Chapter 673 The Upper Limb
Elbow
Panner’s Disease
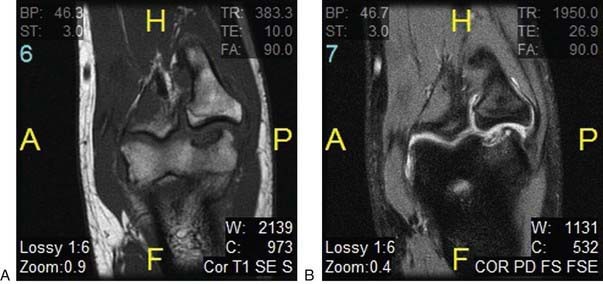
Panner’s disease is a disruption of the blood flow to the articular cartilage and subchondral bone to the capitellum (Fig. 673-1). It typically occurs in boys between the ages of 5 and 13 yr. Presenting symptoms include lateral elbow pain, loss of motion, and, in advanced cases, mechanical symptoms of the elbow.
Radial Longitudinal Deficiency
Radial longitudinal deficiency of the forearm comprises a spectrum of conditions and diseases that have resulted in hypoplasia or absence of the radius (Table 673-1). This process was formerly referred to as radial club hand, but the name has been changed to radial longitudinal deficiency, which better characterizes the condition. Clinical characteristics consist of a small, shortened limb with the hand and wrist in excessive radial deviation.
Table 673-1 SYNDROMES COMMONLY ASSOCIATED WITH RADIAL DEFICIENCY
| SYNDROME | CHARACTERISTICS |
|---|---|
| Holt-Oram syndomre | Heart defects, most commonly atrial septal defects |
| Thrombocytopenia absent radius | Thrombocytopenia present at birth but improves over time |
| VACTERL association | Vertebral abnormalities, anal atresia, cardiac abnormalities, tracheoesophageal fistula, esophageal atresia, renal defects, radial dysplasia, lower limb abnormalities |
| Fanconi anemia | Aplastic anemia not present at birth, develops about 6 yr of age; fatal without bone marrow transplant; chromosomal breakage challenge test available for early diagnosis |
From Trumble T, Budoff J, Cornwall R, editors: Core knowledge in orthopedics: hand, elbow, shoulder, Philadelphia, 2005, Elsevier, p 425.
Radial longitudinal deficiency can range in severity from mild to severe and has been classified into four types according to Bayne and Klug (Table 673-2). Radial longitudinal deficiency can be associated with other syndromes such as Holt-Oram and Fanconi’s anemia.
Table 673-2 CLASSIFICATION OF RADIAL LONGITUDINAL DEFICIENCY
| TYPE | CHARACTERISTICS |
|---|---|
| I | Short radius Minor radial deviation of the hand |
| II | Hypoplastic radius with abnormal growth at proximal and distal ends Moderate radial deviation of the hand |
| III | Partial absence of the radius Severe radial deviation of the hand |
| IV | Complete absence of the radius The most common type |
Adapted from Bayne LG, Klug MS: Long-term review of the surgical treatment of radial deficiencies, J Hand Surg Am 12(2):169–179, 1987.
Nursemaid Elbow
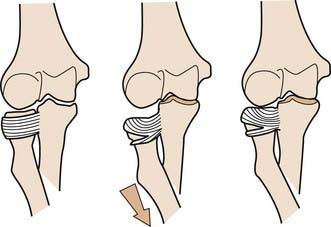
Nursemaid elbow is a subluxation of a ligament rather than a subluxation or dislocation of the radial head. The proximal end of the radius, or radial head, is anchored to the proximal ulna by the annular ligament, which wraps like a leash from the ulna, around the radial head, and back to the ulna. If the radius is pulled distally, the annular ligament can slip proximally off the radial head and into the joint between the radial head and the humerus (Fig. 673-2). The injury is typically produced when a longitudinal traction force is applied to the arm, such as when a falling child is caught by the hand, or when a child is pulled by the hand. The injury usually occurs in toddlers and rarely occurs in children >5 yr of age. Subluxation of the annular ligament produces immediate pain and limitation of supination. Flexion and extension of the elbow are not limited, and swelling is generally absent. The diagnosis is made by history and physical examination, as radiographs are typically normal.
Hand
Camptodactyly
Camptodactyly is a nontraumatic flexion contracture of the proximal interphalangeal joint that is often progressive. The small and ring fingers are most often affected. Bilateralism is observed two thirds of the time. The etiology of camptodactyly is varied. Several different hypotheses have been offered as to the cause of this condition. Camptodactyly can be divided into three different types (Table 673-3).
| TYPE | CHARACTERISTICS |
|---|---|
| I | Congenital no sex bias, small finger only |
| II | Acquired between 7-11 yr, typically progressive |
| III | Severe, significant contracture, bilateral and associated with other musculoskeletal syndromes |
Adapted from Kozin SH: Pediatric hand surgery. In Beredjiklian PK, Bozentka DJ, editors: Review of hand surgery, Philadelphia, 2004, WB Saunders, pp 223–245.
Clinodactyly
Angular deformity of the digit in the coronal plane, distal to the metacarpophalangeal joint is clinodactyly. The most commonly observed finding is a mild radial deviation of the small finger at the level of the distal interphalangeal joint. This is often due to a triangular or trapezoidal middle phalanx. In some cases, a disruption of the physis at the middle phalanx produces a longitudinal epiphysial bracket. This bracket is thought to be the underlying cause for the formation the “delta phalanx” that is often observed in clinodactyly. Clinodactyly has been observed in other fingers, including the thumb (Fig. 673-3) and ring finger.

Polydactyly
Polydactyly or duplication of a digit can occur either as a preaxial deformity (involving the thumb) or as a post axial deformity (involving the small finger) (Table 673-4). Each has an inherited and genetic component. Duplication of the thumb occurs more in white children and is often unilateral, whereas duplication of the small finger occurs mainly in African-Americans and may be bilateral. Transmission is typically in an autosomal dominant pattern and has been linked to defects in genes localized to chromosome 2.
Duplication of the thumb was extensively studied by Wassel. Wassel subdivided thumb duplication on the basis of the degree of duplication. The seven types according to Wassel are listed in Table 673-5. Small finger duplication has been further subdivided into two types. Type A is a well-formed digit. Type B is a small, often underdeveloped supernumerary digit.
| TYPE | CHARACTERISTICS |
|---|---|
| I | Bifid distal phalanx |
| II | Duplicate distal phalanx |
| III | Bifid proximal phalanx |
| IV | Duplicate proximal phalanx |
| V | Bifid metacarpal |
| VI | Duplicate metacarpal |
| VII | Triphalangeal component |
Adapted from Wassel, HD: The results of surgery for polydactyly of the thumb. A review, Clin Orthop 125:175–193, 1969.
Thumb Hypoplasia
Hypoplasia of the thumb is a challenging condition for both the patient and the doctor. The thumb represents ∼40% of hand function. A less-than-optimal thumb can severely limit a patient’s function as he or she grows and develops. Hypoplasia of the thumb can range from being mild with slight shortening and underdeveloped musculature to complete absence of the thumb (Fig. 673-4). Radiographs are useful to help determine osseous abnormalities. The most important finding on physical exam is the presence or absence of a stable carpometacarpal (CMC) joint. This finding helps guide surgical treatment.

Treatment
If a stable CMC joint is not present or the thumb is completely absent, pollicization (surgical construction of a thumb from a finger) is the definitive treatment. Pollicization is a complex procedure rotating the index finger along its neurovascular pedicle to form a thumb. This procedure is typically performed at around 1 yr of age and may be followed by subsequent procedures to deepen the web space or augment abduction (Fig. 673-5).

Syndactyly
Failure of the individual digits to separate during development produces syndactyly. Syndactyly is one of the more common anomalies observed in the upper limb (Table 673-6). It is seen in 0.5 of 1,000 live births. Syndactyly can be classified as simple (skin attachments only), complicated (bone and tendon attachments), complete (fusion to the tips, including the nail), or incomplete (simple webbing).
Ali M, Jackson T, Rayan GM. Closing wedge osteotomy of abnormal middle phalanx for clinodactyly. Hand Surg Am. 2009;34(5):914-918.
Altergott C, Garcia FJ, Nager AL. Pediatric fingertip injuries. Pediatr Emerg Med. 2008;24:148-152.
Kenniston JA, Beredjiklian PK, Bozentka DJ. Osteochondritis dissecans of the capitellum in fraternal twins: case report. J Hand Surg Am. 2008;33:1380-1383.
Lahiri A, Lester R. Hand anomalies in Russell Silver syndrome. J Plast Reconstr Aesthet Surg. 2009;62(4):462-465.
Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009;25(2):157-170.
Pill SG, Ganley TJ, Flynn JM, et al. Osteochondritis dissecans of the capitellum: arthroscopic-assisted treatment of large, full-thickness defects in young patients. Arthroscopy. 2003;19(2):222-225.
Ty JM, James MA. Failure of differentiation: part II (arthrogryposis, camptodactyly, clinodactyly, madelung deformity, trigger finger, and trigger thumb). Hand Clin. 2009;25(2):195-213.
Wafa AM. Hourglass dorsal metacarpal island flap: a new design for syndactylized web reconstruction. J Hand Surg Am. 2008;33(6):905-908.
Zebala LP, Manske PR, Goldfarb CA. Madelung’s deformity: a spectrum of presentation. J Hand Surg Am. 2007;32(9):1393-1401.





