Chapter 7 The Neck
A. Neck Features And Swellings
(1) Generalities
The neck is an important crossroad of anatomic structures and organ systems, the most important of which is the thyroid (discussed in Chapter 8).



7 What are the anterior and posterior triangles of the neck?
They are important regions of the lateral neck, separated from each other by the sternocleidomastoid muscles (SCMs) (Fig. 7-1). These can be easily located through inspection and palpation, especially if tensed against resistance. The remaining borders of the posterior triangle are the anterior margin of the trapezius and the upper margin of the clavicle, whereas the remaining borders of the anterior triangle are the mandible and midline.
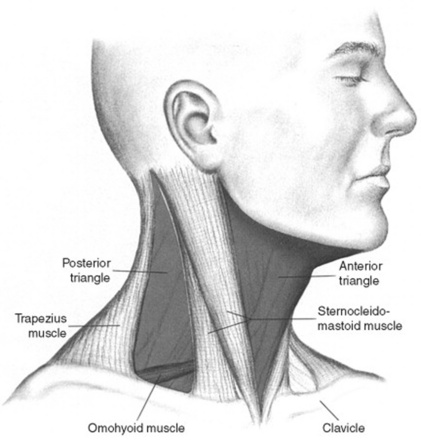
8 What are the contents of the cervical triangles?
 In the anterior triangle, one can often palpate the jugulodigastric node. Other nodes are instead undetectable, unless enlarged by infection, inflammation, or malignancy. The anterior triangles also may harbor important embryologic remnants, such as thyroglossal duct/cysts, branchial cysts, and dermoids.
In the anterior triangle, one can often palpate the jugulodigastric node. Other nodes are instead undetectable, unless enlarged by infection, inflammation, or malignancy. The anterior triangles also may harbor important embryologic remnants, such as thyroglossal duct/cysts, branchial cysts, and dermoids.

 The subclavian artery may be felt pulsating at the base of the neck, just above the clavicle.
The subclavian artery may be felt pulsating at the base of the neck, just above the clavicle.


9 Which swellings may be encountered during inspection of the neck?
Many. Classification and origin depend on location (posterior or anterior triangle; and for the latter, midline or lateral aspect) and nature (inflammatory or neoplastic) (Table 7-1).
| Anterior triangle |
| Midline |
 Mostly thyroidal—goiter/nodule(s) Mostly thyroidal—goiter/nodule(s) |
 Thyroglossal (duct) cyst Thyroglossal (duct) cyst |
 Thyroglossal fistula Thyroglossal fistula |
 Dermoid (cyst) Dermoid (cyst) |
| Lateral aspect |
 Branchial cleft cyst Branchial cleft cyst |
 Branchial fistula Branchial fistula |
 Branchial hygroma Branchial hygroma |
 Cystic hygroma Cystic hygroma |
 Laryngocele Laryngocele |
 Masseter muscle hypertrophy Masseter muscle hypertrophy |
| Posterior triangle |
| Neoplastic |
 Lymphomas Lymphomas |
 Metastatic Metastatic |
 Neurogenic Neurogenic |
 Paragangliomas/glomus tumors Paragangliomas/glomus tumors |
 Miscellaneous (ectopic salivary) Miscellaneous (ectopic salivary) |
| Inflammatory: localized |
 Tuberculous lymphadenitis (scrofula) Tuberculous lymphadenitis (scrofula) |
 Bacterial lymphadenitis (abscess) Bacterial lymphadenitis (abscess) |
 Suppurated branchial or thyroglossal cyst Suppurated branchial or thyroglossal cyst |
| Inflammatory: diffuse |
 Ludwig’s angina Ludwig’s angina |
(2) Swellings of the Anterior Triangle (Midline)
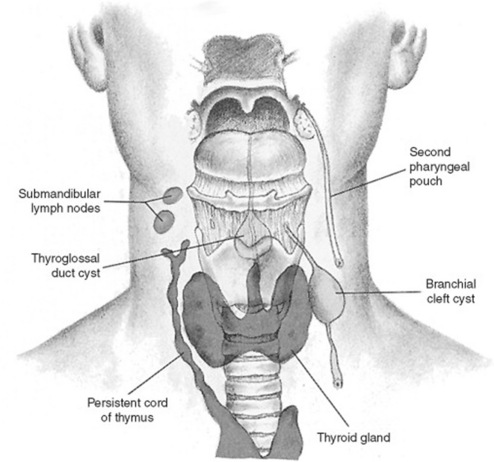
10 What is the origin of midline swellings of the anterior cervical triangle?
They are mostly thyroidal (goiters or nodules). Less commonly, they represent remnants of embryonic structures, such as dermoids or thyroglossal duct cysts (Fig. 7-2). Since only thyroid and laryngeal structures ascend with deglutition, nonthyroidal masses can be easily identified by asking the patient to swallow.
12 Do thyroglossal cysts transilluminate?
No—which is counterintuitive, considering their cystic nature.
13 How common is a thyroglossal cyst?
Quite common. In fact, of all congenital neck masses, 75% are thyroglossal duct cysts.
14 What accounts for the other 25% of congenital neck masses?
Branchial cleft cysts, typically located more laterally, just between the SCM and hyoid.
21 Is adenopathy common in branchial cysts?
No. If present, consider either tuberculous adenitis (scrofula) or a complicating abscess.
28 How does congenital hypertrophy of the masseter present?
Like a parotid mass. Differentiation can be easily accomplished by palpation.
31 What are the most common neoplastic swellings?





39 How does Ludwig’s angina spread?
 The submandibular space. This is the primary site of infection in Ludwig’s. It is subdivided into two spaces that communicate posteriorly: (1) the sublingual space, which is bound superiorly by the mouth floor, posteriorly by the tongue base, anterolaterally by the mandible, and inferiorly by the mylohyoid muscle; and (2) the submaxillary space, which is bound superiorly by the mandibular ramus and inferiorly by both the hyoid and the posterior belly of the digastric muscle. Note that the anterior and lateral borders of the entire submandibular space are formed by the outer investing fascia’s attachments to the mandible.
The submandibular space. This is the primary site of infection in Ludwig’s. It is subdivided into two spaces that communicate posteriorly: (1) the sublingual space, which is bound superiorly by the mouth floor, posteriorly by the tongue base, anterolaterally by the mandible, and inferiorly by the mylohyoid muscle; and (2) the submaxillary space, which is bound superiorly by the mandibular ramus and inferiorly by both the hyoid and the posterior belly of the digastric muscle. Note that the anterior and lateral borders of the entire submandibular space are formed by the outer investing fascia’s attachments to the mandible.







B. Salivary Glands
47 Where are the sublingual glands?
In the mouth floor, just under the tongue. They are palpable but not routinely assessed.
49 What are the causes of salivary gland swelling?
Bilateral swelling carries a much wider differential diagnosis:










C. Trachea
1 Allard RHB. The thyroglossal cyst. Head Neck Surg. 1982;5:134-146.
2 Bailey H. Thyroglossal cysts and fistulae. Br J Surg. 1925;12:579-589.
3 Bounds GA. Subphrenic and mediastinal abscess formation: A complication of Ludwig’s angina. Br J Oral Maxillofac Surg. 1985;23:313-321.
4 Ellis P, Van Nostrand AW. The applied anatomy of thyroglossal tract remnants. Laryngoscope. 1977;87:765-770.
5 Ewing CA, Kornblut A, Greeley C, et al. Presentations of thyroglossal duct cysts in adults. Eur Arch Otorh. 1999;256:136-138.
6 Girard M, Deluca SA. Thyroglossal duct cyst. Am Fam Physician. 1990;42:665-668.
7 Guarisco JL. Congenital head and neck masses in infants and children. Ear Nose Throat J. 1991;70:40-47.
8 Hawkins DB, Jacobsen BE, Klatt EC. Cysts of the thyroglossal duct. Laryngoscope. 1982;92:1254-1258.
9 Himalstein MR. Branchial cysts and fistulas. ENT. 1980;159:2329.
10 Juang YC, Cheng DL, Wang LS, et al. Ludwig’s angina: An analysis of 14 cases. Scand J Infect Dis. 1989;21:121-125.


