a camera is a metaphor for how the human eye functions; such a metaphor could serve as a guide for future investigations of the eye). Despite their limitations, “soft” theories provide more guidance than if there were no theories. In the absence of theory, physicians would be forced to rely on past experience and common sense. However, as noted by Lilienfeld, the more widely held the belief is and the more that a belief is based on common sense (e.g., parents have more influence on children than children have on parents), the more crucial it is that such beliefs be carefully scrutinized and subjected to empirical evaluation.12
Clarity of Focus
Useful conceptual models are often focused on a phenomenon that is important to professionals working in the field and are very specific in their focus, rather than overly general. For example, suppose an investigator wanted to develop a model of communication between practitioner and patient. It would be tempting to include all possible variables in this model. With regard to the patient, the investigator could include variables such as past medical experiences, type of condition, temperament, communication style variables, personality variables, historical and family system variables, and variables that focus on beliefs and expectations. With regard to the practitioner, the investigator could include a similar number of variables. Although all of these variables may be relevant to the phenomenon of interest, inclusion of all relevant variables would make for a very unwieldy conceptual model. From the perspective of a practitioner, there would be too many variables to integrate, making it difficult to consider any one of them during an actual interaction with a patient. From a research perspective, the model would likely be highly exploratory and require “everything but the kitchen sink” data-analytic strategies. Findings based on such strategies would not necessarily be validated across research programs. Thus, a more focused model would be needed. Such a model would explain a smaller aspect of the phenomenon of interest, but it would probably have more clinical and research usefulness. Continuing with the example just given, the investigator might develop a model that proposes a typology of practitioner and patient communication styles that delineates the best fitting matches between different practitioner and patient communication styles.1
Developmental Emphasis
A developmental emphasis is crucial for the work of the developmental-behavioral pediatrician and should, therefore, be an integral part of any theoretical or conceptual model. At the most general level, a model is developmentally oriented if (1) it includes developmentally relevant constructs (which could be biological, cognitive, emotional, or social), (2) the constructs are tied to the age group under consideration, and (3) it emphasizes changes in the proposed constructs.11 Such a model also takes into account the critical developmental tasks and milestones relevant to a particular child’s or adolescent’s presenting problems (e.g., level of self-control, ability to regulate emotions, the development of autonomy, a child’s ability to share responsibilities for medical treatments with parents).
The Model Addresses Limitations of Previous Models and Research
A useful theory-driven model seeks to move the field forward by addressing gaps in prior theorizing.3 The process by which conceptual models are derived is often a cumulative process by which older conceptual models are integrated with new empirical findings to generate new conceptual models. For example, Thompson and Gustafson reviewed prior models of psychological adaptation to chronic illness.3 Older models13 specified important constructs of interest (e.g., stress, coping style, response to illness), but later models14,15 were more focused on identifying particular components of these constructs that were relevant (for an example involving palliative vs. adaptive coping and specific cognitive processes concerning illness appraisal and expectations, see Thompson and colleagues15). Later, these more focused models were refined in response to research findings and critiques16 (see Wallander et al for revised versions of these models17).
Specification of Independent Variables and Dependent Variables
Conceptual models rarely account completely for a medical phenomenon; thus, there is usually variance in the outcome that the predictors do not adequately explain. For example, in attempting to understand causes of spina bifida (a congenital birth defect that produces profound effects on neurological, orthopedic, urinary, cognitive/academic, and social functioning), investigators have recently determined that low levels of maternal folic acid before conception are causally related to the occurrence of spina bifida. Unfortunately, this single variable does not account for all cases of spina bifida. Thus, comprehensive models of causation for this condition often include other variables as well, including genetic and behavioral factors.
Articulation of Links between Independent Variables and Dependent Variables
Perhaps the most important aspect of a conceptual model is the articulation of links between the predictors and outcomes. Models vary considerably in their levels of sophistication; at the simplest level, main (or direct) effects of predictor on outcome (e.g., parenting behaviors→child adjustment) are proposed. As the number of predictors increases, scholars often seek to test multiple pathways between predictors and outcomes. Researchers who study pediatric populations have begun to posit more complex theoretical models to explain phenomena of interest. These models include longitudinal developmental pathways, mediational and moderational effects, genetic × environment interaction effects, risk and protective processes, and intervening cognitive variables (e.g., cognitive appraisal3). This enhancement of the theoretical base has necessitated an increase in terminological and data-analytic sophistication. Research focused on mediational and moderational models (and particularly the definitions of risk and protective factors) has emerged as a crucial method for testing competing theories about developmental pathways and other concepts central to developmental-behavioral pediatrics (see Rose et al for a more in-depth discussion18).
MEDIATOR
A mediator is an explanatory link in the relationship between two other variables (Fig. 2-1). Often a mediator variable is conceptualized as the mechanism through which one variable (i.e., the predictor) influences another variable (i.e., the criterion).17,19,20 Suppose, hypothetically, that a researcher finds that parental intrusive behavior is negatively associated with child adherence to a medical regimen. Given these findings, a researcher could explore whether a third variable (e.g., child independence) might account for or explain the relationship between these variables. Continuing with the example, suppose that child independence mediates the relationship between intrusiveness and adherence (more intrusive parenting→less child independence→less medical adherence). In this case, parental intrusiveness would have a negative effect on level of child independence, which in turn would contribute to poor medical adherence.21
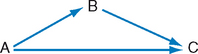
FIGURE 2-1 Mediated relationship among variables. A, Predictor; B, mediator; C, criterion/outcome.
(From Rose BM, Holmbeck GN, Coakley RM, et al: Mediator and moderator effects in developmental and behavioral pediatric research. J Dev Behav Pediatr 25:1-10, 2004. Copyright 2004 by Lippincott Williams & Wilkins. Reprinted with permission.)
MODERATOR
A moderator, unlike a mediator, is a variable that influences the strength or the direction of a relationship between a predictor variable and a criterion variable (Fig. 2-2). Suppose a researcher is interested in examining whether familial stress (e.g., in the context of a child’s chronic illness) is associated with the child’s psychological adjustment and, more specifically, whether this effect becomes more or less robust in the presence of other contextual variables. For example, the strength or the direction of the relationship between stress and adjustment may depend on the level of uncertainty that characterizes the child’s condition; that is, a significant association between stress and adjustment may emerge only when there is considerable uncertainty regarding the child’s illness status. By testing “level of uncertainty” as a moderator of the relationship between stress and outcome, the researcher can specify certain conditions under which family stress is predictive of the child’s adjustment.
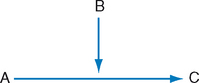
FIGURE 2-2 Moderated relationship among variables. A, Predictor; B, moderator; C, criterion/outcome.
(From Rose BM, Holmbeck GN, Coakley RM, et al: Mediator and moderator effects in developmental and behavioral pediatric research. J Dev Behav Pediatr 25:1-10, 2004. Copyright 2004 by Lippincott Williams & Wilkins. Reprinted with permission.)
Developmental-behavioral pediatric researchers often posit mediational and moderational processes when conducting studies of risk and protective factors. In general, research on risk and protective factors is focused on understanding the adjustment of children who are exposed to varying levels of adversity. There is evidence that both contextual factors (e.g., socioeconomic status, family level functioning, peer relationships) and developmental variables (e.g., cognitive skills, autonomy development) can significantly influence outcomes for individuals living under adverse conditions and thus serve a moderational role.21–24 Risk and protective processes have been explored in the study of “resilience,” a term used with increasing frequency in developmental and pediatric research (see later section on resilience). Resilience refers to the process by which children successfully navigate stressful situations or adversity and attain developmentally relevant competencies.25 More generally, appropriate application of these terms (i.e., resilience, risk factors, protective factors) is necessary for promoting terminological consistency.
PROTECTIVE VERSUS RESOURCE FACTORS
Protective factors are contrasted with resource factors. Specifically, a factor that has a positive effect on the sample regardless of the presence or absence of a stressor is a resource factor24 (sometimes referred to as a promotive factor26). For example, if a positive father-child relationship reduces behavior problems only in children of depressed mothers but has no effect on children of nondepressed mothers, then the father-child relationship would be conceptualized as a protective factor (Fig. 2-3).18 However, if the positive father-child relationship reduces behavior problems in all children, regardless of the mother’s level of depression, then it would be conceptualized as a resource factor (see Fig. 2-3).18,24 A model may also identify a positive father-child relationship as both a protective and resource factor if it reduces behavior problems in children who have depressed mothers more than in children who have nondepressed mothers but if it also produces a significant reduction in behavior problems for all children, regardless of level of maternal depression. It is also important to note that a protective factor represents a moderational effect (see the statistically significant interaction effect in Fig. 2-3, left), whereas a resource factor represents an additive effect (i.e., two main effects; see Fig. 2-3, right).18
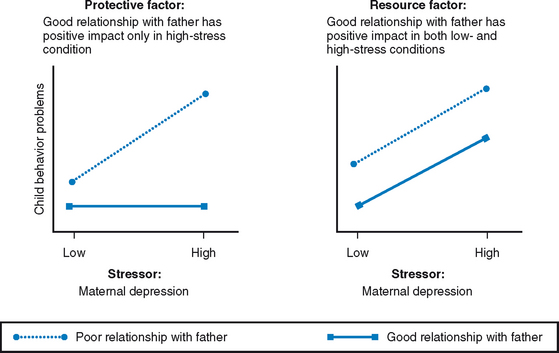
FIGURE 2-3 Protective factors (left) and resource factors (right).
(From Rose BM, Holmbeck GN, Coakley RM, et al: Mediator and moderator effects in developmental and behavioral pediatric research. J Dev Behav Pediatr 25:1-10, 2004. Copyright 2004 by Lippincott Williams & Wilkins. Reprinted with permission.)
RISK VERSUS VULNERABILITY FACTORS
Risk and vulnerability factors operate in much the same way as resource and protective factors but in the opposite direction (Fig. 2-4).18 A vulnerability factor is a moderator that increases the chances for maladaptive outcomes in the presence of adversity.24 Like a protective factor, a vulnerability factor operates only in the context of adversity. In contrast, a variable that negatively influences outcome regardless of the presence or absence of adversity is a risk factor.24 For example, witnessing violence in the home environment is conceptualized as a vulnerability factor if it increases behavior problems only in children who are also exposed to a stressor, such as viewing extreme violence on television (see Fig. 2-4, left).18 A vulnerability factor is a moderator and is demonstrated statistically with a significant interaction effect. Witnessing violence in the home can be conceptualized as a risk factor if it results in an increase in child behavior problems for all children, regardless of the amount of television violence witnessed. As with resource factors, a risk factor represents an additive effect (i.e., two main effects; see Fig. 2-4, right).18 A model may also identify a factor as being both a risk and vulnerability factor if it increases the chance of a maladaptive outcome in samples with and without exposure to a stressor but also if it increases the chances for maladaptive functioning significantly more in the sample with the stressor.
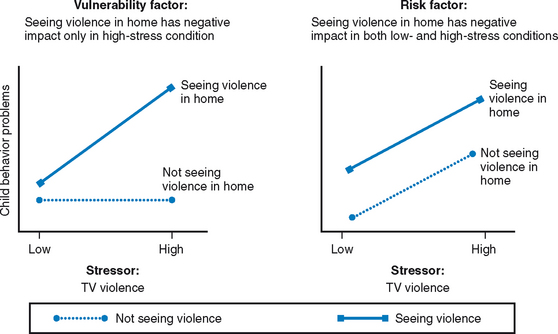
FIGURE 2-4 Vulnerability factors (left) and risk factors (right).
(From Rose BM, Holmbeck GN, Coakley RM, et al: Mediator and moderator effects in developmental and behavioral pediatric research. J Dev Behav Pediatr 25:1-10, 2004. Copyright 2004 by Lippincott Williams & Wilkins. Reprinted with permission.)
In sum, if a factor significantly promotes or impairs the chances of attaining adaptive outcomes in the presence of a stressor, then it operates through protective or vulnerability mechanisms, respectively. In these cases, the factor serves a moderational role. However, if a factor significantly promotes or impairs the chance of attaining adaptive outcomes without differentiating between the presence or absence of a stressor, then it is conceptualized as operating through resource or risk mechanisms, respectively. Many examples of these types of effects have appeared in the literature. For example, in their study of maltreatment and adolescent behavior problems, McGee and associates found that the association between severity of physical abuse and internalizing symptoms was moderated by gender.27 Specifically, the association was positive and significant for girls but not for boys. In other words, being male could be considered a protective factor against the development of internalizing symptoms when a person is exposed to high levels of physical abuse. Similarly, Gorman-Smith and Tolan found that associations between exposure to violence and anxiety/depression symptoms in young adolescents were moderated by level of family cohesion.28 The effect was significant (and positive) only at low levels of cohesion. At high levels of cohesion, the effect was nonsignificant, which suggests that family cohesion buffers (or protects against) the negative effects of exposure to violence on adolescent mental health.
Some investigators have sought to examine risk factors as mediational causal chains over time. For example, Tolan and colleagues examined a causal chain as a predictor of violent behaviors in adolescence, which included the following variables (in temporal order): community structure characteristics, neighborliness, parenting practices, gang membership, and peer violence.29 Woodward and Fergusson examined predictors of increased rates of teen pregnancy and found a causal chain that began with early conduct problems; such problems were associated with subsequent risk-taking behaviors in adolescence, which placed girls at risk for teen pregnancy.30
Clear Implications for Interventions
Perhaps, of most importance, a theory should have clear implications for interventions. Although many variables have potential intervention implications, some are clearly more relevant to practice than are others. For example, suppose a researcher is examining predictors of medical adherence during adolescence in children with type 1 diabetes. The researcher could examine parent and child adherence-relevant problem-solving ability as a predictor of subsequent levels of adherence, or the researcher could examine adolescent personality variables (e.g., neuroticism) as predictors of adherence. Clearly, it would be easier to imagine developing an intervention that targets problem-solving ability than one that targets a personality variable. Moreover, the researcher would speculate that problem-solving ability is also more likely to be responsive to an intervention than is a personality variable. Interestingly, some variables may not appear to be intervention-relevant at first glance but may become so on further examination. For example, demographic variables (e.g., gender, social class) would obviously not be targets of an intervention, but they may be important markers for risk. For example, the researcher may find that individuals from the lower end of the socioeconomic distribution are at increased risk for medical adherence difficulties; thus, this subpopulation could be targeted as an at-risk group and receive a more intense intervention.
Not only do predictor-outcome studies have implications for intervention work but also intervention studies themselves can be very instructive. Specifically, a research design that includes random assignment to intervention condition provides a particularly powerful design for drawing conclusions about causal mediational relationships.31,32 These types of models have three important strengths. First, significant mediational models of intervention effects provide information about mechanisms through which treatments have their effects.33–35 Simply put, with such models, researchers are able to ask how and why an intervention works.33 Second, as noted by Collins and associates, if a manipulated variable (i.e., the randomly assigned intervention) is associated with change in the mediator, which is in turn associated with change in the outcome, there is significant support for the hypothesis that the mediator is a causal mechanism.36 Researchers are more justified in invoking causal language when examining mediational models in which the predictor is manipulated (i.e., random assignment to intervention vs. no intervention) than in mediational models in which no variables are directly manipulated. With random assignment, many alternative interpretations for a researcher’s findings can be ruled out, and thus it is more certain that changes in the outcomes (e.g., symptoms of attention-deficit/hyperactivity disorder [ADHD]) result from the intervention instead of from some other factor.
Third, when a researcher isolates a significant mediational process, the researcher has learned that the mediator may play a role in the maintenance of the outcome (e.g., problem behavior). In this way, knowledge about mediational processes in the context of randomized clinical trials informs investigators about etiological theories of disorders.33,37 As an example of this strategy, Forgatch and DeGarmo examined the effectiveness of a parenting-training program for a large sample of divorcing mothers with sons.38 They also examined several parenting practices as mediators of the intervention→child outcome association. In comparison with mothers in the control sample, mothers in the intervention sample showed improvements in parenting practices. Improvements in parenting practices were linked with improvements in child adjustment. Thus, this study provides important evidence that certain types of maladaptive parenting behavior maintain certain maladaptive child outcomes.
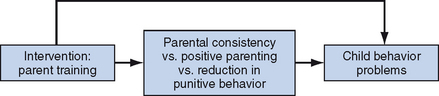
Such intervention/mediation models not only allow researchers to test potential mediators within an experimental design but also allow researchers to examine the differential utility of several mediational variables. In other words, a researcher can determine which mediator best accounts for the effectiveness of a given treatment. For example, if researchers examined the effectiveness of parenting training for decreasing child behavior problems (as in the preceding example), they might target three areas of parenting with this intervention: parental consistency, positive parenting, and harsh/punitive parenting. By testing mediational models within the context of an intervention study, they could determine which of these three parenting targets accounts for the significant intervention effect. It may be, for example, that the intervention’s effect on parental consistency is the mechanism through which the treatment has an effect on child outcome. This component of the treatment could then be emphasized and enhanced in future versions of the intervention (Fig. 2-5).18
This overview of features shared by the most influential theories provides the basis for a focused review of theories relevant to the field of developmental-behavioral pediatrics.
THEORETICAL MODELS IN DEVELOPMENTAL-BEHAVIORAL PEDIATRICS
It would, of course, be impossible to provide an overview of all relevant theories in the field of developmental-behavioral pediatrics. Thus, we have chosen theories from five areas that are of primary concern to developmental-behavioral pediatricians: (1) theories that take into account biological, genetic, and neurological bases for behavior; (2) transactional models of development; (3) theoretical principles from the field of developmental psychopathology (a relatively new discipline through which investigators seek to understand how problem behaviors develop and are maintained across the lifespan); (4) theories of adjustment to chronic illness; and (5) models relevant to medical adherence. Some important models are not covered because they are highlighted in other chapters in this volume (e.g., for a review of family systems theory and models of cultural influence, see Chapter 5).
A Brief Historical Perspective on Child Development
Modern theories of developmental-behavioral pediatrics have their roots in early theories of child development. The purpose of this section is to trace the history of some of the important constructs that are now taken for granted in more recent theorizing. In an earlier review for a volume on developmental-behavioral pediatrics, Kessen provided a comprehensive overview of past theories and research on human behavioral development (beginning with work conducted as early as 1850).6 Moreover, in the four-volume fifth edition of the Handbook of Child Psychology, an entire volume (more than 1200 pages) is devoted to “theoretical models of human development.” Thus, a complete overview of this area is well beyond the scope of this chapter.
The study of human development is a field devoted to identifying and explaining changes in behavior, abilities, and attributes that individuals experience throughout their lives. Because infants and young children change so dramatically over a relatively short time, they received intense empirical scrutiny in past research. However, in more recent years, research has been focused on developmental issues of relevance over the entire lifespan.39 Although the field of developmental psychology has undergone many changes since its advent in the late 1800s, several themes have been revisited throughout the past century.40 These include (1) the nature/nurture issue (i.e., what is the relative importance of biological and environmental factors in human development?), (2) the active/passive issue (i.e., are children active contributors to their own development, or are they passive objects, acted on by the environment?), and (3) the continuous/discontinuous issue (i.e., are developmental changes better seen as discontinuous or continuous?).6,41 These themes emerge throughout the following discussion of some of the most influential early theorists.
Charles Darwin’s A Biological Sketch of an Infant was the most influential of the “baby biographies” and is often cited as the impetus for the child study movement.42 His theory of evolution could be considered the underlying theoretical force behind the entire discipline of developmental psychology, and its influence continues to inspire present-day thought in the field. For example, Boyce and Ellis’s theory of biological stress reactivity (as discussed in a later section) is one example of a modern idea that is largely inspired by evolutionary theory.43 However, before Boyce and Ellis’s notion of biological stress reactivity, Darwinian theory influenced many other notable contributors, including one who would come to be known as the founder of American developmental psychology: G. Stanley Hall (1844–1924). Hall believed that human development follows a course similar to that of the evolution of the species.44,45 He acknowledged the scientific shortcomings of the baby biographies (which were based on potentially biased observations of small numbers of children) and attempted to collect more objective data on larger samples. In 1891, he began a program of questionnaire studies at Clark University in what is often considered the first large-scale scientific investigation of developing youth. Although research has since cast doubt on his “storm and stress model” as described in Adolescence, Hall was instrumental in bringing recognition to this period as a distinct and defining time of growth and transition.44
Hall is also recognized for his role as a mentor and administrator. In 1909, he invited Sigmund Freud (1856–1939) to Clark University, thereby generating international recognition for psychoanalytic theory. Originally trained as a neurologist, Freud observed that many of the physical symptoms seen in his patients appeared to be emotional in origin.46 Through a methodology much different from that employed by Hall, Freud used free association, dream interpretation, and hypnosis to analyze the histories of his emotionally disturbed adult patients. On the basis of his analyses, Freud proposed that development occurs through the resolution of conflict between what a person wants to do versus what the person should do. He suggested that everyone has basic biological impulses that must be indulged but that society dictates the restraint of these impulses. This notion formed the basis of Freud’s theory of psychosexual development. Although many of Freud’s ideas have not been supported by empirical evidence, no one would refute that his contributions changed clinicians’ thinking within the field. For instance, he was the first to popularize the notion that childhood experiences affect adult lives, as well as the first to introduce the idea of a subconscious motivation. In addition, Freud advanced the field by addressing the emotional side of human experience, which previous theorists had neglected.46
Freud was also the first prominent theorist to endorse an interactionist perspective, which acknowledged both biological and environmental factors that influence human development (although he emphasized the impact of environmental factors, such as parenting). Insofar as most theorists today consider both genetic and environmental factors that contribute to a person’s development (e.g., diathesis-stress model of psychopathology), Freud’s influence continues. In contrast to Freud’s interactionist viewpoint, the maturational theory of Arnold Gesell (1880–1961) represents a prominent biological theory of child development.47 In Gesell’s view, development is a naturally unfolding progression that occurs according to some internal biological timetable, and learning and teaching cannot override this timetable.48 He maintained that children are “self-regulating” and develop only as they are ready to do so. Gesell is noteworthy for the detailed studies of children’s physical and behavioral changes that were carried out under his supervision throughout his tenure at the Yale Clinic of Child Development. The results of Gesell’s observational studies revealed a high degree of uniformity in children’s development. Although developmental milestones may not have occurred at the same age for all children, the pattern of development was largely uniform (e.g., children walk before they run and run before they skip). Gesell used his data to establish statistical norms to describe the usual order in which children display various early behaviors, as well as the age range within which each behavior normally appears. Interestingly, physicians still use updated versions of these norms as general guidelines for normative development. Gesell also made important contributions to methodology in the field of psychology. He was the first to capture children’s observations on film, thereby preserving their behavior for later frame-by-frame study, and he also developed the first one-way viewing screens.
Although Gesell was influential in terms of his contributions to methodology and his establishment of developmental norms, his purely biological theory was deemed an oversimplication of the complex process of human development insofar as it neglected to account for the importance of children’s experiences. However, his emphasis on similarities across children’s development and his focus on patterns of behavior set the stage for Jean Piaget (1896–1980), who is often credited for having the greatest influence on present-day developmental psychology.49 Unlike the theorists previously discussed, many of Piaget’s general theoretical hypotheses are still widely accepted by developmental psychologists. One reason his theories are appealing is that they complement other theories well. For instance, more recent thinkers in developmental psychology combine aspects of Piagetian theory with information processing and contextualist perspectives to more thoroughly understand the process of cognitive development.
Piaget became interested in child cognitive development through the administration of intelligence tests. He was interested less in the answers that children provided to test questions than in the reasoning behind the answers they gave. He soon realized that the way children think is qualitatively different from how adults think. Piaget became immersed in the study of the nature of knowledge in young children, as well as how it changes as they grow older.50–52 He termed this area of study genetic epistemology. Unlike Gesell’s method, in which the researcher stood apart from his objects of study, Piaget developed a research technique known as the clinical method. This involved presenting children with various tasks and verbal problems that would tap into children’s reasoning. Although he would begin with a set of standardized questions, he would then probe children’s responses with follow-up questions to reveal the reasoning behind their responses. According to Piaget’s cognitive-developmental theory, children universally progress through a series of stages: the sensorimotor stage (birth to age 2 years), the preoperational stage (ages 2 to 7 years), the concrete operational stage (ages 7 to 11 years), and the formal operational stage (ages 11 years and beyond). Piaget’s theory is extremely complex, and a discussion of the processes by which children progress from stage to stage is beyond the scope of this chapter.50
Although Piaget’s ideas about children are still widely accepted today, his theory has not gone without criticism. One major criticism of his theory concerns its lack of emphasis on cross-cultural factors that may play a role in development. Although Piaget acknowledged that culture may influence the rate of cognitive growth, he did not address ways in which culture can affect how children grow and develop. He is also criticized for overlooking the role of social interactions in cognitive development. This latter idea is the hallmark of Lev Vygotsky’s (1896–1934) sociocultural perspective.53,54 According to Vygotsky, cognitive development occurs when children take part in dialogs with skilled tutors (e.g., parents and teachers).55 It is through the process of social interaction that children incorporate and internalize feedback from these skilled tutors. As social speech is translated into private speech and then inner speech, the culture’s method of thinking is incorporated into the child’s thought processes. Vygotsky is also noteworthy for his consideration of the way cognitive development varies across cultures. Unlike Piaget, who maintained that cognitive development is largely universal across cultures, Vygotsky argued that variability in cognitive development that reflects the child’s cultural experiences should be expected. As such, Vygotsky played a role in the movement toward cross-cultural and contextually oriented studies in developmental psychology. His influence can also be seen in the more recent literature on child and adolescent development, in which various contexts (e.g., family, peers, school, work) are considered with regard to their unique influences on development.
Current Theories in Developmental-Behavioral Pediatrics
MODELS THAT FOCUS ON BIOLOGICAL, GENETIC, AND NEUROLOGICAL BASES FOR BEHAVIOR
Several models of child functioning that focus on biological, genetic, and neurological bases for behavior have been proposed. It is believed that biologically based vulnerabilities can account, at least in part, for the emergence of certain psychosocial difficulties (e.g., depression, anxiety). In this section, models in the areas of biological stress reactivity and behavioral genetics (including a discussion of shared and nonshared environmental effects) are emphasized. Neurodevelopmental factors relevant to developmental-behavioral pediatricians are discussed thoroughly in Chapter 4.
BIOLOGICAL STRESS REACTIVITY
Stress reactivity is an individual differences variable that refers to an individual’s physical neuroendocrine response to stressful events and adversity.43 Researchers measure such reactivity with a host of physiological assessment techniques, including measures of heart rate, blood pressure, salivary cortisol, and respiratory sinus arrhythmia. Early research and theorizing on stress reactivity suggested that heightened or prolonged reactivity in response to stressors is maladaptive and places the individual at risk for adjustment difficulties (including affective disorder, anxiety disorders, and externalizing symptoms) and medical illness (e.g., heart disease). On the other hand, such reactivity may be adaptive in the short term by preparing the individual to confront external threats. Moreover, when significant stressors occur early in an individual’s life, such individuals appear to be at risk for heightened levels of stress reactivity.
In 2005, Boyce and Ellis proposed a complex and intriguing theory of biological stress reactivity.43 On the basis of a comprehensive review of research findings (including anomalous findings) in this literature, they concluded that the relationship between reactivity and outcome is not so straightforward. Rather, they proposed, according to an evolutionary-developmental theory, that high reactivity can result from exposure to highly stressful environments or from exposure to highly supportive/protective environments. As in previous theorizing, they maintained that early exposure to highly stressful environments can cause heightened reactivity (such individuals are more prepared for future occurrences of highly stressful events). But they also proposed that environments with very low stress can also produce children with heightened reactivity because such reactivity levels enable such children to experience more completely the beneficial characteristics of a protective environment. They argued further that this curvilinear relationship between early stress and reactivity is a process that has evolved through natural selection and one that affords advantages to both of these highly reactive groups. They concluded, “Highly reactive children sustain disproportionate rates of morbidity when raised in adverse environments but unusually low (emphasis added) rates when raised in low-stress, highly supportive settings.” Interestingly, in a empirical investigation that was a companion to their theoretical paper, Ellis and associates found support for many of their propositions.56 Empirical support for this viewpoint has also emerged in studies of primates.57
Another intriguing theory of stress reactivity was proposed by Grossman and colleagues, who discussed longitudinal changes in stress reactivity in depressed individuals.58 They argued that the interplay between stressful environmental events and genetic expression can produce “potentiated stress reactivity” over time.58 They suggested that early stressful events may alter genetic expression, whereby depressive episodes are triggered by increasingly less intense environmental and psychological stressors over time. The term kindling is used to explain this process in which life experiences produce subtle changes in brain functioning, genetic expression, and stress reactivity. They also invoke Waddington’s compelling concept of “canalization.”59 The argument here is that development progresses in a “canal” of normative development that increases in “depth” with age. Psychopathology (e.g., depression) is likely to result if the individual is pushed up the sides of the canal beyond a genetically determined threshold (i.e., the threshold is higher in the canal for some individuals than for other individuals). In typically developing individuals, and because of the increasing depth of the canal, early stressors are more likely to move the individual beyond the pathology threshold than are stressors that occur later in life. With regard to depression, a severe stressor early in childhood can produce a depressive episode. After recovery from this episode, the individual can experience a second episode (moving above the threshold in the canal) as a result of another, less intense stressor. Genetics may influence the severity of the stressor that is necessary for the initial episode and the pace at which the kindling process takes hold.58 The following case example illustrates how such a process may unfold:
BEHAVIORAL GENETICS
Two important areas of behavioral genetics are discussed in this section. First, a number of investigators have examined ways in which there are gene × environment interactions, whereby the effect of certain environmental conditions may be exacerbated (or buffered) depending on the level of genetic vulnerability. Second, the field of behavioral genetics has attempted to shed light on how behavioral variation observed among children and adolescents can be ascribed to either genetic or environmental processes or to both. Researchers in this area have contributed to the field by investigating how both “nature” and “nurture” are the precursors of normal as well as abnormal behavior.60,61 We begin with a discussion of gene × environment interactions and later discuss how investigators have attempted to partition variance into genetic and environmental effects.
Whether an individual is more a product of his or her genetic makeup versus his or her environment has been long debated. However, research in the fields of medicine and psychology has indicated that these influences are rarely distinct from one another and that their effects are probabilistic rather than determinative.62 For example, modifications in lifestyle can decrease the risk of heart disease in an individual who is genetically prone to this illness.
Investigators who study joint effects of genes and environment on psychopathology distinguish between gene-environment interactions and gene-environment correlations.63 Gene-environment interactions represent the diathesis-stress model of psychopathology. According to this model, certain environmental stressors contribute to the emergence of psychopathology in individuals who have a genetic vulnerability (i.e., diathesis). In this way, associations between stress and outcome are moderated by genetic vulnerability. In a set of intriguing studies, Caspi and colleagues identified polymorphisms in specific genes that moderate the effects of negative life experiences on the emergence of both antisocial behavior and depression.64,65
Unlike gene-environment interactions, gene-environment correlations refer to significant associations between genetic vulnerabilities and environmental risk, whereby individuals with higher levels of genetic vulnerability are more likely to be exposed to higher levels of environmental risk.63 Hypothesized mechanisms for gene-environment correlations include (1) a passive process, whereby environmental risk is beyond the individual’s control; (2) an evocative process, whereby an individual with a certain genetic vulnerability elicits certain toxic characteristics from the environment; and (3) an active process, whereby an individual with a certain genetic vulnerability actively alters or promotes a specific type of environment. To illustrate these hypothesized mechanisms, consider the example of a child with a genetic vulnerability to ADHD:
Studies of depression, anxiety, and antisocial behavior have supported the role of both gene-environment interactions and gene-environment correlations.62,64–67
The degree to which there is interplay between genetic and environmental factors may also be dependent on developmental timing and contextual influences. For example, studies of the roles of genes and environment on depressive symptoms have suggested that environmental factors are associated with depressive symptoms in childhood. However, during adolescence and adulthood, genes appear to play a more salient role.68 In addition, in terms of gene-environment correlations, passive processes, such as family influences, may be more prominent during early childhood. Evocative and active gene-environment correlations may play a greater role later in development.69 Finally, the strength of genetic influence may be dependent on environmental context. For example, genetic factors appear to play a weaker role in the intellectual development of children raised in impoverished environments than in those raised in more affluent environments.70
Grossman and colleagues noted that the manifestation of many pathological conditions that may, at first glance, appear to be produced entirely by genetic factors or environmental factors may, in fact, be produced by a combination of genetic and environmental factors.58 Fetal alcohol syndrome is an example of a disorder that is caused environmentally (by fetal exposure to alcohol). Clinical outcomes associated with fetal alcohol syndrome result from disruption of several neurodevelopmental processes. On the other hand, the developmental processes that are affected depend on several factors. For example, large single-episode quantities of alcohol are more detrimental to fetal brain development than are several exposures to low levels of alcohol. Moreover, effects are greater in the later stages of pregnancy. Thus, although fetal alcohol syndrome is clearly caused by environmental factors, it is also true that environmental factors are interacting with “genetically determined developmental time courses” to produce varying detrimental effects on brain development.58 Unlike fetal alcohol syndrome, fragile X syndrome is an example of how a genetically caused disorder can be influenced by environmental factors, inasmuch as individuals with fragile X syndrome vary widely in their presentation. Environmental factors, such as the quality of the home environment, can interact with genetic effects to lead to significant variability in outcomes for individuals afflicted with fragile X syndrome.58
With regard to the partitioning of individual variation (e.g., variation in childhood problem behaviors) into environmental and genetic effects, classic behavioral genetics research methods include family, twin, and adoption study designs. Adoption and twin studies, in which the family members of varying genetic relatedness are compared, are needed to disaggregate genetic and environmental sources of variance. For example, if heredity affects a behavioral trait, then it follows that monozygotic twins will be more similar to each other with regard to that trait than will dizygotic twins. A stepfamily design is also used in which monozygotic twins and dizygotic twins are compared, along with full siblings, half-siblings, and unrelated siblings living in the same household.60,61,71
Most of the work in behavior genetics has employed an additive statistical model. One basic assumption of the additive model is that genetic and environmental influences are independent factors that sum to account for the total amount of individual variation. This model partitions the variance of the characteristic being studied among three components: genetic factors, shared environmental influences, and nonshared environmental influences. A heritability estimate, which ascribes an effect size to genetic influence, is calculated. The variance left over is then ascribed to environmental influences.36,60,61,71
Environmental influences are then further subdivided into shared and nonshared types. The term shared environment refers to environmental factors that produce similarities in developmental outcomes among siblings in the same family. If siblings are more similar than would be expected from their shared genetics alone, then this implies an effect of the environment that is shared by both siblings, such as being exposed to marital conflict or poverty or being parented in a similar manner. Shared environmental influence is estimated indirectly from correlations among twins by subtracting the heritability estimate from the monozygotic twin correlation. Nonshared environment, which refers to environmental factors that produce behavioral differences among siblings in the same family, can then be estimated. Nonshared environmental influence is calculated by subtracting the monozygotic twin correlation from 1.0.60,61,71 In the stepfamily design described previously, shared environmental influence is implicated when correlations among siblings are large across all types of sibling pairs, including those that are not related. On the other hand, nonshared environmental influence is implicated when sibling correlations are low across all pairs of siblings of varying genetic relatedness, including monozygotic twins.72
Results of multiple studies with genetically sensitive designs suggest that many aspects of child and adolescent psychopathology show evidence of genetic influence.60,61,71 Autism and Tourette syndrome in particular have been demonstrated to be mostly genetically determined.61,71 Genetic factors have also been found to strongly influence externalizing behaviors, including aggression.73 Although the results are less clear, genetic influence has been associated with the development of internalizing problems as well.74 However, genetic influence does not account for all of the variance in psychopathological disorders.60,61,71 For example, the environmental conditions under which children and adolescents are socialized play an important role. Interestingly, however, it is the environmental factors that are not shared—those that create differences among siblings and not shared environmental factors—that seem to contribute to a large portion of the variation. Environmental factors that have been postulated to be nonshared include differential treatment by parents, peer influences, and school environment.60,61,71
Nonshared environmental factors have been implicated in hyperactivity, anorexia nervosa, aggression, and internalizing symptoms.71 In addition, the combination of nonshared and genetic influences may influence the adolescent’s choice of peer group.75 Juvenile delinquency appears to be one exception to the rule in that shared environmental factors have been shown to be more influential than nonshared environmental or genetic factors.71
Behavior genetics research has gone beyond the partitioning of variance into genetic and environmental components. For example, researchers have examined how differential parenting practices may produce differing developmental outcomes among siblings. One study revealed that more than 50% of the variance in antisocial behavior and 37% of the variance in depressive symptoms were associated with conflictive and negative parenting behavior that was directed specifically at the child.76 However, research has also suggested that longitudinal associations between both parenting behavior and child adjustment may be explained partly by genetic factors,77 which suggests that genetically influenced characteristics of the child may elicit specific types of parenting behavior. In this way, nonshared experiences of siblings may in fact reflect genetic differences, such as differences in temperament.78 One adoption study demonstrated that those who were at genetic risk for the development of antisocial behavior, by virtue of having a biological parent with a disorder, were more likely than children without this risk to be exposed to coercive parenting by their adoptive parents.79
Another important question examined in behavioral genetics research is whether genetic influences are more prominent at the extreme range of a psychopathological condition. By examining the full range of symptoms rather than specific diagnoses, behavior genetics research may highlight the continuity or discontinuity between normal and abnormal development.61 One study showed that although variation in subclinical depressive symptoms is influenced mostly by genetics, adolescent depressive disorder appears to be influenced mostly by shared environmental factors.74 Behavior genetic research has also demonstrated that genetic influences may partly explain comorbidity among disorders.60 One study demonstrated that half of the correlation between externalizing and internalizing behaviors can be explained by common genetic liability.72
Researchers have pointed to the many limitations of behavior genetics research that need to be considered when these findings are evaluated.34,36,80,81 In particular, the additive statistical model, the assumption that lies at the heart of behavior genetics methodology, has been criticized as neglecting to consider the potentially important contribution of gene-environment interactions (see earlier discussion). As noted previously, genetic and environmental influences may also be correlated.34,36,80–82 Stable heritability estimates are also difficult to calculate. These estimates are highly influenced by the range of genetic and environmental variations within the sample and also tend to be influenced by reporter. For example, parent reports of child characteristics tend to show lower heritability estimates than when the same characteristics are reported on by children or teachers or when observational measures are used.81 If heritability estimates are unstable, then estimates of environmental influences, derived from heritability estimates, are also unstable.81 Critics have suggested that environmental influences cannot be estimated without being measured directly. However, the methods used in studies of environmental factors, such as differential parenting, may also be difficult to interpret. For example, genetic similarity may be confounded with family structure in that full siblings are likely to have more congruent parenting experiences than are half-siblings or step-siblings.80,81 Also, shared events, such as those found in similar family environments, may contribute to nonshared variance in that different siblings may be affected differently by the same experiences.60
TRANSACTIONAL MODELS OF DEVELOPMENT
Transactional models have been crucial in highlighting how children can have an effect on their environment (e.g., their parents). For example, parents may not be aware that their children can have significant effects on their parenting and that children are not merely passive recipients of their parenting behaviors and values. As one example, it is known that a child’s temperament (i.e., adaptability, reactivity, emotionality, activity level, sociability) has a significant effect over time on the nature and quality of a parent’s behaviors toward the child.83
Studies of temperament and attachment provided early support for a transactional model of development.84,85 Theories that postulated that negative temperament was simply a result of poor parenting behaviors were replaced by the idea that specific child characteristics elicited maladaptive parenting, which later resulted in child behavioral difficulties.86 Similarly, increasing emphasis has been given to the child’s role in the development of attachment style, as illustrated in the following case example:
Consistent with Bronfenbrenner’s biopsychosocial model,87 various levels of context can interact with one another and either directly or indirectly affect child development. For example, in the context of poor maternal social support, irritable infants may elicit unresponsive mothering, leading to insecure attachment.88 However, when provided with adequate social support, mothers may be able to respond to their children in a more positive manner, thereby promoting secure attachment.
In addition, the relative importance of various contexts on development is dependent on developmental timing. Whereas the family context is primary during infancy and early childhood, interactions with teachers and peers take on increasing importance in late childhood and adolescence.89,90 Research on conduct problems has supported this notion. In early childhood, children who exhibit difficult temperament and noncompliant behavior often elicit punitive and inadequate parenting practices, which may actually serve to reinforce noncompliant behaviors.91,92 Over time, parents and child may engage in interactions in which parenting becomes increasingly harsh and child behavior more noncompliant and aggressive. This transactional pattern appears to be especially salient in the context of poverty, as inherent parental stress and lack of access to resources may compromise parenting ability.89 In the school environment, the child’s aggressive behavior may lead to negative teacher-child interactions, contributing to poor academic achievement and negative peer interactions, resulting in peer rejection and poor self-esteem.89 Indeed, phenomena such as peer rejection have been found to both predict and be predicted by conduct problems.89 Additional research has supported the role of transactional processes in disrupting parent-child interactions and peer functioning in other types of psychopathology, such as depression and ADHD.66,93
Transactional processes contribute to the understanding of continuity, or maintenance, of psychopathology and personality characteristics, over time, through these cyclical interaction processes between the individual and the environment.94 Hence, lack of healthy adaptation over time is probably a reflection of continued dysfunctional interaction between an individual and his or her environment.95,96 Some studies of depression have differentiated between dependent and independent negative life events, occurrences that are within versus beyond an individual’s control, respectively. This research has demonstrated that whereas the onset of depression may result from the occurrence of independent negative life events, depressive symptoms may be maintained by dependent negative life events.66
The exacerbation and emergence of new psychosocial difficulties also can be understood through transactional processes. For example, aggressive individuals may be prone to peer rejection as a result of their aggressive behaviors. This “self-generated” peer rejection may create negative life events linked to depression.66 In addition, these individuals may hold cognitive biases that lead them to expect and misperceive others’ actions as rejecting, thereby further contributing to the negative cycle of aggression and depression.66
Transactional models of development are also suggestive of targets for interventions. Indeed, efforts to change perceptions, expectations, and child-environment interactions, through parent training, have proved successful in terms of promoting healthy attachment and reducing conduct problems in infants and children, respectively.97–99
DEVELOPMENTAL PSYCHOPATHOLOGY
Developmental psychopathology could be considered a metatheory, or a macroparadigm that integrates knowledge from many fields, including lifespan developmental psychology, clinical child psychology, family systems, neuroscience, and behavioral genetics, to name just a few.100,101 As such, this section is the longest and most detailed of the “current theory” sections. Developmental-behavioral pediatricians can benefit greatly from knowledge of this field because of its emphasis on tracing the evolution of problems in development. In this way, informed pediatricians can play a key role in identifying children who are manifesting the beginnings of maladaptive developmental trajectories and who are probabilistically at risk for eventually developing more severe levels of pathological behavior. In view of the young ages of their patients, they also have the first opportunity to recommend or provide interventions designed to reduce risk.
Assumptions and Tenets of the Developmental Psychopathology Perspective
The goal of developmental psychopathology is to understand the unfolding of psychopathology over the lifespan and how the processes that lead to psychopathology interact with normative developmental milestones and contextual factors.101,102 Some of the assumptions and tenets of this field are as follows:101,102
Developmental Trajectories during Childhood and Adolescence: Multifinality and Equifinality
As implied previously, proponents of the developmental psychopathology perspective attempt to understand how pathology unfolds over time, rather than examining symptoms at a single time point. As a consequence, developmental psychopathologists have found the notion of “developmental trajectories” very useful.101 For example, researchers could examine alcohol use and isolate different developmental trajectories of such use over time (e.g., some youth may show rapid increases in alcohol use over time, some may show gradual increases, and others may show increases followed by decreases109).
It is also assumed that some developmental trajectories are indicative of a developmental failure that probabilistically increases the chances that a psychopathological disorder will develop at a later point in time.101 Thus, there is an interest in isolating early-onset trajectories that portend later problems. As an example, Dodge and Pettit pointed out that children who have early difficult temperaments (i.e., an early trajectory) who are also rejected by their peers for 2 or more years by grade 2 have a 60% chance of developing a serious conduct problem during adolescence.89 Again, this confluence of trajectory (i.e., difficult temperament) and risk factor (i.e., chronic peer rejection) does not automatically produce a conduct-disordered adolescent; rather, it merely increases the odds that the child will develop such a disorder.
In view of the vast individual differences in trajectories in any given domain of functioning, developmental psychopathologists have also been interested in the concepts of multifinality and equifinality.110 Multifinality occurs when there are multiple outcomes in those who have been exposed to the same antecedent risk factor (e.g., maternal depression). After equivalent exposure to a parent who is depressed, not all children so exposed will develop along identical pathways. In a study of multifinality, Marsh and colleagues examined outcomes of adolescents with insecure preoccupied attachment orientations (i.e., they all had the same starting point).111 Those adolescents with mothers who displayed low levels of autonomy in observed interactions were more likely to display internalizing symptoms. Conversely, those with mothers who displayed very high levels of autonomy were more likely to exhibit risky behaviors. Thus, multiple outcomes (i.e., multifinality) occur in those who all have the same initial risk factor (i.e., insecure preoccupied attachment orientation).
Equifinality occurs when individuals with the same level of psychopathology achieved such pathological outcomes through different pathways. Evidence for equifinality has emerged in research. For example, Harrington and associates found that suicidal behavior can be reached through different paths, one involving depression and another involving conduct disorder.112 Similarly, in girls, it appears that several of the same outcomes (e.g., anxiety disorders, substance use, school dropout, pregnancy) emerge in those with depression or conduct disorder.113 Finally, Gjerde and Block suggested that depressed adult women and men progress along very different developmental pathways before developing depression.114 It is worth noting, from an intervention perspective, that the presence of equifinality suggests that different versions of a given treatment for a given problem may be needed, depending on the pathway by which an individual progressed toward a psychopathological outcome.
Interestingly, the existence of such diverse types of trajectories has been supported by past research. For example, Lacourse and colleagues were able to isolate different trajectories of delinquent group membership in boys and their association with subsequent violent behaviors115 (see Zucker et al116 for a similar example involving a typology of alcoholics or Broidy et al117 for an example involving outcomes of typologies of childhood aggression). Such approaches have been termed person-oriented approaches (as opposed to variable-oriented), insofar as people are clustered into groups on the basis of the similarity of their characteristics or patterns of trajectories over time.118 Trajectory groups are differentiated on the basis of their patterning or profile of scores on antecedent or outcome variables of interest (e.g., maladaptive parenting, school failure). Moreover, such trajectories can assume quadratic forms (i.e., U-shaped functions).119
The Onset versus Maintenance of Psychopathology
It appears that factors that lead to the onset or initiation of a developmental trajectory are often different from those that maintain an individual on a developmental trajectory.108 This distinction has considerable clinical relevance. For example, a professional may be able to prevent the onset of sleep problems in young children by instructing parents on how to institute various behavioral plans early in development. Once a maladaptive sleep pattern emerges, other types of interventions may be needed.
With regard to maintenance of problem behaviors, an individual who has begun on a particular pathway may continue on the pathway or may be steered from the pathway.105 Factors that steer an individual from a maladaptive trajectory may be chance events, developmental successes, or protective processes that serve an adaptive function.102 In an analogous manner, other factors may steer individuals from adaptive trajectories onto maladaptive trajectories. It is an assumption of developmental psychopathology that maintenance on a pathway is more likely than steering away, particularly when an individual has moved through several developmental transitions on the same pathway.108
What do we know about factors that lead to the onset of maladaptive paths versus those that serve to maintain individuals on such pathways? Steinberg and Avenevoli argued that researchers have tended to confuse factors that lead to the onset of psychopathology versus those that lead to its maintenance and that this confusion has hampered progress in the field of developmental psychopathology.108 With regard to “onset,” Steinberg and Avenevoli argued (from a “diathesis-stress” perspective) that biological predispositions (e.g., temperament, level of autonomic arousal) can exacerbate or decrease the degree to which individuals are vulnerable to the effect of subsequent environmental stressors.108 Thus, two individuals exposed to the same stressor may begin on different pathways (e.g., anxiety vs. depression vs. aggression vs. no pathology), depending on the specific nature of each individual’s biological predispositions. Put another way, stressors appear to have nonspecific effects on the onset of pathology as a result of the moderating effect of particular biological vulnerabilities.108 These authors argued that future research on the elicitation of psychopathology needs to begin to isolate particular combinations of biological vulnerabilities and environmental threats that precede engagement with maladaptive developmental pathways. Indeed, such evidence is beginning to emerge; Brennan and associates found that early-onset and persistent aggression are predicted by interactions of biological and social risks (see later discussion of early- vs. late-onset psychopathology).120 Similarly, as noted earlier, Caspi and colleagues found support for a gene × environmental stress interaction effect in predicting depressive symptoms.65
With regard to “maintenance,” Steinberg and Avenevoli argued that environmental stressors have specific effects on the course of psychopathology.108 Thus, it is possible that two individuals may begin on the same pathway (as a result of having the same biological predispositions and same level of exposure to early stressors) but may have very different long-term outcomes if their environments differ. For example, two young children who have started on an early aggression pathway may diverge from each other over time because one of them is exposed to incompetent parenting, lack of structure, and deviant peers and the other is not (also see Dodge and Pettit89). Those who begin on an “early aggression” trajectory are probabilistically more likely to associate with deviant peers and “choose” maladaptive environments, but this is clearly not always the case for every affected child. Steinberg and Avenevoli also provided evidence that those who continue on certain paths and select certain environments are also more likely to strengthen the synaptic weights or connections of the original biological predisposition (e.g., the nature of the child’s arousal regulation capacities), which makes it even less likely that the individual will desist from this behavior or be steered from the maladaptive developmental trajectory.108 Put another way, psychopathology is likely to be maintained in individuals in whom the symptoms or the antecedents of the symptoms are repeated.108 In the preceding example, “lack of structure” in the family environment may not be a factor in the onset of conduct problems, but it may help maintain these problems because it permits more exposure to deviant peers and permits the pathological process to become more ingrained and entrenched.108
Researchers in several areas have begun to distinguish between onset and maintenance in their research designs (e.g., in the area of substance use, see Brook et al121; in the area of antisocial behavior, see Patterson et al122). For example, Dodge and Pettit89 provided a model of chronic conduct problems that is consistent with the notions advanced by Steinberg and Avenevoli.108 Dodge and Pettit argued that the bulk of research on conduct problems in childhood and adolescence suggests that children with certain neural or psychophysiological predispositions are more likely than others to begin a trajectory leading to conduct problems in adolescence. Such children are more likely to be parented harshly or neglected, because of their early difficult temperament. Outside the family, such children are more likely to be aggressive and to engage in conflict with peers during early childhood. According to Dodge and Pettit, such children enter elementary school in an at-risk state (although this transition is also an opportunity for steering away from this trajectory).89 Most often, such children experience peer rejection and have difficult relations with teachers. This combination of harsh parenting and peer rejection serves to stabilize the negative trajectory, which makes it less likely that steering away will occur. Although adolescence is another transitional opportunity, such children are at risk for affiliation with deviant peers. In fact, Dodge and Pettit provided evidence that such children react psychophysiologically in ways that make it uncomfortable for them to interact with typical peers.89 At this point, other cognitive strategies also play a role (e.g., the greater likelihood of hostile attributions). Movement toward a diagnosis of conduct disorder is overdetermined in such adolescents; the probability of such an outcome increases rapidly with age because of a confluence of multiple contributing factors.
In describing a developmental psychopathology model of depression, Hammen argued that cognitive vulnerabilities (e.g., negative view of self and negative self-schema) may be developed over time as a consequence of problematic relations and attachments with parents. Such cognitions make affected individuals more vulnerable to subsequent stressors, depression being the eventual outcome.123 Interestingly, Hammen provided evidence that depression-prone individuals are also more likely to generate new stressors or exacerbate existing ones, thus fueling the cycle123 (see Petersen et al for a similar perspective on adolescent depression124).
From a clinical perspective, understanding factors that contribute to the onset and/or maintenance of psychopathology informs preventive interventions, as well as the need to involve families in the implementation of these interventions. Research has demonstrated that, beginning in infancy, children with difficult temperaments are at risk for negative or harsh parenting. Early identification of difficult temperament then becomes a critical time point for clinician intervention. At this stage, pediatricians have the opportunity to intervene and provide support to parents in order to prevent the onset of conduct problems. Suppose that this early opportunity is missed. The transition into elementary school can then become stressful for the child and lead to difficulties with peer interactions. However, the clinician can act to prevent the maintenance of psychopathological behavior by engaging the family in the process of intervention. The earlier a clinician can identify risk for pathological behavior, the sooner the opportunity for prevention or intervention occurs, which in turn, provides the child with the most opportunities to master developmental transitions successfully.
Although we have argued thus far that factors associated with the onset of psychopathological behavior may differ from those associated with its maintenance, this is not always the case. For example, Patterson and associates found that early-onset antisocial behavior (during preadolescence) is linked with early arrests (before age 14) which are, in turn, linked with chronic offending in later adolescence (at age 18).122 Of most relevance to this discussion is that they also found that the factors that were associated with the onset of the trajectory (i.e., problematic parental discipline and monitoring, marital transitions, social disadvantage, deviant peer involvement) were the same factors that were associated with the maintenance of this “chronic offending” trajectory.
Age-at-Onset Research
A related line of research focuses on the age of the child or adolescent when symptoms of psychopathology begin. Interestingly, it appears that both the antecedents and long-term outcomes for children and adolescents with early onset of symptoms differ significantly from those for persons who have late-onset symptoms. This is important because it suggests that studies of adolescents that do not take age at onset into account in sampling procedures will probably combine across multiple subgroups of adolescents in whom severity and chronicity vary significantly.101
Perhaps the most widely cited example of such age-at-onset differences is Moffitt’s distinction between “life course-persistent” and “adolescence-limited” delinquents.125 The former exhibit earlier conduct problems than do the latter, and they are more likely to have neuropsychological problems, difficult early temperament, inadequate parenting and family dysfunction, hyperactivity, and psychopathic personality traits126 (although there is some debate about whether the neuropsychological difficulties predate the conduct problems127).
The outcomes for the life course-persistent delinquents tend to be worse than for their adolescence-limited counterparts, with higher rates of adult criminality and violence, substance dependence, and adult work-related problems.101,128 The conduct problems of adolescence-limited delinquents are more likely to abate over time than is the case for the life course-persistent delinquents (although the former are not without problems, inasmuch as they are also at risk for mental health problems and high levels of life stress).127,128 Clearly, these are very different pathways with different antecedents and outcomes. On the other hand, if these two groups were studied together at only one point in time (e.g., middle to late adolescence), their behaviors may appear similar.126 Finally, Moffitt and colleagues suggested that there is a third group of boys who are aggressive as children but exhibit low levels of conduct problems in adolescence (in earlier work, these boys were referred to as “recoveries”).128 These individuals are also at risk for problems in adulthood, but the risk is lower than in the other two groups just described. Moreover, their problems are more likely to be of the internalizing type (e.g., depression, anxiety). An analogous distinction has been made in the literature on adolescent alcohol use. Zucker and associates described three types of adolescent and young adult “alcoholisms,” each with different ages at onset, antecedents, and long-term consequences129 (see Schulenberg et al for a similar approach to adolescent alcohol use130).
Interestingly, it appears that Moffitt’s distinction between the two types of delinquency in adolescents (i.e., childhood onset vs. adolescence limited) may apply only to boys.125 Silverthorn and Frick proposed that the childhood-onset form may be the only one that applies to girls, but with one important difference.131 Delinquent adolescent girls appear to have the same antecedents as boys with life course-persistent delinquency, but their conduct problems emerge later than in boys. Thus, it appears that adolescent girls are more likely to fit a “delayed-onset” life course-persistent subtype.
With regard to internalizing symptoms, there is some suggestion that the antecedents of childhood symptoms of depression differ from those of adolescent symptoms of depression.132 Whereas variables indexing the overall family context are associated with symptoms in childhood, factors such as maternal depression (in girls) and lack of supportiveness in the early rearing environment (in boys) were more strongly associated with symptoms during adolescence. On the other hand, it is difficult to determine whether such differences in findings are related more to the question of onset versus maintenance (see previous discussion) or early versus late onset. In the literature on depression, distinctions have also been made between adolescent-onset and adult-onset depression. Those with the former are more likely than those with the latter to have perinatal problems, psychopathology in their family background, caregiver instability, and other mental health problems.133
Resilience
Developmental psychopathologists are interested in understanding the full range of normative and atypical functioning. In fact, researchers have examined a subset of individuals in the normative range: namely, those who function adaptively despite exposure to significant levels of risk and/or adversity (e.g., trauma, social disadvantage, marital transitions, difficult temperament, high genetic loading for psychopathology). Rather than engaging with a maladaptive developmental trajectory (as would be expected, in view of their history), these “resilient” children manage to defy their at-risk status. From a prevention and intervention perspective, children who exhibit resilience are of interest because they can provide much needed information to researchers and interventionists regarding factors that protect at-risk individuals from developing later problems. The issue of resilience is also relevant to the study of multifinality; in children with a particular risk factor (e.g., a substance-abusing parent), outcomes are likely to vary (e.g., substance use vs. normal functioning); one of these outcomes is resilience.134 Moreover, a child may display resilience with regard to one outcome (e.g., academic achievement) but not necessarily with regard to another (e.g., peer relations). Indeed, researchers have found that some inner-city adolescents who have experienced high levels of uncontrolable stress may be resilient in some areas (e.g., school performance, behavioral conduct) but not in others (e.g., they may exhibit high levels of internalizing symptoms).135
How does resilience develop? Researchers and theorists agree that resilience is best viewed as a dynamic process that unfolds over time on the basis of transactions between the individual and the environment rather than as a single variable operating at a single time within a child.102,105 Interestingly, past research suggests that individual and environmental factors that characterize resilient children are similar to those that provide developmental advantages to any child. Superior intellectual functioning, easy temperament, and close relations with caring adults are characteristics that can protect a child exposed to adversity,136 but they provide advantages for other children as well. Also, research by Stouthamer-Loeber and colleagues suggests that protective and risk effects often occur within the same variables, in such a way that scores on one end of a continuum (e.g., superior intellectual functioning) may be protective, whereas scores on the other end of the continuum (e.g., low intellectual functioning) produce higher risk status.137 Also, a variable may be protective by increasing adaptation or by decreasing maladaptation (see more detailed previous discussion of risk, protective, vulnerability, and resource factors).137
Adaptive coping patterns are related to both physical and psychological well-being. Seeking social support has been identified as a beneficial contributor to stress tolerance and has been shown to function as both a mediator and a moderator of stress-illness relations.136,138 Also, the use of problem-focused coping strategies in childhood has been tied to increased resilience to stress later in life.139 The ability to minimize the threat of potential stressors by rationally reappraising oneself or the situation also contributes to stress tolerance.140 In some cases, avoidance, blaming others, and wishful thinking have been shown to be maladaptive coping strategies.141,142 Avoidant coping, specifically, has been linked to distress, depression, mood disturbance, poorer quality of life, and increased pain perception in medical patients.143–145
Key interventions that can build resilience and are especially appropriate as interventions with the chronically ill include creating a flexible narrative about the course of the illness and its effect and meaning for all family members; improving communication within the family to increase understanding and support; and helping the child and family develop a sense of health efficacy.146 Health efficacy (the belief that a person can have a positive influence on his or her own health) can be enhanced when there is an accurate understanding of the illness and its medical and psychosocial consequences. In addition, a proactive stance, such as advocating for appropriate health services, can help families experience a sense of control.146
Comorbidity
Comorbidity involves the presence of two or more disorders within a single individual; the term comorbidity is typically used when disorders co-occur at rates higher than expected from each disorder’s base rate (e.g., ADHD and conduct disorder).102,147 Although some instances of comorbidity may be the result of definitional ambiguities or methodological artifacts,102 comorbidity does seem to occur with regularity in childhood and adolescence. One well-known clustering scheme suggests that there are two broadband categories of psychopathology:148 internalizing problems (i.e., disorders that represent problems within the self, such as depression, anxiety, somatic complaints, and social withdrawal) and externalizing problems (i.e., disorders that represent conflicts with the external environment, such as delinquency, aggression, and other self-control difficulties). Alternatively, Jessor and colleagues proposed that a “problem behavior syndrome” characterizes some children and adolescents, whereby there tend to be high intercorrelations among several types of problem behavior (e.g., drug use, sexual intercourse, drinking, and aggression).149,150 According to problem behavior theory, such behaviors develop as a function of the same etiological factors and, therefore, tend to co-occur in the same individuals (such findings have been replicated in several laboratories; for examples, see Bingham and Crockett151 and Farrell et al152; but see Loeber et al153 for an alternative perspective).
Some studies have shown evidence for comorbidity that combines across the internalizing and externalizing dimensions. For example, Capaldi studied four groups of boys: those with depressed mood only, those with conduct problems only, those with both problems, and those with neither.154 Findings suggested that the poorest adjustment occurred for those with the comorbid problems. Like many who study comorbidity, Capaldi was also interested in whether there was a temporal relationship between the two disorders (in which one disorder precedes the other or in which a common risk factor causes both comorbid disorders).154 Specifically, she found that once a conduct disorder is in place, multiple failures across multiple contexts (i.e., family, peer) place such young adolescents at risk for subsequent depressive symptoms. Similarly, Aseltine and associates examined four groups of participants with presence versus absence of depression and substance use. They found distinctive risk factors for depression, substance use, and their comorbidity.155
The presence of comorbid disruptive disorders (oppositional defiant disorder or conduct disorder) in children with ADHD has been well established.156,157 It has become apparent that internalizing disorders such as depression and anxiety also commonly co-occur with ADHD.156,158,159 In a study of 6- to 12-year-old children with ADHD, a significant comorbidity was found to exist between ADHD-combined type and oppositional defiant disorder/conduct disorder.160 On the other hand, children with ADHD with predominantly inattention symptoms are not as likely to have a comorbid diagnosis of oppositional defiant disorder or conduct disorder.160–162
Person-Environment Fit Research
Person-environment fit theory focuses on the interaction between characteristics of the individual and the environment, whereby the individual not only influences his or her environment, but the environment also affects the individual (see earlier discussion of transactional models). The adequacy of this fit between a person and the environment can affect the person’s motivation, behavior, and overall mental and physical health163; that is, if the fit is optimal, the individual’s functioning may be facilitated; if it is unsuitable, the individual may experience maladaptation. For example, a developmental-behavioral pediatrician may learn that a particular school environment is not providing much needed academic programming for an academically at-risk child. The clinician can intervene, the goal being to maximize the fit between the child’s needs and the schools programming. The importance of person-environment fit with parents can provide a useful rationale when a particular intervention is recommended.
The person-environment fit paradigm has been successfully integrated within a developmental framework. Within this developmental perspective, person-environment fit theory, or, more specifically, stage-environment fit theory, postulates that the combination of an individual’s developmental stage and the surrounding environment produces adaptive change within the individual.164 Proponents of this perspective maintain that synchronizing the trajectory of development to the characteristics and changes in the surrounding environment will encourage positive growth and maturity.163 According to stage-environment fit theory, adaptation is more likely if changes within the individual are matched with supportive change within the child’s three main environments: home, peer, and school.
One environmental change that marks early adolescence is the transition from elementary school to junior high, or middle, school. Several negative changes within the individual have been associated with this transition, such as decreases in motivation, self-concept, and self-confidence, as well as increased academic failure.163 This phenomenon may be a result of several differences between elementary schools and junior high schools that make the latter less developmentally appropriate for students in this age range. In fact, the Michigan Study of Adolescent Life Transitions revealed that, in comparison with elementary schools, junior high schools were characterized by a greater emphasis on discipline and control, fewer opportunities for the students to participate in decision making, less personal and less positive teacher-student relationships, and lower cognitive requirements for assigned tasks.163 Thus, a stage-environment mismatch within the school environment may be associated with some of the negative changes that often occur within the adolescent at this time.
Patterns of change in the adolescent’s home environment are also supportive of the stage-environment hypothesis. During early adolescence, the process of establishing greater independence from parents results in greater conflict and modification of roles between the child and parents.165 Collins postulated that maladaptive conflicts may occur when there is a poor fit between the child’s desire for autonomy and opportunities for such independence.166 Consideration of pubertal development has provided further support for this theory. In general, early-maturing girls report that they are less satisfied with levels of autonomy and decision making provided at home and in school than are their less physically mature peers.163 For children who must adhere to complex medical regimens, the degree of fit between home environment and their readiness to assume some responsibility for self-care can be crucial for adaptive outcomes. Specifically, the degree to which parents can facilitate a sharing of responsibility when a child is developmentally ready can have an effect on subsequent health and important medical outcomes.
Another notable aspect of stage-environment fit is how congruence, or lack thereof, in one environment may affect functioning in another environment. Current research suggests that compatibility of stage-environment match in one setting is associated with functioning in other settings. For example, a positive home environment characterized by involvement in decision making was directly associated with higher intrinsic school motivation in one study.167 This “spillover effect” is appealing from a clinical perspective insofar as positive outcomes that result from an intervention (e.g., increased congruence in the home environment) may yield positive effects in other domains (e.g., academic performance), thus making the intervention more efficient.
Culture and Contextualism
A major question in the literature is this: How do culture and context affect a child’s development trajectory and the development of symptoms? Indeed, research on culture and contextual factors has revealed that there may be individual pathways to psychopathology that vary depending on type of neighborhood, ethnicity, or sociocultural circumstances.168,169 Also, norms for appropriate behavior, as well as the types of processes that are protective, may vary across culture.101 Even help-seeking behaviors appear to vary across cultures (e.g., initial problem identification, choice of treatment provider).170 For example, in many cultures, discussing ailments is negatively viewed as a sign of weakness, particularly if those ailments are not entirely physical in nature. Members of those cultural groups are encouraged to manage their pain internally and often sacrifice the opportunity to receive beneficial support as a result of their silence. In this case, clinicians may miss an important opportunity to gather helpful information about a child’s emotional or behavioral concerns because of the parents’ or the child’s cultural beliefs. In addition, cultural beliefs play a role in the timing of help-seeking behaviors, which perhaps explains a family’s choice to delay treatment. Culture can also limit the types of treatment that clinicians are allowed to provide. Moreover, the effectiveness of interventions promoted by developmental-behavioral pediatricians may depend on the pediatrician’s sensitivity to cultural context and how the intervention is presented to the family. In short, culture appears to play a complex role in all stages of the treatment process.
As a result of demographic changes, minority populations in the United States have steadily increased, which underscores the need to study acculturation and other cultural issues.168 Although culture has been defined as the continual passing of socially transmitted patterns from one generation to another that govern the thoughts, values, and behaviors of individuals in all societies,171 the continually changing role of culture in the lives of children makes it a difficult topic to investigate.168 On the other hand, taking culture into consideration in developmental psychopathology research can help validate and extend current theories of normal development in a number of ways:168 (1) Cultural research can reveal which developmental progressions or associations between predictors and outcomes are culture-specific and which are universal,172 (2) such research can isolate pathways to adaptive and maladaptive outcomes that vary across cultural groups, and (3) research may suggest factors crucial for mental growth that are culture specific versus culturally invariant (e.g., parental warmth appears to be crucial across cultures,172 but “kinship” may be particularly crucial for African-American children173). Garcia Coll and Magnuson called for a paradigm shift in research whereby culture and context would be placed at the core rather than the periphery of understanding and investigating developmental processes.174
A number of issues have yet to be addressed in investigating the role of contextualism in developmental psychopathology. First, more systematic and carefully crafted assessments of cultural context must be used. Future research must “unpack culture” to gain a better understanding of its role in developmental psychopathology.175 Intervention is another area affected by the study of culture and context. Little work has been directed toward understanding and applying culturally sensitive modes of intervention, despite research showing that interventions that incorporate knowledge of cultural issues may be more effective.176,177
A Framework for Understanding Adolescent Development: An Application of Principles of Developmental Psychopathology
Adolescence is a transitional developmental period between childhood and adulthood that is characterized by more biological, psychological, and social role changes than is any other stage of life except infancy.178,179 Indeed, change is the defining feature of adolescence. In view of the many changes that characterize adolescent development, it is not surprising that there are also significant changes in the types and frequency of psychological disorders and problem behaviors that are manifested during adolescence, in comparison with childhood. Moreover, distinctions between normal and abnormal are sometimes less clear during this developmental period than they are in earlier developmental periods.101
As noted, the influence of theories from the field of developmental psychopathology is evident in research on adolescent problem behaviors. Developmentally oriented research has documented the importance of the following for the psychosocial functioning of the child and adolescent:107,126 the timing (early vs. late) of developmental events, the accumulation of multiple events that occur simultaneously and the effect of such accumulation on subsequent trajectories of psychopathology, and the fit between the developmental needs of an adolescent and the adolescent’s environmental context. Contextual perspectives on adolescent psychopathology also have their roots in developmental theory.87
It is our contention that adolescent behavior and psychopathology are best understood within the context of the major tasks of this developmental period. We believe that an appreciation for the rapid developmental changes of adolescence and the contexts of such development will aid developmental-behavioral pediatricians in considering developmental issues in their clinical and research endeavors. The sample framework presented here summarizes major constructs that have been studied by researchers in this field and is based on earlier models presented by the American Psychological Association,180 Hill,181 Holmbeck and colleagues,21,182,183 Steinberg,184 and Grotevant.185 The model is biopsychosocial in nature, insofar as it emphasizes the biological, psychological, and social changes of the adolescent developmental period (Fig. 2-6).186
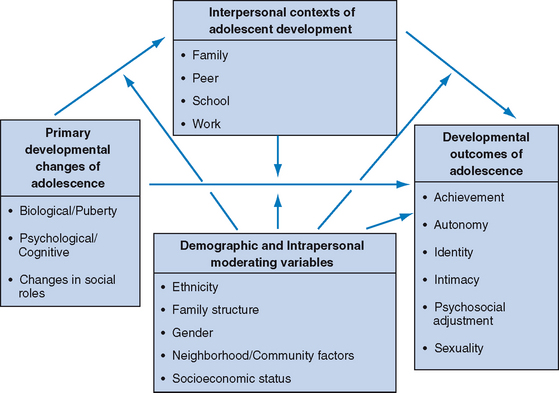
FIGURE 2-6 A framework for understanding adolescent development and adjustment.
(From Holmbeck GN, Shapera WFA: Research methods with adolescents. In Kendall PC, Butcher JN, Holmbeck GN, eds: Handbook of Research Methods in Clinical Psychology, 2nd ed. New York: Wiley, 1999, pp 634-661. Copyright 1999 by John Wiley & Sons, Inc. Reprinted with permission.)
At the most general level, the framework presented in Figure 2-6 indicates that the primary developmental changes of adolescence have an effect on the developmental outcomes of adolescence through the interpersonal contexts in which adolescents develop. In other words, the developmental changes of adolescence (puberty, cognitive, social) have an effect on the behaviors of significant others (family, peers, teachers), which, in turn, influence ways in which adolescents resolve the major issues of adolescence, such as autonomy, sexuality, and identity. Moreover, it is apparent that multifinality would be more the rule than the exception, in view of the multitude of factors noted in the framework that could influence developmental trajectories. Many of the contextual factors noted in the framework could buffer the adolescent from the effects of early risk factors, thus facilitating resilience.
For example, suppose that a young preadolescent girl begins to mature physically much earlier than her age mates. Such early maturity will probably affect her peer relationships, insofar as early-maturing girls are more likely to date and initiate sexual behaviors at an earlier age than are girls who mature on time.187 Such effects on male peers may influence the girl’s own self-perceptions in the areas of identity and sexuality. In this way, the behavior of peers in response to the girl’s early maturity could be said to mediate associations between pubertal change and outcomes such as identity and the trajectories of sexual behaviors (and therefore account, at least in part, for these significant associations).
Such causal and mediational influences may also vary depending on the demographic and intrapersonal contexts in which they occur (see Fig. 2-6, “Demographic and Intrapersonal Moderating Variables”186). Specifically, associations between the primary developmental changes and the developmental outcomes may be moderated by demographic variables such as ethnicity, gender, and socioeconomic status. For example, if associations between pubertal change and certain sexual outcomes held only for girls, investigators could infer that gender moderates such associations. In addition to serving a mediational role as described previously, the interpersonal contexts (i.e., family, peer, school, and work contexts) can also serve a moderating role in the association between the primary changes and the developmental outcomes. For example, early maturity may lead to poor adjustment outcomes only when parents react to early pubertal development in certain ways (e.g., with increased restriction and supervision); in this example, familial reactions to puberty moderate associations between pubertal development and adjustment.
In summary, we have attempted to demonstrate how a developmentally oriented theory (see Fig. 2-6186) can integrate across an array of potential linkages among many developmental changes for a given developmental period (in this case, adolescence). With such a theory, investigators can begin to explain the onset and maintenance of both adaptive and maladaptive behavior over time and formulate hypotheses regarding appropriate points for intervention. Such a model can also guide the developmental-behavioral pediatrician in the information-gathering process as the practitioner attempts to understand, in an organized way, the complex array of influences affecting a given child or adolescent.
THEORIES OF ADJUSTMENT TO CHRONIC ILLNESS
In their comprehensive text on adaptation to childhood chronic illness, Thompson and Gustafson3 trace the history of theorizing in the area of adjustment to chronic illness, beginning with Pless and Pinkerton’s integrated model.13 According to this early theory, adjustment to chronic illness is affected by numerous factors, including intrinsic attributes, coping, self-concept, the family and social environment, an individual’s and others’ responses to the illness, and disability characteristics. Thompson and Gustafson proposed that relations between predictors and adjustment were bidirectional (see previous section on transactional models of development) and cumulative over time. They also noted that an individual’s functioning before diagnosis can have an effect on responses to his or her illness.
A similar early influential theory was Moos and Tsu’s life crisis model.188 They extended Pless and Pinkerton’s work by detailing some of the cognitive events that underlie successful coping with chronic illness. Specifically, they detailed the explanatory importance of cognitive appraisal, or the individual’s understanding and thoughts about his or her own illness. They also described several “adaptive tasks” that follow from appraisals, such as the manner in which a person manages his or her symptoms. Finally, they also identified a variety of coping strategies that individuals may use when adapting to a physical illness, a conceptualization that could be considered a precursor to later conceptualizations of coping (see Thompson and Gustafson for a thorough review3).
More recent conceptual work has expanded and integrated such early conceptual frameworks to account for variations in adjustment to chronic illness. Wallander and Varni’s disability-stress-coping model is a risk-and-resilience framework that identifies a number of “resistance” factors (e.g., intrapersonal factors, stress processing variables, social-ecological factors) that buffer (or exacerbate) the effect of psychosocial stress (both illness-related and non-illness-related stressors) on child adjustment.189 Similarly, Thompson and Gustafson’s transactional stress and coping model identifies adaptational processes residing within the mother and child that buffer the effects of illness on adjustment outcomes.3 Although both these theories have been very influential in providing a basis for many programs of research, these models are not without conceptual difficulties (see Holmbeck for a review16). These models tend to be more “temporal” than causal (which makes them difficult to test). Moreover, there is some confusion over descriptions of moderational and mediational effects, and the focus of Thompson and Gustafson’s model is on mothers, with the exclusion of fathers. With regard to the last point, and as noted by family systems theorists190 and ecological theorists,87 clinicians should take all contexts of the child’s life into account when attempting to understand variations in psychosocial adjustment. Following is an example of a case in which the family, peer, and school contexts are all affected by a chronic condition:
THEORIES OF MEDICAL ADHERENCE
Models of medical adherence have been reviewed by several theorists.1–3,191 One of the most influential theories is the Health Belief Model,192 which focuses on individual perceptions of barriers to satisfactory medical adherence (e.g., cost, time considerations, the degree to which the medical regimen disrupts daily activities) and factors predictive of higher levels of adherence (e.g., realistic perceptions of susceptibility to complications, adequate understanding of the seriousness of the condition, appreciation of the benefits associated with adherence to a medical plan). Analysis of barriers and benefits can often yield a greater understanding of patient adherence across settings, as illustrated in the following case example:
Although the validity of an individual’s self-reports of barriers and benefits has been questioned, some support has been found for the Health Belief Model of medical adherence.2 As yet, however, few interventions exist that have attempted to manipulate these types of “barrier” cognitions.1 A related theory, based on Bandura’s self-efficacy theory,193 suggests that the degree to which individuals believe themselves capable of managing their medical regimen is likely to be predictive of higher levels of adherence.2
Another influential theory (although one that has not received much attention in studies of children with chronic physical conditions) is the transtheoretical model.194 According to this perspective, an individual acquires adherence behaviors over five stages of change:191 (1) precontemplation (i.e., not thinking about changing his or her behavior), (2) contemplation (i.e., thinking about changing his or her behavior at some point in the future), (3) preparation (i.e., considering a change in behavior in the near future), (4) action (i.e., changing his or her behavior), and (5) maintenance (i.e., maintaining the changes made to his or her health behaviors). One potential promise of this stage-oriented approach is that different interventions could be developed for different individuals at varying stages of change. On the other hand, this theory awaits empirical validation with samples of children (see Rapoff for a thorough critique2).
Behavioral theory has played a major role in facilitating a more complete understanding of adherence, especially in children. The term operant conditioning describes the effect that a consequence can have in terms of either strengthening (positively reinforcing) or weakening (negatively reinforcing) a behavior.195 A close analysis of conditions that may support or undermine a person’s adherence to a medical regimen can yield greater understanding and thereby help the professional make informed decisions and recommendations with the goal of improving adherence. Interventions, including behavioral components such as distraction, praise, and incentives, have been found to increase children’s cooperation during painful medical procedures.196
Rapoff concluded his review of models of adherence by noting that theories tend to emphasize one of two processes: cognitive processes (e.g., individual perceptions of barriers, self-efficacy) or environmental contingencies (e.g., parental reinforcement for successful completion of adherence tasks).2 Despite the differing theoretical perspectives, Rapoff argued that the interventions that have been developed on the basis of these various theories have more similarities than their underlying conceptual frameworks would suggest. Specifically, most interventions that focus on medical adherence include the following components: (1) verbal discussions with patients and family members concerning the importance of adherence, (2) a “role model” that demonstrates appropriate levels of adherence, (3) goal setting and goal monitoring, (4) teaching of adherence skills, and (5) strategies to help individuals put into place positive consequences for satisfactory adherence behaviors.
CONCLUSIONS AND FUTURE DIRECTIONS
A second limitation of current theory concerns a lack of emphasis on the mechanisms that operate between the variables. For example, although clinicians know a lot about what risk and protective factors may contribute to various outcomes, they know little as to how these processes operate. More specifically, although they know that children with chronic illnesses are at a heightened risk for behavioral and psychosocial difficulties, they have not yet identified a causal mechanism.197 Future research should aim to uncover processes by which these factors operate.
With regard to theory development, what future directions would be fruitful? The field would benefit greatly from theories that provide seamless linkages between a clearly articulated research-driven, developmentally oriented theory and interventions that follow directly from the constructs and pathways specified in the theory.1 In addition, increased focus on mechanisms of treatment and the delineation of which populations do and do not benefit from specific interventions are needed. Too often, theories lack clarity or include constructs that have little relevance to the interventionist. Simply put, theories should be conceived with the interventionist in mind.
Although the importance of Bronfenbrenner’s biopsychosocial model87 and the role of transactional influences have been recognized, the application of these theories has been limited. These theoretical models are especially salient in view of improved rates of survival in pediatric conditions that were previously considered fatal (e.g., spina bifida, cancer, human immunodeficiency virus [HIV] infection) and increased incidence rates of other chronic conditions (e.g., obesity). Therefore, more attention to transactional processes between pediatric conditions and various contexts surrounding the child throughout the lifespan is necessary. For instance, theories focusing on mechanisms of intervention should be expanded to include their influence on surrounding systems and their indirect effects on the child’s adjustment.198 In addition, more theory is needed to address (1) how cultural beliefs and practices used in various contexts interact over time, (2) the influence of the health care system on family and individual functioning, (3) transactional interactions between peers and children and their effects on psychosocial adjustment, and (4) effects of financial forces on the various contexts affecting the child’s development.199
1 Riekert KA, Drotar D. Adherence to medical treatment in pediatric chronic illness: Critical issues and answered questions. In: Drotar D, editor. Promoting Adherence to Medical Treatment in Chronic Childhood Illness. Mahwah, NJ: Erlbaum; 2000:3-32.
2 Rapoff MA. Adherence to Pediatric Medical Regimens. New York: Kluwer, 1999.
3 Thompson RJ, Gustafson KE. Adaptation to Chronic Childhood Illness. Washington, DC: American Psychological Association, 1996.
4 Eyberg S, Schuhmann E, Rey J. Psychosocial treatment research with children and adolescents: Developmental issues. J Abnorm Child Psychol. 1998;26:71-81.
5 Kazdin AE. Psychotherapy for children and adolescents: Current progress and future research directions. Am Psychol. 1993;48:644-657.
6 Kessen W. The development of behavior. In: Levine MD, Carey WB, Crocker AC, editors. Developmental-Behavioral Pediatrics. Philadelphia: WB Saunders; 1999:1-13.
7 Levine MD, Carey WB, Crocker AC. Developmental-Behavioral Pediatrics. Philadelphia: WB Saunders Company, 1999.
8 Meehl PE. Theoretical risks and tabular asterisks: Sir Karl, Sir Ronald, and the slow progress of soft psychology. J Consult Clin Psychol. 1978;46:806-834.
9 Platt JR. Strong inference. Science. 1964;146:347-353.
10 Popper KR. The Logic of Scientific Discovery. New York: Harper, 1965.
11 Miller PH. Theories of Developmental Psychology. San Francisco: Freeman, 1983.
12 Lilienfeld SO. When worlds collide: Social science, politics, and the Rind et al (1998) child sexual abuse meta-analysis. Am Psychol. 2002;57:176-188.
13 Pless IB, Pinkerton P. Chronic Childhood Disorders: Promoting Patterns of Adjustment. Chicago: Year Book Medical, 1975.
14 Wallander JL, Varni JW, Babani L, et al. Family resources as resistance factors for psychological maladjustment in chronically ill and handicapped children. J Pediatr Psychol. 1989;14:157-173.
15 Thompson RJ, Gustafson KE, George LK, et al. Change over a 12-month period in the psychosocial adjustment of children and adolescents with cystic fibrosis. J Pediatr Psychol. 1994;19:189-203.
16 Holmbeck GN. Toward terminological, conceptual, and statistical clarity in the study of mediators and moderators: Examples from the child-clinical and pediatric psychology literatures. J Consult Clin Psychol. 1997;65:599-610.
17 Wallander JL, Thompson RJ, Alriksson-Schmidt A. Psychosocial adjustment of children with chronic physical conditions. In: Roberts MC, editor. Handbook of Pediatric Psychology. New York: Guilford; 2003:141-158.
18 Rose BM, Holmbeck GN, Coakley RM, Franks EA. Mediator and moderator effects in developmental and behavioral pediatric research. J Dev Behav Pediatr. 2004;25:1-10.
19 Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51:1173-1182.
20 Holmbeck GN. Post-hoc probing of significant moderational and mediational effects in studies of pediatric populations. J Pediatr Psychol. 2002;27:87-96.
21 Holmbeck GN, Johnson SZ, Wills KE, et al. Observed and perceived parental overprotection in relation to psychosocial adjustment in preadolescents with a physical disability: The mediational role of behavioral autonomy. J Consult Clin Psychol. 2002;70:96-110.
22 Holmes CS, Yu Z, Frentz J. Chronic and discrete stress as predictors of children’s adjustment. J Consult Clin Psychol. 1999;67:411-419.
23 Masten AS, Hubbard JJ, Gest SD, et al. Competence in the context of adversity: Pathways to resilience and maladaptation from childhood to late adolescence. Dev Psychopathol. 1999;11:143-169.
24 Rutter M. Psychosocial resilience and protective mechanisms. In: Rolf J, Masten AS, Cicchetti D, et al, editors. Risk and Protective Factors in the Development of Psychopathology. New York: Cambridge University Press; 1990:181-214.
25 Masten AS. Ordinary magic: Resilience processes in development. Am Psychol. 2001;56:227-238.
26 Stouthamer-Loeber M, Loeber R, Wei E, et al. Risk and promotive effects in the explanation of persistent serious delinquency in boys. J Consult Clin Psychol. 2002;70:111-123.
27 McGee RA, Wolfe DA, Wilson SK. Multiple maltreatment experiences and adolescent behavior problems: Adolescents’ perspectives. Dev Psychopathol. 1997;9:131-149.
28 Gorman-Smith D, Tolan P. The role of exposure to community violence and developmental problems among inner-city youth. Dev Psychopathol. 1998;10:101-116.
29 Tolan PH, Gorman-Smith D, Henry DB. The developmental ecology of urban males’ youth violence. Dev Psychol. 2003;39:274-291.
30 Woodward LJ, Fergusson DM. Early conduct problems and later risk of teenage pregnancy in girls. Dev Psychopathol. 1999;11:127-141.
31 Clingempeel WG, Henggeler SW. Randomized clinical trials, developmental theory, and antisocial youths: Guidelines for research. Dev Psychopathol. 2002;14:695-711.
32 Howe GW, Reiss D, Yuh J. Can prevention trials test theories of etiology? Dev Psychopathol. 2002;14:673-694.
33 Kraemer HC, Wilson T, Fairburn CG, et al. Mediators and moderators of treatment effects in randomized clinical trials. Arch Gen Psychiatry. 2002;59:877-883.
34 Rutter M, Pickles A, Murray R, et al. Testing hypotheses on specific environmental causal effects on behavior. Psychol Bull. 2001;127:291-324.
35 Weersing VR, Weisz JR. Mechanisms of action in youth psychotherapy. J Child Psychol Psychiatry. 2002;43:3-29.
36 Collins WA, Maccoby EE, Steinberg L, et al. Contemporary research on parenting: The case for nature and nurture. Am Psychol. 2000;55:218-232.
37 Kraemer HC, Stice E, Kazdin A, et al. How do risk factors work together? Mediators, moderators, and independent, overlapping, and proxy risk factors. Am J Psychiatry. 2001;158:848-856.
38 Forgatch MS, DeGarmo DS. Parenting through change: An effective prevention program for single mothers. J Consult Clin Psychol. 1999;67:711-724.
39 Dixon RA, Lerner RM. History and systems in developmental psychology. In: Bornstein MH, Lamb ME, editors. Developmental Psychology: An Advanced Textbook. Mahwah, NJ: Erlbaum; 1999:3-46.
40 Parke RD, Ornstein PA, Rieser JJ, et al. The past as prologue: An overview of a century of developmental psychology. In: Parke RD, Ornstein PA, Rieser JJ, et al, editors. A Century of Developmental Psychology. Washington, DC: American Psychological Association; 1994:1-72.
41 Shaffer DR. Developmental Psychology: Childhood and Adolescence. Belmont, CA: Thomson Learning, 2002.
42 Darwin C. A biological sketch of an infant. Mind. 1877;2:285-294.
43 Boyce WT, Ellis BJ. Biological sensitivity to context: I. An evolutionary-developmental theory of the origins of stress reactivity. Dev Psychopathol. 2005;17:271-301.
44 Hall GS. Adolescence: Its Psychology and Its Relations to Psychology, Anthropology, Sex, Crime, Religion, and Education. New York: Appleton-Century-Crofts; 1904;2.
45 White SH, Stanley Hall G. From philosophy to developmental psychology. In: Parke RD, Ornstein PA, Rieser JJ, et al, editors. A Century of Developmental Psychology. Washington, DC: American Psychological Association; 1994:103-126.
46 Freud S. The Basic Writings of Sigmund Freud. New York: TheModern Library, 1938.
47 Thelen E, Adolph KE. Arnold L. Gesell: The paradox of nature and nurture. In: Parke RD, Ornstein PA, Rieser JJ, et al, editors. A Century of Developmental Psychology. Washington, DC: American Psychological Association; 1994:357-388.
48 Gesell A. Infancy and Human Growth. New York: Macmillan, 1929.
49 Beilin H. Piaget’s enduring contribution to developmental psychology. In: Parke RD, Ornstein PA, Rieser JJ, et al, editors. A Century of Developmental Psychology. Washington, DC: American Psychological Association; 1994:257-290.
50 Piaget J. Genetic Epistemology. New York: Columbia University Press, 1970.
51 Piaget J. Intellectual evolution from adolescence to adulthood. Hum Dev. 1972;15:1-12.
52 Piaget J. Piaget’s theory. In: Kessen W, Mussen PH, editors. Handbook of Child Psychology, Volume 1: History, Theory, and Methods. New York: Wiley; 1983:103-128.
53 Daniels H. Introduction: Psychology in a social world. In: Daniels H, editor. An Introduction to Vygotsky. New York: Routledge; 1996:1-27.
54 Wertsch JV, Tulviste P. L.S. Vygotsky and contemporary developmental psychology. In: Daniels H, editor. An Introduction to Vygotsky. New York: Routledge; 1996:53-74.
55 Vygotsky L. Mind in Society: The Development of Higher Psychological Processes. Cambridge, MA: Harvard University Press, 1978.
56 Ellis BJ, Essex MJ, Boyce WT. Biological sensitivity to context: II. Empirical exploration of an evolutionary-developmental theory. Dev Psychopathol. 2005;17:303-328.
57 Suomi SJ. Early determinants of behavior: Evidence from primate studies. Br Med Bull. 1997;53:170-184.
58 Grossman AW, Churchill JD, McKinney BC, et al. Experience effects on brain development: Possible contributions to psychopathology. J Child Psychol Psychiatry. 2003;44:33-63.
59 Waddington CH. The Strategy of the Genes. London: Allen & Unwin, 1957.
60 O’Connor TG, Plomin R. Developmental behavior genetics. In: Sameroff AJ, Lewis M, editors. Handbook of Developmental Psychopathology. New York: Plenum Press; 2000:217-235.
61 Rende R, Plomin R. Nature, nurture, and the development of psychopathology. In: Cicchetti D, Cohen DJ, editors. Developmental Psychopathology, Volume 1: Theory and Methods. New York: Wiley; 1995:291-314.
62 Rutter M, Sroufe LA. Developmental psychopathology: Concepts and challenges. Dev Psychopathol. 2000;12:265-296.
63 Plomin R, Rutter M. Child development, molecular genetics, and what to do with genes once they are found. Child Dev. 1998;69:1223-1242.
64 Caspi A, McClay J, Moffitt TE, et al. Role of genotype in the cycle of violence in maltreated children. Science. 2002;297:851-855.
65 Caspi A, Sugden K, Moffitt TE, et al. Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science. 2003;301:386-390.
66 Hankin BL, Abramson LY. Development of gender differences in depression: An elaborated cognitive vulnerability-transactional stress theory. Psychol Bull. 2001;127:773-796.
67 Silberg J, Rutter M, Neale M, Eaves L. Genetic moderation of environmental risk for depression and anxiety in adolescent girls. Br J Psychiatry. 2001;179:116-121.
68 Thapar A, McGuffin P. The genetic etiology of childhood depressive symptoms: A developmental perspective. Dev Psychopathol. 1996;8:751-760.
69 Scarr S, McCartney K. How people make their own environments: A theory of genotype to environment effects. Child Dev. 1983;54:1-19.
70 Rowe DC, Jacobson KC, Van Den Oord JCG. Genetic and environmental influences on vocabulary IQ: Parental education level as moderator. Child Dev. 1999;70:1151-1162.
71 Pike A, Plomin R. Importance of nonshared environmental factors for childhood and adolescent psychopathology. J Am Acad Child Adolesc Psychiatry. 1996;35:560-570.
72 O’Connor TG, McGuire S, Reiss D, et al. Cooccurrence of depressive symptoms and antisocial behavior in adolescence: A common genetic liability. J Abnorm Psychol. 1998;107:27-37.
73 Deater-Deckard K, Plomin R. An adoption study of etiology of teacher and parent reports of externalizing behavior problems in middle childhood. Child Dev. 1999;70:144-154.
74 Rende R, Plomin R, Reiss D, et al. Genetic and environmental influences on depressive symptomatology in adolescence: Individual differences and extreme scores. J Child Psychol Psychiatry. 1993;34:1387-1398.
75 Iervolino AC, Pike A, Manke B, et al. Genetic and environmental influences in adolescent peer socialization: Evidence from two genetically sensitive designs. Child Dev. 2002;73:162-174.
76 Reiss D, Hetherington EM, Plomin R, et al. Genetic questions for environmental studies: Differential parenting of siblings and its association with depression and antisocial behavior in adolescence. Arch Gen Psychiatry. 1995;52:925-936.
77 Neiderhiser JM, Reiss D, Hetherington EM, et al. Relationships between parenting and adolescent adjustment over time: Genetic and environmental contributions. Dev Psychol. 1999;35:680-692.
78 Plomin R, Reiss D, Hetherington EM, et al. Nature and nurture: Genetic contributions to measures of the family environment. Dev Psychol. 1994;30:32-43.
79 O’Connor TG, Deater-Deckard K, Fulker D, et al. Genotype-environment correlations in late childhood and early adolescence: Antisocial behavioural problems and coercive parenting. Dev Psychol. 1998;34:970-981.
80 Jackson FJ. Human behavioral genetics, Scarr’s theory, and her views on interventions: A critical review and commentary on their implications for African-American children. Child Dev. 1993;64:1318-1332.
81 Maccoby E. Parenting and its effects on children: On reading and misreading behavior genetics. Annu Rev Psychol. 2000;51:1-27.
82 Steinberg L, Morris AS. Adolescent development. Annu Rev Psychol. 2001;52:83-110.
83 Saudino KJ. Behavioral genetics and child temperament. J Dev Behav Pediatr. 2005;26:214-223.
84 Thomas A, Chess B, Birch HG, et al. Behavioral Individuality in Early Childhood. New York: New York University Press, 1963.
85 Bell RQ. A reinterpretation of the direction of effects in studies of socialization. Psychol Rev. 1968;75:81-95.
86 Thomas A, Chess B, Birch HG. Temperament and behavior disorders in children. Oxford, UK: New York University Press, 1968.
87 Bronfenbrenner U. The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press, 1979.
88 Crockenberg SB. Infant irritability, mother responsiveness, and social support influences on the security of infant-mother attachment. Child Dev. 1981;52:857-865.
89 Dodge KA, Pettit GS. A biopsychosocial model of the development of chronic conduct problems in adolescence. Dev Psychol. 2003;39:349-371.
90 Sameroff AJ, Peck SC, Eccles JS. Changing ecological determinants of conduct problems from early adolescence to early adulthood. Dev Psychopathol. 2004;16:873-896.
91 Anderson KE, Lytton H, Romney DM. Mothers’ interactions with normal and conduct-disordered boys: Who affects whom? Dev Psychol. 1986;22:604-609.
92 Patterson GR. Performance models for antisocial boys. Am Psychol. 1986;41:432-444.
93 Johnston C, Mash EJ. Families of children with attention-deficit/hyperactivity disorder: Review and recommendations for future research. Clin Child Fam Psychol Rev. 2001;4:183-207.
94 Wachtel PL. Cyclical processes in personality and psychopathology. J Abnorm Psychol. 1994;103:51-54.
95 Sameroff A. Developmental systems and family functioning. In: Parke RD, Kellam SG, editors. Exploring Family Relationships with Other Social Contexts. Hillsdale, NJ: Erlbaum; 1994:199-214.
96 Sameroff AJ. Developmental systems and psychopathology. Dev Psychopathol. 2000;12:297-312.
97 Kazdin AE. Problem-solving skills training and parent management training for conduct disorder. In: Kazdin AE, Weisz JR, editors. Evidence-Based Psychotherapies for Children and Adolescents. New York: Guilford; 2003:241-262.
98 Kazdin AE, Weisz JR. Identifying and developing empirically supported child and adolescent treatments. J Consult Clin Psychol. 1998;66:19-36.
99 Van Den Boom DC. Neonatal irritability and the development of attachment. In: Kohnstamm GA, Bates JE, Rothbart MK, editors. Temperament in Childhood. Chichester, UK: Wiley; 1989:299-318.
100 Cicchetti D, Rogosch FA. Conceptual and methodological issues in developmental psychopathology research. In: Kendall PC, Butcher JN, Holmbeck GN, editors. Handbook of Research Methods in Clinical Psychology. 2nd ed. New York: Wiley; 1999:433-465.
101 Cicchetti D, Rogosch FA. A developmental psychopathology perspective on adolescence. J Consult Clin Psychol. 2002;70:6-20.
102 Mash EJ, Dozois DJA. Child psychopathology: A developmental-systems perspective. In: Mash EJ, Barkley RA, editors. Child Psychopathology. 2nd ed. New York: Guilford; 2003:3-71.
103 Kazdin AE, Kraemer HC, Kessler RC, et al. Contributions of risk-factor research to developmental psychopathology. Clin Psychol Rev. 1997;17:375-406.
104 Sroufe LA. Considering normal and abnormal together: The essence of developmental psychopathology. Dev Psychopathol. 1990;2:335-347.
105 Sroufe LA. Pychopathology as an outcome of development. Dev Psychopathol. 1997;9:251-268.
106 Sroufe LA, Carlson EA, Levy AK, et al. Implications of attachment theory for developmental psychopathology. Dev Psychopathol. 1999;11:1-13.
107 Graber JA, Brooks-Gunn J. Transitions and turning points: Navigating the passage from childhood through adolescence. Dev Psychol. 1996;32:768-776.
108 Steinberg L, Avenevoli S. The role of context in the development of psychopathology: A conceptual framework and some speculative propositions. Child Dev. 2000;71:66-74.
109 Schulenberg J, Wadsworth KN, O’Malley PM, et al. Adolescent risk factors for binge drinking during the transition to young adulthood: Variable- and pattern-centered approaches to change. Dev Psychol. 1996;32:659-674.
110 Cicchetti D, Rogosch FA. Equifinality and multifinality in developmental psychopathology. Dev Psychopathol. 1996;8:597-600.
111 Marsh P, McFarland FC, Allen JP, et al. Attachment, autonomy, and multifinality in adolescent internalizing and risky behavioral symptoms. Dev Psychopathol. 2003;15:451-467.
112 Harrington R, Rutter M, Fombonne E. Developmental pathways in depression: Multiple meanings, antecedents, and endpoints. Dev Psychopathol. 1996;8:601-616.
113 Bardone AM, Moffitt TE, Caspi A, et al. Adult mental health and social outcomes of adolescent girls with depression and conduct disorder. Dev Psychopathol. 1996;8:811-829.
114 Gjerde PF, Block J. A developmental perspective on depressive symptoms in adolescence: Gender differences in autocentric-allocentric modes of impulse regulation. Cicchetti D, Toth SL, editors. Adolescence: Opportunities and Challenges. Rochester, NY: University of Rochester Press; 1996;7:167-196.
115 Lacourse E, Nagin D, Tremblay RE, et al. Developmental trajectories of boys’ delinquent group membership and facilitation of violent behaviors during adolescence. Dev Psychopathol. 2003;15:183-197.
116 Zucker RA, Ellis DA, Fitzgerald HE, et al. Other evidence for at least two alcoholisms II: Life course variation in antisociality and heterogeneity of alcoholic outcome. Dev Psychopathol. 1996;8:831-848.
117 Broidy LM, Nagin DS, Tremblay RE, et al. Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: A six-site, cross-national study. Dev Psychol. 2003;39:222-245.
118 Bergman LR, Magnusson D. A person-oriented approach in research on developmental psychopathology. Dev Psychopathol. 1997;9:291-319.
119 Garber J, Keiley MK, Martin NC. Developmental trajectories of adolescents’ depressive symptoms: Predictors of change. J Consult Clin Psychol. 2002;70:79-95.
120 Brennan PA, Hall J, Bor W, et al. Integrating biological and social processes in relation to early-onset persistent aggression in boys and girls. Dev Psychol. 2003;39:309-323.
121 Brook JS, Kessler RC, Cohen P. The onset of marijuana use from preadolescence and early adolescence to young adulthood. Dev Psychopathol. 1999;11:901-914.
122 Patterson GR, Forgatch MS, Yoerger KL, et al. Variables that initiate and maintain an early-onset trajectory for juvenile offending. Dev Psychopathol. 1998;10:531-547.
123 Hammen C. Cognitive, life stress, and interpersonal approaches to a developmental psychopathology model of depression. Dev Psychopathol. 1992;4:189-206.
124 Petersen AC, Compas BE, Brooks-Gunn J, et al. Depression in adolescence. Am Psychol. 1993;48:155-168.
125 Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychol Rev. 1993;100:674-701.
126 Moffitt TE, Caspi A, Dickson N, et al. Childhood-onset versus adolescent-onset antisocial conduct problems in males: Natural history from ages 3 to 18 years. Dev Psychopathol. 1996;8:399-424.
127 Aguilar B, Sroufe LA, Egeland B, et al. Distinguishing the early-onset/persistent and adolescence-onset antisocial behavior types: From birth to 16 years. Dev Psychopathol. 2000;12:109-132.
128 Moffitt TE, Caspi A, Harrington H, et al. Males on the life-course-persistent and adolescence-limited antisocial pathways: Follow-up at age 26 years. Dev Psychopathol. 2002;14:179-207.
129 Zucker RA, Fitzgerald HE, Moses HD. Emergence of alcohol problems and the several alcoholisms: A developmental perspective on etiologic theory and life course trajectory. In: Cicchetti D, Cohen D, editors. Developmental Psychopathology, Volume 2: Risk, Disorder, and Adaptation. New York: Wiley; 1995:677-711.
130 Schulenberg J, Maggs JL, Hurrelmann K. Negotiating developmental transitions during adolescence and young adulthood: Health risks and opportunities. In: Schulenberg J, Maggs JL, Hurrelmann K, editors. Health Risks and Developmental Transitions during Adolescence. Cambridge, UK: Cambridge University Press; 1997:1-19.
131 Silverthorn P, Frick PJ. Developmental pathways to antisocial behavior: The delayed-onset pathway in girls. Dev Psychopathol. 1999;11:101-126.
132 Duggal S, Carlson EA, Sroufe LA, Egeland B. Depressive symptomatology in childhood and adolescence. Dev Psychopathol. 2001;13:143-164.
133 Jaffee SR, Moffitt TE, Caspi A, et al. Differences in early childhood risk factors for juvenile-onset and adult-onset depression. Arch Gen Psychiatry. 2002;59:215-222.
134 Cicchetti D, Rogosch FA. Psychopathology as risk for adolescent substance use disorders: A developmental psychopathology perspective. J Clin Child Psychol. 1999;28:355-365.
135 Luthar SS, Doernberger CH, Zigler E. Resilience is not a unidimensional construct: Insights from a prospective study of inner-city adolescents. Dev Psychopathol. 1993;5:703-717.
136 Masten AS, Coatsworth JD. The development of competence in favorable and unfavorable environments: Lessons from research on successful children. Am Psychol. 1998;53:205-220.
137 Stouthamer-Loeber M, Loeber R, Farrington DP, et al. The double edge of protective and risk factors for delinquency: Interrelations and developmental patterns. Dev Psychopathol. 1993;5:683-701.
138 Taylor SE, Klein LC, Lewis BP, et al. Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychol Rev. 2000;107:411-429.
139 Cederblad M, Dahlin L, Hagnell O, et al. Salutogenic childhood factors reported by middle-aged individuals. Eur Arch Psychiatry Clin Neurosci. 1994;244:1-11.
140 Isaacowitz DM, Seligman ME. Cognitive styles and well-being in adulthood and old age. In: Bornstein MH, Davidson L, editors. Well-Being: Positive Development Across the Life Course: Crosscurrents in Contemporary Psychology. Mahwah, NJ: Erlbaum; 2003:449-475.
141 Vitaliano PP, DeWolfe DJ, Maiuro RD, et al. Appraised changeability of a stressor as a modifier of the relationship between coping and depression: A test of the hypothesis of fit. J Pers Soc Psychol. 1990;59:582-592.
142 Vitaliano PP, Maiuro RD, Russo J, et al. Coping profiles associated with psychiatric, physical health, work, and family problems. Health Psychol. 1990;9:348-376.
143 Carver CS, Pozo C, Harris SD, et al. How coping mediates the effect of optimism on distress: A study of women with early stage breast cancer. J Pers Soc Psychol. 1993;65:375-390.
144 Culver JL, Arena PL, Antoni MH, et al. Coping and distress among women and under treatment for early stage breast cancer: Comparing African Americans, Hispanics, and non-Hispanic whites. Psychooncology. 2002;11:495-504.
145 Penedo FJ, Gonzalez JS, Davis C, et al. Coping and psychological distress among symptomatic HIV+ men who have sex with men. Ann Behav Med. 2003;25:203-213.
146 Shapiro ER. Chronic illness as a family process: A social-developmental approach to promoting resilience. J Clin Psychol. 2002;58:1375-1384.
147 Hinshaw SP, Lahey BB, Hart EL. Issues of taxonomy and comorbidity in the development of conduct disorder. Dev Psychopathol. 1993;5:31-49.
148 Achenbach TM. Assessment and Taxonomy of Child and Adolescent Psychopathology, Volume 3: Developmental Clinical Psychology and Psychiatry. Beverly Hills, CA: Sage Publications, 1985.
149 Jessor R, Donovan JE, Costa FM. Beyond Adolescence: Problem Behavior and Young Adult Development. New York: Cambridge University Press, 1991.
150 Jessor R, Jessor SL. Problem Behavior and Psychosocial Development: A Longitudinal Study of Youth. New York: Academic Press, 1977.
151 Bingham CR, Crockett LJ. Longitudinal adjustment patterns of boys and girls experiencing early, middle, and late sexual intercourse. Dev Psychol. 1996;32:647-658.
152 Farrell AD, Danish SJ, Howard CW. Relationship between drug use and other problem behaviors in urban adolescents. J Consult Clin Psychol. 1992;60:705-712.
153 Loeber R, Farrington DP, Stouthamer-Loeber M, et al. Antisocial Behavior and Mental Health Problems: Explanatory Factors in Childhood and Adolescence. Mahwah, NJ: Erlbaum, 1998.
154 Capaldi DM. Cooccurrence of conduct problems and depressive symptoms in early adolescent boys: I. Familial factors and general adjustment at grade 6. Dev Psychopathol. 1991;3:277-300.
155 Aseltine RH, Gore S, Colten ME. The cooccurrence of depression and substance abuse in late adolescence. Dev Psychopathol. 1998;10:549-570.
156 Bird H, Gould M, Staghezza-Jaramillo B. The comorbidity of ADHD in a community sample of children aged 6 through 16 years. J Child Fam Stud. 1990;3:365-378.
157 Hinshaw SP. On the distinction between attentional problems/hyperactivity and conduct problems/aggression in child psychopathology. Psychol Bull. 1987;101:443-463.
158 Biederman J, Newcorn J, Sprich S. Comorbidity of attention deficit hyperactivity disorder with conduct, depressive, anxiety, and other disorders. Am J Psychiatry. 1991;148:564-577.
159 A 14-month randomized clinical trial of treatment strategies for attention deficit hyperactivity disorder. The MTA Cooperative Group. Multimodal treatment study of children with ADHD. Arch Gen Psychiatry. 1999;56:1073-1086.
160 Eiraldi RB, Power TJ, Nezu CM. Patterns of comorbidity associated with subtypes of attention-deficit/hyper-activity disorder among 6- to 12-year-old children. J Am Acad Child Adolesc Psychiatry. 1997;36:503-514.
161 Barkley RA. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York: Guilford, 1990.
162 Cantwell DP, Baker L. Attention deficit disorder with and without hyperactivity: A review and comparison of matched groups. J Am Acad Child Adolesc Psychiatry. 1992;31:432-438.
163 Eccles JS, Midgley C, Wigfield A, et al. Development during adolescence: The impact of stage-environment fit in young adolescents’ experiences in schools and in families. Am Psychol. 1993;48:90-101.
164 Eccles JS, Midgley C. Stage-environment fit: Developmentally appropriate classrooms for young adolescents. Ames C, Ames R, editors. Researchon Motivation in Education: Goals and Cognitions. San Diego, CA: Academic Press; 1989;3:139-186.
165 Fuligni AJ, Eccles JS. Perceived parent-child relationships and early adolescents’ orientation toward peers. Dev Psychol. 1993;29:622-632.
166 Collins WA. Parent-child relationships in the transition to adolescence: Continuity and change in interaction, affect, and cognition. Montemayor R, Adams G, Gullotta T, editors. Advances in Adolescent Development: From Childhood to Adolescence: A Transitional Period?. Beverly Hills, CA: Sage Publications; 1990;2:85-106.
167 Eccles JS, Buchanan CM, Flanagan C, et al. Control versus autonomy during early adolescence. J Soc Issues. 1991;47:53-68.
168 Garcia Coll CT, Akerman A, Cicchetti D. Cultural influences on developmental processes and outcomes: Implications for the study of development and psychopathology. Dev Psychopathol. 2000;12:333-356.
169 Rutter M. Antisocial behavior: developmental psychopathology perspectives. In: Stoff DM, Breiling J, editors. Handbook of Antisocial Behavior. New York: Wiley; 1997:115-124.
170 Cauce AM, Domenech-Rodriguez M, Paradise M, et al. Cultural and contextual influences in mental health help-seeking: A focus on ethnic minority youth. J Consult Clin Psychol. 2002;70:44-45.
171 Hallowell AI. Culture and mental disorder. J Abnorm Soc Psychol. 1934;29:1-9.
172 Greenberger E, Chen C. Perceived family relationships and depressed mood in early and late adolescence: A comparison of European and Asian Americans. Dev Psychol. 1996;32:707-716.
173 Taylor RD. Adolescents’ perceptions of kinship support and family management practices: Association with adolescent adjustment in African American families. Dev Psychol. 1996;32:687-695.
174 Garcia Coll CT, Magnuson K. Cultural influences on child development: Are we ready for a paradigm shift?. Nelson C, Masten A, editors. Minnesota Symposium on Child Psychology. Mahwah, NJ: Erlbaum; 1999;29:1-24.
175 Cooper CR, Jackson JF, Azmitia M, et al. Multiple selves, multiple worlds: Three useful strategies for research with ethnic minority youth on identity, relationships, and opportunity structures. In: McLoyd VC, Steinberg L, editors. Studying Minority Adolescents: Conceptual, Methodological, and Theoretical Issues. Hillsdale, NJ: Erlbaum; 1998:111-125.
176 Sameroff A, Fiese B. Transactional regulation and early interaction. In: Meisels S, Shonkoff J, editors. Handbook of Early Intervention. New York: Cambridge University Press; 1990:119-149.
177 Toth SL, Cicchetti D. Developmental psychopathology and child psychotherapy. In: Russ S, Ollendick T, editors. Handbook of Psychotherapies with Children and Families. New York: Plenum Press; 1999:15-44.
178 Feldman SS, Elliott GR, editors. At the Threshold: The Developing Adolescent. Cambridge, MA: Harvard University Press, 1990.
179 Holmbeck GN, Colder C, Shapera W, et al. Working with adolescents: Guides from developmental psychology. In: Kendall PC, editor. Child & Adolescent Therapy: Cognitive-Behavioral Procedures. 2nd ed. New York: Guilford; 2000:334-385.
180 American Psychological Association. Developing Adolescents: A Reference for Professionals. Washington, DC: American Psychological Association, 2002.
181 Hill JP. Understanding Early Adolescence: A Framework. Carrboro, NC: Center for Early Adolescence, 1980.
182 Holmbeck GN. A model of family relational transformations during the transition to adolescence: Parent-adolescent conflict and adaptation. In: Graber JA, Brooks-Gunn J, Petersen AC, editors. Transitions through Adolescence: Interpersonal Domains and Context. Mahwah, NJ: Erlbaum; 1996:167-199.
183 Holmbeck GN, Updegrove AL. Clinical-developmental interface: Implications of developmental research for adolescent psychotherapy. Psychotherapy. 1995;32:16-33.
184 Steinberg L. Adolescence, 6th ed. Boston, MA: McGraw-Hill, 2002.
185 Grotevant HD. Adolescent development in family contexts. In: Damon W, Eisenberg N., editors. Handbook of Child Psychology, vol 3: Social, Emotional and Personality Development. New York: Wiley; 1997:1097-1149.
186 Holmbeck GN, Shapera WFA. Research methods with adolescents. In: Kendall PC, Butcher JN, Holmbeck GN, editors. Handbook of Research Methods in Clinical Psychology. 2nd ed. New York: Wiley; 1999:634-661.
187 Magnusson D, Stattin H, Allen VL. A longitudinal study of some adjustment processes from mid-adolescence to adulthood. J Youth Adolesc. 1985;14:267-283.
188 Moos RH, Tsu UD. The crisis of physical illness: An overview. In: Moos RH, editor. Coping with Physical Illness. New York: Plenum Press; 1977:3-21.
189 Wallander JL, Varni JW. Effects of pediatric chronic physical disorders on child and family adjustment. J Child Psychol Psychiatry. 1997;39:29-46.
190 Fiese BH, Sameroff AJ. Family context in pediatric psychology: A transactional perspective. In: Roberts MC, Wallander JL, editors. Family Issues in Pediatric Psychology. Hillsdale, NJ: Erlbaum; 1992:239-260.
191 La Greca AM, Bearman KJ. Adherence to pediatric treatment regimens. In: Roberts MC, editor. Handbook of Pediatric Psychology. New York: Guilford; 2003:119-140.
192 Becker MH, Maiman LA, Kirscht JP, et al. Patient perceptions and compliance: Recent studies of the health belief model. In: Haynes RB, Taylor DW, Sackett DL, editors. Compliance in Health Care. Baltimore, MD: TheJohns Hopkins University Press; 1979:78-109.
193 Bandura A. Self-Efficacy: The Exercise of Control. New York: Freeman, 1997.
194 Prochaska JL, DiClemente CC. The Transtheoretical Approach: Crossing Traditional Boundaries of Change. Homewood, IL: Dorsey, 1984.
195 Skinner BF. Science and Human Behavior. New York: Macmillan, 1953.
196 Powers SW. Empirically supported treatments in pediatric psychology: Procedure-related pain. J Pediatr Psychol. 1999;24:131-145.
197 Fiese BH, Wilder J, Bickham NL. Family context in developmental psychopathology. In: Sameroff AJ, Lewis M, Miller SM, editors. Handbook of Developmental Psychopathology. 2nd ed. Dordrecht, The Netherlands: Kluwer; 2000:115-134.
198 Sameroff AJ, MacKenzie MJ. Research strategies for capturing transactional models of development: The limits of the possible. Dev Psychopathol. 2003;15:613-640.
199 Brown RT. Society of pediatric psychology presidential address: Toward a social ecology of pediatric psychology. J Pediatr Psychol. 2002;27:191-201.
* All authors after the first are listed in alphabetical order by last name; the contributions of these authors were similar. Completion of this manuscript was supported by research grants from the National Institute of Child Health and Human Development (R01-HD048629) and the March of Dimes Birth Defects Foundation (12-FY04-47). All correspondence should be sent to: Grayson N. Holmbeck, Loyola University at Chicago, Department of Psychology, 6525 N. Sheridan Road, Chicago, IL 60626 (gholmbe@luc.edu)