[level-membership-for-orthopaedics-category]
Chapter 10 The Relative Strengths of Anterior Cruciate Ligament Autografts and Allografts
Methods
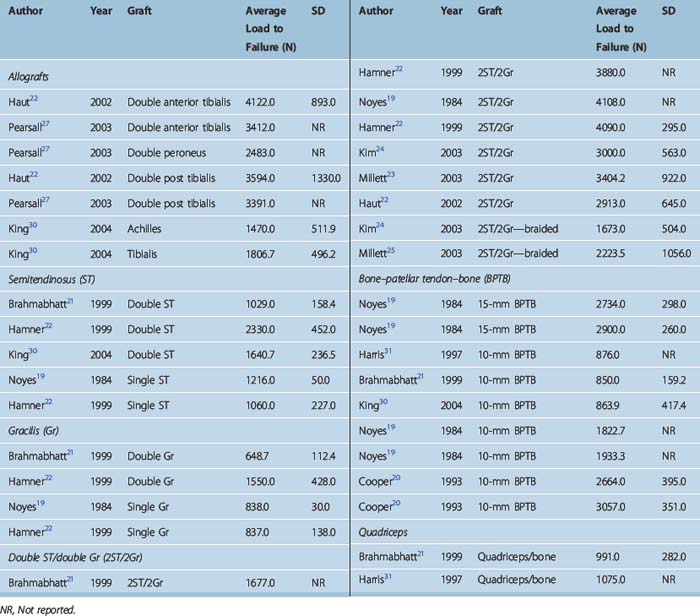
Table 10–1 summarizes the data that we were able to find in the literature on graft strengths. Load to failure (LTF) is the parameter compared in each case. This data was found from computerized literature searches targeting ACL reconstruction and each of the specific grafts in clinical use. Although some tissue banks have performed their own studies on graft strengths, we have purposely excluded such proprietary data and relied only on data published in the peer-reviewed literature to avoid bias.
Comparison of Graft Strengths
There is significant variability in LTF results among different studies for the same graft (see Table 10–1). This is likely related to differences in testing methodologies. Thus, it is necessary to look at the totality of the data to get an overall idea of relative graft strengths. Some of the authors have what appears to be outlier LTFs, but the relative strengths between grafts within their study generally reflect the bulk of the literature. The two main examples here are the data of Brahmabhatt21 and Harris, with low LTFs for all grafts tested relative to other studies. When comparing grafts it is important also to notice the configuration of the tested grafts; in other words, whether it is a single, double, or quadruple graft, and in the case of bone–patellar tendon–bone (BPTB), whether it is a 10-mm or 15-mm graft. The data in Table 10–1 also show that braiding of grafts has been shown to weaken rather than strengthen grafts and is not clinically indicated.
Effect of Ligamentization
Chapter 55 describes the effects of ligamentization on graft strength. Although there is some disagreement, it appears that grafts retain only about half their initial strength at long-term follow-up. Thus, grafts that are significantly stronger than the native ACL at time zero may indeed be necessary to produce ultimate strengths that are as strong as the ACL initially was. Indeed, some studies report a lower re-rupture rate for reconstructed ACLs than for the contralateral normal ACL,1 perhaps due to greater graft strength.
Allograft Strengths
Autograft strengths are relatively straightforward to measure. However, allograft strengths are more complicated because of the varying effects of graft preparation and sterilization techniques on the graft. Thus, any study that measures allograft strength can only be considered accurate for an allograft prepared in a similar manner. The relevant parameters may include radiated versus not radiated, the amount of radiation, and whether or not a radioprotectant was used. Other processes shown to significantly affect tissue properties include the use of cryoprotectant2 and even simple freezing.3 This is further complicated by the fact that these parameters may affect allograft strength at longer-term follow-up by influencing revascularization and cellular repopulation in addition to their effects at time zero. Thus, time zero data may not be sufficient for comparison between autografts and allografts, particularly in light of evidence that late failure rates may be higher for allografts than for autografts.4–7 The literature has also shown overall lower stability rates for allograft BPTB versus autograft BPTB,8–17 suggesting that ligamentization may weaken allografts more than autografts.18
Relative Strength of Hamstring and Bone–patellar tendon–bone Grafts
The classic paper of Noyes et al19 first compared various tissues with the ACL from the same cadaveric specimen. Other works have followed a similar methodology. These studies are summarized in Table 10–1. It should be noted that the study by Noyes et al used a 15-mm BPTB graft, whereas in practice a roughly 10-mm graft is used. Extrapolating from their numbers, a 10-mm BPTB graft would be 110% as strong as the native ACL. A two-strand semitendinosus (ST) and two-strand gracilis (Gr) (2ST/2Gr) graft would be 238% as strong as the native ACL. A four-strand ST (4ST) would be 280% as strong as the ACL. The real values for these multistrand grafts are probably a little less than these extrapolations because it is unlikely that the entire tendon is as strong as these index values. Some more recent studies have produced very different absolute numbers, perhaps related to testing methodological differences.20–29 However, within studies the relative strengths of various grafts show general agreement.
Conclusions
1 Prodromos CC, Han YS, Keller BL, et al. Stability of hamstring anterior cruciate ligament reconstruction at two- to eight-year follow-up. Arthroscopy. 2005;21:138-146.
2 Caborn D, Nyland J, Chang HC, et al. Tendon allograft cryoprotectant incubation and rehydration time alters mechanical stiffness properties. Presented at the 2006 meeting of the European Society of Sports Traumatology, Knee Surgery, and Arthroscopy, Innsbruck, Australia. May 2006.
3 Clavert P, Kempf JF, Bonnomet F, et al. Effects of freezing/thawing on the biomechanical properties of human tendons. Surg Radiol Anat. 2001;23:259-262.
4 Prodromos CC, Fu F, Howell S, et al. Controversies in soft tissue anterior cruciate ligament reconstruction. Presented at the 2006 Symposium of the American Academy of Orthopaedic Surgeons. Chicago: AAOS Symposium; Controversies in Soft Tissue ACL Reconstruction; May, 2006.
5 Scheffler S, Unterhauser F, Keil J, et al. Comparison of tendon-to-bone healing after soft tissue autograft and allograft ACL reconstruction in a sheep model. Presented at the 2006 meeting of the European Society of Sports Traumatology, Knee Surgery, and Arthroscopy, Innsbruck, Australia. May, 2006.
6 Siegel MG. Personal communication. Meeting of the Arthroscopy Association of North America, Hollywood, Florida. May, 2006.
7 Risinger RJ, Bach BRJr. Late anterior cruciate ligament reconstruction failure by femoral bone plug dislodgement. J Knee Surg. 2006;19:202-205.
8 Barrett G, Stokes D, White M. Anterior cruciate ligament reconstruction in patients older than 40 years: allograft versus autograft patellar tendon. Am J Sports Med. 2005;33:1505-1512.
9 Gorschewsky O, Klakow A, Riechert K, et al. Clinical comparison of the Tutoplast allograft and autologous patellar tendon (bone–patellar tendon–bone) for the reconstruction of the anterior cruciate ligament: 2- and 6-year results. Am J Sports Med. 2005;33:1202-1209.
10 Harner CD, Olson E, Irrgang JJ, et al. Allograft versus autograft anterior cruciate ligament reconstruction: 3- to 5-year outcome. Clin Orthop Rel Rsch. 1996;324:134-144.
11 Kleipool AEB, Zijl JAC, Willems WJ. Arthroscopic anterior cruciate ligament reconstruction with bone-patellar tendon-bone allograft or autograft: a prospective study with an average follow up of 4 years. Knee Surg Sports Traumatol Arthrosc. 1998;6:224-230.
12 Peterson RK, Shelton WR, Bomboy AL. Allograft versus autograft patellar tendon anterior cruciate ligament reconstruction: a 5-year follow-up. Arthroscopy. 2001;17:9-13.
13 Shelton WR, Papendick L, Dukes AD. Autograft versus allograft anterior cruciate ligament reconstruction. Arthroscopy. 1997;13:446-449.
14 Stringham DR, Pelmas CJ, Burks RT, et al. Comparison of anterior cruciate ligament reconstruction using patellar tendon autograft or allograft. Arthroscopy. 1996;12:414-421.
15 Victor J, Bellemans J, Witvrouw E, et al. Graft selection in anterior cruciate ligament reconstruction—prospective analysis of patellar tendon autografts compared with allografts. Int Orthop. 1997;21:93-97.
16 Zijl JAC, Kleipool AEB, Willems WJ. Comparison of tibial tunnel enlargement after anterior cruciate ligament reconstruction using patellar tendon autograft or allograft. Am J Sports Med. 2000;28:547-551.
17 Chang SKY, Egami DK, Shaib MD, et al. Anterior cruciate ligament reconstruction: allograft versus autograft. Arthroscopy. 2003;19:453-462.
18 Prodromos CC, Joyce BT, Shi KS. A meta-analysis of stability of autografts compared to allografts after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc (In press)
19 Noyes FR, Butler DL, Grood ES, et al. Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am. 1984;66A:344-352.
20 Brahmabhatt V, Smolinski R, McGlowan J, et al. Double-stranded hamstring tendons for anterior cruciate ligament reconstruction. Am J Knee Surg. 1999;12:141-145.
21 Cooper DE, Deng XH, Burstein AL, et al. The strength of the central third patellar tendon graft. Am J Sports Med. 1993;21:818-824.
22 Haut Donahue TL, Howell SM, Hull ML, et al. A biomechanical evaluation of anterior and posterior tibialis tendons as suitable single-loop anterior cruciate ligament grafts. Arthroscopy. 2002;18:589-597.
23 Hamner DL, Brown CHJr, Steiner ME, et al. Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am. 1999;81A:549-557.
24 Kim DH, Wilson DR, Hecker AT, et al. Twisting and braiding reduces the tensile strength and stiffness of human hamstring tendon grafts used for anterior cruciate ligament reconstruction. Am J Sports Med. 2003;31:861-867.
25 Millett PJ, Miller BS, Close M, et al. Effects of braiding on tensile properties of four-strand human hamstring tendon grafts. Am J Sports Med. 2003;31:714-717.
26 Nicklin S, Waller C, Walker P, et al. In vitro structural properties of braided tendon grafts. Am J Sports Med. 2000;28:790-793.
27 Pearsall AW, Hollis JM, Russel GV, et al. A biomechanical comparison of three lower extremity tendons for ligamentous reconstruction about the knee. Arthroscopy. 2003;19:1091-1096.
28 Stapleton TR, Curd DT, Baker CLJr. Initial biomechanical properties of anterior cruciate ligament reconstruction autografts. J South Orthop Assoc. 1999;8:173-180.
29 Tis JE, Klemme WR, Kirk KL, et al. Braided hamstring tendons for reconstruction of the anterior cruciate ligament. Am J Sports Med. 2002;30:684-688.
30 King W, Mangan D, Endean T, et al. Microbial sterilization and viral inactivation in soft tissue allografts using novel applications of high-dose gamma irradiation. Presented at the American Academy of Orthopaedic Surgeons, San Francisco, CA. March 2004.
31 Harris NL, Smith DA, Lamoreaux L, Purnell M. Central quadriceps tendon for anterior cruciate ligament reconstruction. Part I: Morphometric and biomechanical evaluation. Am J Sports Med. 1997;5:725-727.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
Chapter 10 The Relative Strengths of Anterior Cruciate Ligament Autografts and Allografts
Methods
Table 10–1 summarizes the data that we were able to find in the literature on graft strengths. Load to failure (LTF) is the parameter compared in each case. This data was found from computerized literature searches targeting ACL reconstruction and each of the specific grafts in clinical use. Although some tissue banks have performed their own studies on graft strengths, we have purposely excluded such proprietary data and relied only on data published in the peer-reviewed literature to avoid bias.
Comparison of Graft Strengths
There is significant variability in LTF results among different studies for the same graft (see Table 10–1). This is likely related to differences in testing methodologies. Thus, it is necessary to look at the totality of the data to get an overall idea of relative graft strengths. Some of the authors have what appears to be outlier LTFs, but the relative strengths between grafts within their study generally reflect the bulk of the literature. The two main examples here are the data of Brahmabhatt21 and Harris, with low LTFs for all grafts tested relative to other studies. When comparing grafts it is important also to notice the configuration of the tested grafts; in other words, whether it is a single, double, or quadruple graft, and in the case of bone–patellar tendon–bone (BPTB), whether it is a 10-mm or 15-mm graft. The data in Table 10–1 also show that braiding of grafts has been shown to weaken rather than strengthen grafts and is not clinically indicated.
Effect of Ligamentization
Chapter 55 describes the effects of ligamentization on graft strength. Although there is some disagreement, it appears that grafts retain only about half their initial strength at long-term follow-up. Thus, grafts that are significantly stronger than the native ACL at time zero may indeed be necessary to produce ultimate strengths that are as strong as the ACL initially was. Indeed, some studies report a lower re-rupture rate for reconstructed ACLs than for the contralateral normal ACL,1 perhaps due to greater graft strength.
Allograft Strengths
Autograft strengths are relatively straightforward to measure. However, allograft strengths are more complicated because of the varying effects of graft preparation and sterilization techniques on the graft. Thus, any study that measures allograft strength can only be considered accurate for an allograft prepared in a similar manner. The relevant parameters may include radiated versus not radiated, the amount of radiation, and whether or not a radioprotectant was used. Other processes shown to significantly affect tissue properties include the use of cryoprotectant2 and even simple freezing.3 This is further complicated by the fact that these parameters may affect allograft strength at longer-term follow-up by influencing revascularization and cellular repopulation in addition to their effects at time zero. Thus, time zero data may not be sufficient for comparison between autografts and allografts, particularly in light of evidence that late failure rates may be higher for allografts than for autografts.4–7 The literature has also shown overall lower stability rates for allograft BPTB versus autograft BPTB,8–17 suggesting that ligamentization may weaken allografts more than autografts.18
