[level-membership-for-internal-medicine-category]
Chapter 3 The Skin
Basic Terminology and Diagnostic Techniques
1 How many skin diseases exist? What are the two main categories of skin lesions?
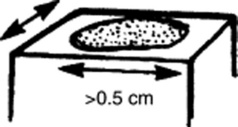
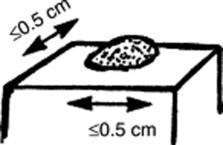
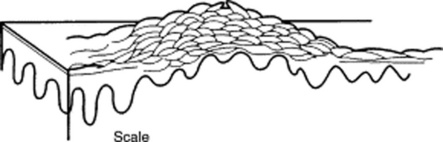
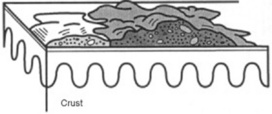
There are more than 1400 skin diseases. Yet, only 30 are important, common, and worth knowing. The first step toward their recognition is the separation of primary from secondary lesions (Table 3-1).
 Primary lesions result only from disease and have not been changed by additional events (such as trauma, scratching, or medical treatment; see Table 3-1). To better identify primary lesions, pay attention to their colors, shape, arrangement, and distribution.
Primary lesions result only from disease and have not been changed by additional events (such as trauma, scratching, or medical treatment; see Table 3-1). To better identify primary lesions, pay attention to their colors, shape, arrangement, and distribution.

| skin lesions | ||
|---|---|---|
| Primary | Secondary | Special |
| Solid (Nonpalpable) | Crusts | Purpurae |
| • Macules (≤0.5 cm) | Scales | Petechiae |
| • Patches (>0.5 cm) | Ulcers | Ecchymoses |
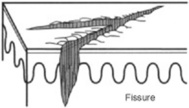
| Fissures | Teleangiectasias | |
| Solid (Palpable) | Excorations | Comedones |
| • Papules (≤0.5 cm) | Scars | Burrows |
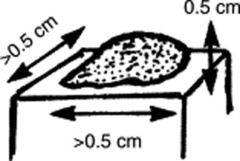
| • Plaques (>0.5 cm) | Erosions | Target lesions |
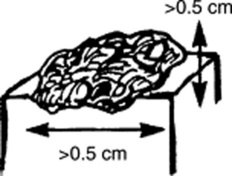
| • Nodules (deeper plaques) | Lichenification | |
| • Wheals (pruritic plaques) | Atrophy | |
| • Tumors (larger nodules) | Scars | |
| Sinuses | ||
| Fluid-Lesions | ||
| • Vesicles (fluid-filled papules) | ||
| • Pustules (pus-filled papules) | ||
| • Bullae (fluid-filled plaques) | ||
| • Cysts (fluid-filled nodules) | ||
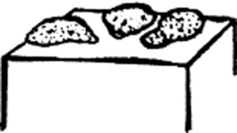
2 What are the major primary lesions?
 Macules: Flat, nonpalpable, circumscribed areas of discoloration ≤0.5 cm in diameter. Typical macules are the familiar freckles.
Macules: Flat, nonpalpable, circumscribed areas of discoloration ≤0.5 cm in diameter. Typical macules are the familiar freckles.




 Tumors: Nodules that are either >2 cm in diameter or poorly demarcated. Usually neoplastic.
Tumors: Nodules that are either >2 cm in diameter or poorly demarcated. Usually neoplastic.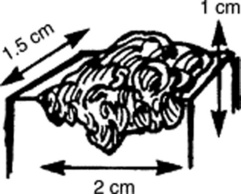







 Pustules: Pus-filled papules. Typically seen in patients with impetigo or acne.
Pustules: Pus-filled papules. Typically seen in patients with impetigo or acne.









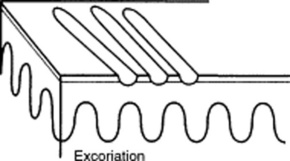
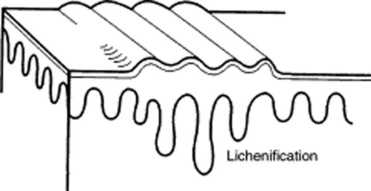
3 What are the major secondary lesions?
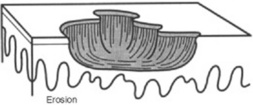
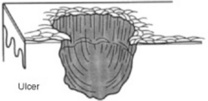
 Excoriations: Linear erosions produced by scratching. Often raised, scratch marks may also present as crust on top of a primary lesion that has been partially scratched off. They are almost exclusively confined to the eczematous diseases.
Excoriations: Linear erosions produced by scratching. Often raised, scratch marks may also present as crust on top of a primary lesion that has been partially scratched off. They are almost exclusively confined to the eczematous diseases.







 Sinuses: Connective channels between the surface of the skin and deeper components.
Sinuses: Connective channels between the surface of the skin and deeper components.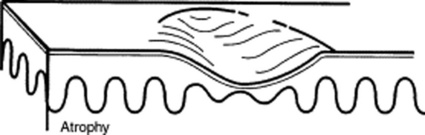
4 Are there other ways to classify skin lesions?
Many ways. One divides lesions into four groups based on the relationship with the surrounding skin:







6 What is the configuration of a skin lesion?
It is the outline of the lesion as observed from above. The most common configurations are:




9 And so, what are the required components of a dermatologic diagnosis?
 Morphology: Color, shape, dimensions (width and height, if necessary), elevation/depression, and palpable features (smoothness, induration, tenderness, scaling, and crusting)
Morphology: Color, shape, dimensions (width and height, if necessary), elevation/depression, and palpable features (smoothness, induration, tenderness, scaling, and crusting)
 Distribution (body location): Generalized versus localized
Distribution (body location): Generalized versus localized
 Distribution (arrangement to one another): Clustered, confluent, dermatomal
Distribution (arrangement to one another): Clustered, confluent, dermatomal




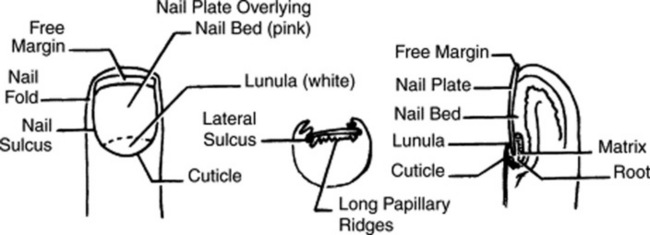
14 How should fingernails and toenails be assessed?
If covered by polish, clean them first with a solvent like acetone. Then pay attention to color and shape but also to anatomic details (Fig. 3-25):



15 What systemic conditions are associated with changes in nail shape or growth?
 Clubbing: Inflammatory bowel disease, pulmonary malignancy, asbestosis, chronic bronchitis, chronic obstructive pulmonary disease, cirrhosis, congenital heart disease, endocarditis, atrioventricular malformation and fistulas (see also question 19)
Clubbing: Inflammatory bowel disease, pulmonary malignancy, asbestosis, chronic bronchitis, chronic obstructive pulmonary disease, cirrhosis, congenital heart disease, endocarditis, atrioventricular malformation and fistulas (see also question 19)
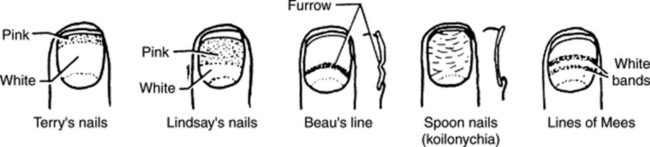
 Koilonychia (spoon nails) (Fig. 3-26): Iron deficiency anemia, hemochromatosis, Raynaud’s disease, systemic lupus disease, trauma, nail-patella syndrome
Koilonychia (spoon nails) (Fig. 3-26): Iron deficiency anemia, hemochromatosis, Raynaud’s disease, systemic lupus disease, trauma, nail-patella syndrome

 Pitting: Psoriasis, Reiter’s syndrome, incontinentia pigmenti, alopecia areata
Pitting: Psoriasis, Reiter’s syndrome, incontinentia pigmenti, alopecia areata
 Beau’s lines (see Fig. 3-26): Any severe systemic illness that disrupts nail growth, Raynaud’s disease, pemphigus, trauma
Beau’s lines (see Fig. 3-26): Any severe systemic illness that disrupts nail growth, Raynaud’s disease, pemphigus, trauma

16 What systemic conditions are associated with changes in nail color?
 Terry’s nails (see Fig. 3-26): Hepatic failure, cirrhosis, diabetes, congestive heart failure, hyperthyroidism, malnutrition
Terry’s nails (see Fig. 3-26): Hepatic failure, cirrhosis, diabetes, congestive heart failure, hyperthyroidism, malnutrition
 Azure lunula: Wilson’s disease, silver poisoning, quinacrine
Azure lunula: Wilson’s disease, silver poisoning, quinacrine
 Lindsay’s nails (half-and-half nails) (see Fig. 3-26): Specific for renal failure
Lindsay’s nails (half-and-half nails) (see Fig. 3-26): Specific for renal failure
 Muehrcke’s lines: Specific for hypoalbuminemia
Muehrcke’s lines: Specific for hypoalbuminemia
 Lines of Mees’ (see Fig. 3-26): Arsenic poisoning, Hodgkin’s disease, congestive heart failure, leprosy, malaria, chemotherapy, carbon monoxide poisoning, other systemic insults
Lines of Mees’ (see Fig. 3-26): Arsenic poisoning, Hodgkin’s disease, congestive heart failure, leprosy, malaria, chemotherapy, carbon monoxide poisoning, other systemic insults

 Longitudinal striations: Alopecia areata, vitiligo, atopic dermatitis, psoriasis
Longitudinal striations: Alopecia areata, vitiligo, atopic dermatitis, psoriasis

 Telangiectasia: Rheumatoid arthritis, systemic lupus erythematosus, dermatomyositis, scleroderma
Telangiectasia: Rheumatoid arthritis, systemic lupus erythematosus, dermatomyositis, scleroderma





Nails
19 What is clubbing?
A condition that can be (1) idiopathic; (2) congenital (dominant trait); or (3) a clue to serious underlying pathology, including cardiovascular, hepatobiliary, mediastinal, endocrine, gastrointestinal, neoplastic, infectious, and, especially, pulmonary (see Chapter 13, questions 101–116).
22 What are the nail findings of psoriasis?
 Pitting (previously discussed)
Pitting (previously discussed)

 Beau’s lines in the proximal nail matrix (see later)
Beau’s lines in the proximal nail matrix (see later)
 Leukonychia: Areas of white nail plate; due to parakeratotic foci in the mid-matrix
Leukonychia: Areas of white nail plate; due to parakeratotic foci in the mid-matrix
 Subungual hyperkeratosis: Excessive proliferation of the nail bed that can lead to onycholysis
Subungual hyperkeratosis: Excessive proliferation of the nail bed that can lead to onycholysis

 Nail plate crumbling: Weakened nail plate, bed, and matrix from diseased underlying structures
Nail plate crumbling: Weakened nail plate, bed, and matrix from diseased underlying structures

 Dilated tortuous capillaries in the dermal papillae
Dilated tortuous capillaries in the dermal papillae
 Spotted lunula: Distal matrix involvement characterized by erythema of the lunula
Spotted lunula: Distal matrix involvement characterized by erythema of the lunula
26 What is longitudinal ridging (Reedy nails)?
A normal variant of patients older than 50, but one that also can occur in younger subjects. It may even represent a brittle nail variation. Ridges typically extend from the proximal nail fold to the distal plate, with some being very prominent, especially in older women. They are usually multiple, but at times may be single—like in patients with lichen planus (see questions 38 and 210–216).
38 What is lichen planus of the nail?
A condition present in 10% of patients with lichen planus. The most common finding is thinning of the nail plate, leading to longitudinal grooving and ridging (see also question 26). Hyperpigmentation, subungual hyperkeratosis, onycholysis, and longitudinal melanonychia can also be present.
41 What are azure half-moons in nail beds?
The nails of Wilson’s disease (hepatolenticular degeneration). Lunulae are not white, but bluish.
48 What is paronychia?
An acute or chronic inflammation of the perionychium, with redness, swelling, and tenderness.
Fluid-Filled Lesions: PUS (Pustules)—Table 3-2
Acne
54 What does acne look like?
| Fluid-Filled Lesions | ||
|---|---|---|
| Pus-Filled | Clear Fluid | |
| Pustular | Vesiculo-Bullous | Bullous |
| Acne vulgaris | H. simplex | Pemphygus vulgaris |
| Acne rosacea | H. zoster/varicella | Pemphygoid |
| Steroid acne | Dermatophytoses | Drug reactions |
| • Erythema multiforme | ||
| • Stevens-Johnson | ||
| • TEN | ||
| Folliculitis (bacterial/fungal) | Insect bites | Poison ivy/contact dermatitis |
| Intertriginous candidiasis | Dermatitis herpetiformis | Bullous impetigo |
| Porphyria cutanea tarda | ||
| Lupus erythematosus | ||
Fluid-Filled Lesions: Clear Fluid (Vesiculobullous Diseases)
62 What is the typical clinical course of herpes simplex?


63 What are the other clinical presentations of herpes simplex?



66 Who develops varicella?
Mostly children younger than 10 years. Only 5% of cases occur in subjects older than 15.
73 What are the other presentations of herpes zoster?



79 Are there any other causes of PV?
A form of PV (but also BP, see question 80) can be drug induced, resulting from penicillamine, captopril, thiol-containing compounds, and rifampin. Emotional stress can also trigger it. Finally, PV may occur in other autoimmune diseases, including myasthenia gravis and thymoma.
82 What is Asboe-Hansen sign?
Another sign of PV; lateral pressure on the edge of a blister may spread it into unaffected skin.
84 What is erythema multiforme (EM)?
A relatively benign process characterized by target or targetoid lesions, with or without blisters, in a symmetric and acral distribution. In fact, the rash favors palms and soles, dorsum of hands, face, and extensor surfaces of extremities (Fig. 3-27). It is often associated with oral lesions, but rarely involves more than one mucosal surface. Although it can be caused by drugs, it is most commonly a sequela of herpes virus infection. It has low morbidity, no mortality, but frequent recurrences. It may be associated with epidermal detachment, yet denudation always involves <10% of BSA.

85 What is Stevens-Johnson syndrome (SJS)?
A potential dermatologic emergency. First described in 1922 by the American pediatricians Albert Stevens and Frank Johnson, SJS is characterized by widespread purpuric macules and targetoid lesions, usually more common on face and torso, and with concomitant mucosal involvement of more than one site (usually the eyes, mouth, and genitalia; Fig. 3-28). Lesions may undergo full-thickness epidermal necrosis, although this is limited by definition to <10% of cutaneous surface. Hence, mortality is much less than in TEN (only 5%).

86 What is toxic epidermal necrolysis (TEN)?
Also known as Lyell’s syndrome, this is a true dermatologic emergency characterized by widespread skin and mucosal denudation. Skin lesions are erythematous and target-like macules associated with full-thickness epidermal necrosis and detachment of >30% BSA (Fig. 3-29). It is fatal in 50% of the cases, usually because of sepsis and respiratory distress. Mortality is related to BSA involvement: 11% for BSA (which is actually more of a SJS-TEN transitional form), and 35% for BSA >30%.
91 What are the sequelae of SJS/TEN?














97 What are the most common photosensitizing medications?





101 What is the clinical course of urticaria?
 Acute urticaria resolves in 4–6 weeks. It is usually associated with drugs (penicillin, sulfonamides, aspirin); food allergens (e.g., chocolate, shellfish, eggs, cheese, nuts, peanut butter, berries, tomatoes, strawberries); new pets; or infections (upper respiratory infection, especially streptococcal in children). Pregnancy may aggravate it into pruritic and urticarial papules and plaques of pregnancy (PUPPP syndrome).
Acute urticaria resolves in 4–6 weeks. It is usually associated with drugs (penicillin, sulfonamides, aspirin); food allergens (e.g., chocolate, shellfish, eggs, cheese, nuts, peanut butter, berries, tomatoes, strawberries); new pets; or infections (upper respiratory infection, especially streptococcal in children). Pregnancy may aggravate it into pruritic and urticarial papules and plaques of pregnancy (PUPPP syndrome).

102 What are the other clinical presentations of urticaria?
1. Hereditary angioedema: Autosomal dominant, it presents in the second to fourth decade of life with sudden attacks of angioedema that often last for days and can be life threatening. Due to low or nonfunctional C1 inhibitor, with diagnosis being suggested by a low C4 level.
2. Physical urticarias: appear in response to a stimulus, such as cold, sunlight, trauma, water:






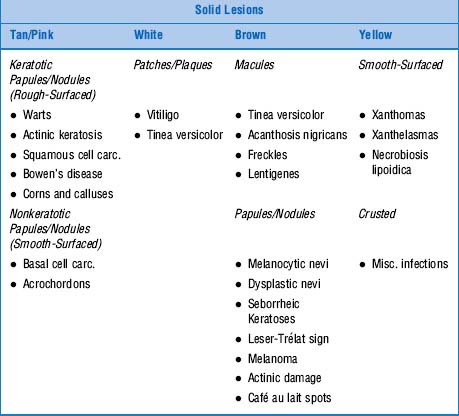
Solid Lesions: Tan Or Pink—Table 3-3
106 How are warts transmitted?
By direct or indirect contact, especially when the normal epithelial barrier has been disrupted.
107 What are the major types of warts?
 Common wart: Often referred to as verruca vulgaris, it presents as a rough-surfaced, scaly, and circumscribed papule, <1 mm to >0.5 cm in size. Most commonly located on hands and knees, although it can occur anywhere (Fig. 3-30). Often accompanied by “black seeds” (i.e., thrombosed capillaries). Usually asymptomatic, warts may cause cosmetic disfigurement or tenderness.
Common wart: Often referred to as verruca vulgaris, it presents as a rough-surfaced, scaly, and circumscribed papule, <1 mm to >0.5 cm in size. Most commonly located on hands and knees, although it can occur anywhere (Fig. 3-30). Often accompanied by “black seeds” (i.e., thrombosed capillaries). Usually asymptomatic, warts may cause cosmetic disfigurement or tenderness.
 Filiform wart: Long and slender growth, usually around lips, eyelids, or nares
Filiform wart: Long and slender growth, usually around lips, eyelids, or nares


 Flat wart: Also called “plane warts” (or verruca plana). Flat and flesh-colored papules, >1–5 mm in size. Smooth or slightly hyperkeratotic, they may number just a few or in the hundreds, at times becoming grouped or confluent, and often acquiring linear distribution after scratching or trauma (Koebner’s phenomenon). Although possible anywhere, they typically involve the face (Fig. 3-31), shins, and dorsum of hands. May regress spontaneously, often after an inflammatory flare.
Flat wart: Also called “plane warts” (or verruca plana). Flat and flesh-colored papules, >1–5 mm in size. Smooth or slightly hyperkeratotic, they may number just a few or in the hundreds, at times becoming grouped or confluent, and often acquiring linear distribution after scratching or trauma (Koebner’s phenomenon). Although possible anywhere, they typically involve the face (Fig. 3-31), shins, and dorsum of hands. May regress spontaneously, often after an inflammatory flare.


Squamous Cell Carcinoma (SCC)
109 How does SCC present?
In a myriad of morphologic variants, although typically as a scaly, erythematous, and hyperkeratotic plaque, often with superficial ulceration and no defined translucent border (Fig. 3-32).

110 Where in the skin does SCC originate?
From keratinocytes located in the epidermis, just above the basal layer.
117 What are the causes of skin tags?




Solid Lesions: White
120 How does vitiligo present?
As milky white, nonscaly, and sharply demarcated macules and patches of variable size (Fig. 3-33). These are often symmetric, and commonly involving areas of repeated trauma, such as elbows, ventral wrists, knees, axillae, dorsal hands, and feet. Other targets include mucous membranes and periorificial sites (eyes, nose, ears, lips, gums, genitals, areolas, and nipples). Lesions eventually increase in number and become confluent, taking on bizarre shapes. They may also appear at sites of injury (koebnerization). Localized vitiligo (i.e., restricted to one area) is less common.

121 What are the other associated cutaneous findings?
Prematurely gray hair, piebaldism (see question 122), halo nevi, alopecia areata, and ocular abnormalities, such as chorioretinitis, retinal pigmentary abnormalities, and iritis. The scalp is the hair most frequently involved, followed by eyebrows, pubis, and axillae. Vitiligo of the scalp usually presents as a localized patch of white or gray hair, but total scalp depigmentation (leukotrichia) may also occur, usually indicating low likelihood of repigmentation.
123 What are the characteristics of piebaldism?
Eighty to ninety percent of individuals have a white forelock, typically from birth. The central frontal scalp can also be permanently white, as may be eyebrow and eyelash hair. Finally, white spots may occur on the face, trunk, and extremities. Piebaldism is one of the cutaneous signs of Waardenburg’s syndrome, along with heterochromia of irides, lateral displacement of inner canthi, and deafness (see Chapter 4, questions 106 and 107).
126 What are the other clinical presentations of vitiligo?
 Segmental vitiligo: Characterized by unilateral depigmented macules and patches in a dermatomal or quasi-dermatomal distribution. It generally has a stable course.
Segmental vitiligo: Characterized by unilateral depigmented macules and patches in a dermatomal or quasi-dermatomal distribution. It generally has a stable course.
 Focal vitiligo: One or more pale macules in an area that is single but not segmental
Focal vitiligo: One or more pale macules in an area that is single but not segmental
 Universal vitiligo: It results in total or nearly total body involvement.
Universal vitiligo: It results in total or nearly total body involvement.
Solid Lesions: Brown
133 What are the causes of AN?




136 What about congenital nevi?
They are nevi that are present at birth or soon thereafter. They are probably hamartomas, since they contain many skin elements, but a predominance of melanocytes. Large congenital nevi have a low (5%) but real risk for malignant transformation into melanoma. Hence, the need for prophylactic excision. In a rare autosomal dominant condition, family members acquire with time many large nevi, sometimes more than 100 (see FAMMM, discussed in question 141).
137 List and describe the different types of common nevi (moles).



139 What are atypical or dysplastic nevi (Clark nevi)?
They are acquired variants typical of families of northern European descent, with fair skin, light-colored hair, freckles, and other Celtic features. The United Kingdom, Netherlands, Germany, and occasionally Poland and Russia are the most affected countries. Patients present with hundreds of relatively broad lesions that are flat or thinly papular. The more numerous the nevi, the greater the likelihood of melanoma (see discussion on familial atypical multiple mole and melanoma in question 141). Still, dysplastic nevi are just a marker for risk, and not necessarily a precursor. Hence, removal of all dysplastic nevi may not really alter the risk.
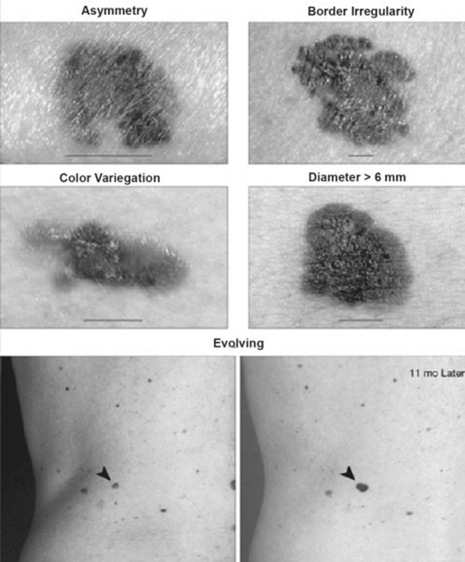
149 What is the ABCD(E) checklist?
A commonly used acronym for identifying the warning signs of malignant melanoma. Developed in 1985, it considers a lesion suspicious when it has more than one of the five following features (see Fig. 3-34):
 A = Asymmetry (if the lesion is bisected, one half is not identical to the other half)
A = Asymmetry (if the lesion is bisected, one half is not identical to the other half)
 B = Border irregularity (a border that is uneven or ragged as opposed to smooth and straight)
B = Border irregularity (a border that is uneven or ragged as opposed to smooth and straight)
 C = Color variegation (more than one shade of pigment)
C = Color variegation (more than one shade of pigment)
 D = Diameter increase (defined as a diameter greater than 6 mm)
D = Diameter increase (defined as a diameter greater than 6 mm)

153 How good is the 7-point checklist?
Several studies have found sensitivity of 79–100% and specificity of 30–37%.
155 What are the major clinical-histopathologic types of melanoma?
 Superficial spreading melanoma: The most common subtype (>70% of cases) and the one most frequently found near existing nevi. Onset is during the third to fifth decade, usually over the back of men, legs of women, and trunk of both genders. Lesions are flat or slightly raised, brown, variegated (with black, blue, pink, or white discoloration), >6 mm in diameter, and with irregular borders.
Superficial spreading melanoma: The most common subtype (>70% of cases) and the one most frequently found near existing nevi. Onset is during the third to fifth decade, usually over the back of men, legs of women, and trunk of both genders. Lesions are flat or slightly raised, brown, variegated (with black, blue, pink, or white discoloration), >6 mm in diameter, and with irregular borders.




Signs of Sun Damage
157 What are the characteristic signs of sun damage?
 Solar lentigo (lentigines): From the Latin lentigo (lentil), these are sun-induced, well-circumscribed, light brown or tan macules that resemble a freckle, except for regular border, microscopic proliferation of the rete ridges, and persistence even after the tan or sunburn fades. Typically on sun-exposed areas of the face, hands, and shoulders, they range in size between 5–20 mm. They have no potential for neoplastic degeneration, and yet a lentigo with black, pinhead-sized speckles (lentigo maligna) may degenerate over years into lentigo maligna melanoma.
Solar lentigo (lentigines): From the Latin lentigo (lentil), these are sun-induced, well-circumscribed, light brown or tan macules that resemble a freckle, except for regular border, microscopic proliferation of the rete ridges, and persistence even after the tan or sunburn fades. Typically on sun-exposed areas of the face, hands, and shoulders, they range in size between 5–20 mm. They have no potential for neoplastic degeneration, and yet a lentigo with black, pinhead-sized speckles (lentigo maligna) may degenerate over years into lentigo maligna melanoma.
 Freckles: From the Old English freken (ephelis), these are yellowish/brownish sun-induced macules on exposed areas, typical of light-complexioned individuals with red or blond hair. Lesions increase in number after exposure to the sun. The epidermis is microscopically normal, except for increased melanin. A freckle resembles a solar lentigo, except that (1) it appears early in life (lentigines do not occur until mid-adulthood); (2) it is usually smaller (only 1–2 mm in diameter); and (3) it may disappear with time. It has no malignant potential. Still, clustered freckles (especially over lips and fingertips) should raise the possibility of Peutz-Jeghers (see Chapter 6, question 74).
Freckles: From the Old English freken (ephelis), these are yellowish/brownish sun-induced macules on exposed areas, typical of light-complexioned individuals with red or blond hair. Lesions increase in number after exposure to the sun. The epidermis is microscopically normal, except for increased melanin. A freckle resembles a solar lentigo, except that (1) it appears early in life (lentigines do not occur until mid-adulthood); (2) it is usually smaller (only 1–2 mm in diameter); and (3) it may disappear with time. It has no malignant potential. Still, clustered freckles (especially over lips and fingertips) should raise the possibility of Peutz-Jeghers (see Chapter 6, question 74).


Solid Lesions: Yellow
158 What are the most common yellow lesions of the skin?
Cutaneous xanthomas and necrobiosis lipoidica (see also questions 258 and 259).
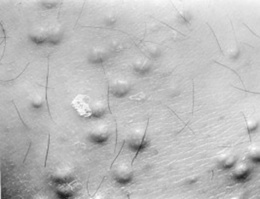
165 What are eruptive xanthomas?
Small and red-yellow papules on an erythematous base, typically erupting in crops over the buttocks, shoulders, and extensor surfaces of extremities (more rarely over the face or oral mucosa) (Fig. 3-35). Often pruritic and tender, they usually resolve spontaneously in a few weeks. Eruptive xanthomas are associated with hypertriglyceridemia, particularly types I, IV, and V (high very low-density lipoprotein [VLDL] level and chylomicrons), yet they also may occur in secondary hyperlipidemias, especially if related to diabetes.
Solid Lesions: Red or Purple—Table 3-4
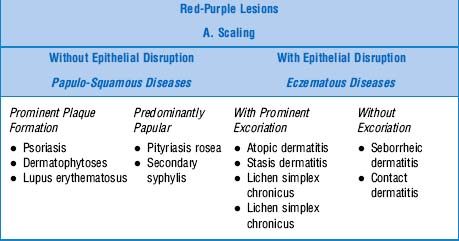
173 What is the typical clinical course of psoriasis?
One of variable extent and duration, even though usually as a lifelong disease. Spontaneous remissions occur with unpredictable frequency, and patients may move from one clinical form to another. Acute flares may evolve into more severe disease, such as pustular or erythrodermic (see question 174).
174 What are the other clinical presentations of psoriasis?
Psoriasis is a heterogeneous disorder with a spectrum of clinical variants:




179 How are dermatophytoses classified?
By the body region involved (Table 3-5). Note that fungal involvement can affect multiple sites. Hence, if you see lesions on the buttocks, always ask, “Can I see your feet?” Almost invariably there will be typical fungal lesions in the fourth web space.
| Disease | Location | Clinical Presentation |
|---|---|---|
| Tinea capitis | Scalp | Infection of scalp hair. It causes erythematous patches of alopecia and scaling, with broken hair. Kerion celsi, an inflammatory variant, produces tender abscesses with purulent drainage that may result int scarring alopecia. Favus (also termed tinea favosa) is severe tinea capitis with yellow, cup-shaped crusts around infected hair follicles. |
| Tinea corporis | Body | Infection of exposed areas of trunk and extremities. Characterized by circular lesions with central clearing and erythematous/raised edges (ringworm) eventually evolving into annular scaly plaques. May also present with pustules and vesicles. |
| Tinea faciale | Face | Red scaly plaques sometimes lacking central clearing and elevated border. |
| Tinea barbae | Beard | Infection of beard and neck area, characterized by erythema, scaling, and pustules. |
| Tinea cruris (jock itch) | Groin | Infection of groin and pubic region. Causes plaques with central clearing and raised scaly border. On inguinal fold and adjacent skin, but not scrotum. |
| Tinea manus | Hand | Infection of palms and finger webs, usually in association with tinea pedis. Lesions consist of annular plaques on the dorsum of hand, with hyperkeratosis of palms. Scaling and erythema may also be present. Affects only one hand (but often two feet). |
| Tinea pedis | Feet | Infection of interdigital webs, usually third and fourth. Presents with erythema, scaling, fissuring, and maceration (athlete’s foot). Hyperkeratosis and scaling may extend to the sole’s instep. Variations include bilateral moccasin distribution (scaling of soles and lateral surfaces) or vesicopustules on the instep. Onychomycosis may also occur, and is often the portal of entry for other tinea lesions. |
| Tinea unguium (onychomycosis) | Nail | Yellow-brown discoloration of nail plate associated with subungual hyperkeratosis. |
184 Who gets it?
Any age group, although usually 10- to 35-year-olds—women twice more frequently than men.




188 How is pityriasis rosea diagnosed?




190 What are the clinical features of atopic dermatitis?



191 Describe the distribution of atopic dermatitis lesions.
 Infants: Face (especially the cheeks) and extensor surfaces
Infants: Face (especially the cheeks) and extensor surfaces


Generalized involvement may develop at any age (see Fig. 3-36).

208 How is seborrheic dermatitis diagnosed?
By the typical clinical appearance. Biopsy is nondiagnostic.
Nonscaling Lesions—Table 3-6
Cherry Angiomas
209 What are cherry angiomas?
| Red-Purple Lesions | ||
|---|---|---|
| B. Nonscaling | ||
| Dome-Shaped | Flat-Topped | Drug Reactions |
| Inflammatory Papules | Vascular Reactions | Minor-to-Major |
| • Cherry angiomas | A. Nonpurpuric (Blanchable) | • Morbilliform fine pink papules |
| • Pyogenic granuloma | • Toxic erythema | • Urticaria |
| • Insect bites | • Urticaria | • Vasculitis |
| • Lichen planus | • Erythema multiforme | |
| • Erythema multiforme | • Stevens-Johnson | |
| • Erythema nodosum | • TEN | |
| • Vascular reactions | ||
| B. Purpuric (Nonblanchable) | ||
| • Palpable purpura | ||
| • Miscellaneous petechiae and ecchymotic disease | ||
211 Who gets lichen planus?
Men and women in their 40s; 10% have positive family history, suggesting genetic predisposition.
213 What other sites beside the skin may be involved?
LP can occur on mucous membranes, genitalia, nails (see question 38), and the scalp. The latter can progress to atrophic cicatricial alopecia.
Vascular Reactions
220 How are noninflammatory purpuras classified?
By size, shape, and depth. In this regard, blood extravasations can be divided into four groups:
 Petechiae: Superficial, pinpoint (<3 mm), red or purple, nonblanching macules. Mostly located on dependent areas, usually caused by platelet-related issues or vessel disease.
Petechiae: Superficial, pinpoint (<3 mm), red or purple, nonblanching macules. Mostly located on dependent areas, usually caused by platelet-related issues or vessel disease.

 Vibices: Linear purpuric lesions due to scratching
Vibices: Linear purpuric lesions due to scratching
 Hematomata: Deeper collections of blood within the skin. They may be fluctuant.
Hematomata: Deeper collections of blood within the skin. They may be fluctuant.
224 What are the characteristics of LCV lesions?
 Palpable purpura: The most common cutaneous small-vessel vasculitis. Lesions are usually on the legs, even though any area can be involved; round; small (1–3 mm in size, but at times coalescing into plaques); palpable (if only barely); and rarely ulcerated (a more common feature of large vessels vasculitis). Subungual splinter hemorrhages also may occur.
Palpable purpura: The most common cutaneous small-vessel vasculitis. Lesions are usually on the legs, even though any area can be involved; round; small (1–3 mm in size, but at times coalescing into plaques); palpable (if only barely); and rarely ulcerated (a more common feature of large vessels vasculitis). Subungual splinter hemorrhages also may occur.

226 What are the causes of cutaneous vasculitis?
It depends on the patient’s age:
1. In children the most common cause is Henoch-Schönlein purpura, followed at a great distance by leukocytoclastic hypersensitivity (i.e., drug reaction).
2. In adults, cutaneous vasculitis is often due to immune complexes, although other autoantibodies can do it, too. Yet, 30–50% of all cases are idiopathic. The rest are caused by:





Miscellaneous Disorders
Kaposi’s Sarcoma
227 What are the major types of Kaposi’s sarcoma? Describe each.
 Classic (traditional): Now relatively rare, this is the KS of shins or feet of older men of either Mediterranean or Eastern European descent (Ashkenazi Jews). It begins as purplish papules slowly progressing to plaques. Rarely fatal. In fact, most patients die with KS rather than of KS.
Classic (traditional): Now relatively rare, this is the KS of shins or feet of older men of either Mediterranean or Eastern European descent (Ashkenazi Jews). It begins as purplish papules slowly progressing to plaques. Rarely fatal. In fact, most patients die with KS rather than of KS.
 Epidemic (AIDS-associated): Present in more than one third of AIDS patients. Lesions are more varied and widespread than in the classic form, ranging from macules to papules, to plaques or ulcers, all red-purple in color (Fig. 3-37). Mean survival is 15–24 months, although antiretroviral therapy has extended it. Visceral involvement is common, including genital, oral, GI, and pulmonary sites.
Epidemic (AIDS-associated): Present in more than one third of AIDS patients. Lesions are more varied and widespread than in the classic form, ranging from macules to papules, to plaques or ulcers, all red-purple in color (Fig. 3-37). Mean survival is 15–24 months, although antiretroviral therapy has extended it. Visceral involvement is common, including genital, oral, GI, and pulmonary sites.

 Iatrogenic: From immunosuppression, may regress with its termination. Often with GI bleeding.
Iatrogenic: From immunosuppression, may regress with its termination. Often with GI bleeding.

228 What is the presentation of KS?
 Usually begins as bilateral and symmetric discrete skin patches, red or purple in color but occasionally violaceous, typically involving the lower extremities. These eventually become elevated, evolving into spongy nodules and plaques (localized nodular form).
Usually begins as bilateral and symmetric discrete skin patches, red or purple in color but occasionally violaceous, typically involving the lower extremities. These eventually become elevated, evolving into spongy nodules and plaques (localized nodular form).

 Finally, it may spare the skin and present with visceral involvement (including lymph nodes).
Finally, it may spare the skin and present with visceral involvement (including lymph nodes).

233 What are the cutaneous manifestations of LE?
 Acute cutaneous lupus erythematosus (ACLE)
Acute cutaneous lupus erythematosus (ACLE)
 Subacute cutaneous lupus erythematosus (SCLE)
Subacute cutaneous lupus erythematosus (SCLE)
 Chronic cutaneous lupus erythematosus (CCLE), also called discoid lupus (DLE)
Chronic cutaneous lupus erythematosus (CCLE), also called discoid lupus (DLE)
These are histopathologically similar but clinically very different.
237 What laboratory studies are positive in ACLE?




241 What is the association with discoid lupus erythematosus (DLE)?
Some SCLE patients can have lesions of DLE. Some may even develop small vessel vasculitis.
Syphilis
252 What are the primary lesions of syphilis?
 Primary syphilis: Classic lesion is the chancre, which occurs within 3 weeks at the site of treponemal penetration—usually the penis or scrotum in men (70%) and the vulva, cervix, or perineum in women (50%), but also any body region in both genders. The lesion begins as a 1–2 cm, single, round, and firm papule, rapidly evolving into a painless nonbleeding ulcer (the chancre) with raised indurated borders. Induration is key. In fact, the lesion can almost be flipped between fingers, as if it were a button under the skin. Chancres are highly infectious, but heal in 4–8 weeks—with or without therapy. Painless regional lymphadenopathy is common.
Primary syphilis: Classic lesion is the chancre, which occurs within 3 weeks at the site of treponemal penetration—usually the penis or scrotum in men (70%) and the vulva, cervix, or perineum in women (50%), but also any body region in both genders. The lesion begins as a 1–2 cm, single, round, and firm papule, rapidly evolving into a painless nonbleeding ulcer (the chancre) with raised indurated borders. Induration is key. In fact, the lesion can almost be flipped between fingers, as if it were a button under the skin. Chancres are highly infectious, but heal in 4–8 weeks—with or without therapy. Painless regional lymphadenopathy is common.


254 What are the other clinical presentations of syphilis?
 Syphilis in HIV-infected patients: Often difficult to diagnose, with negative serology, increased incidence of neurosyphilis, and persistence of disease even after adequate treatment.
Syphilis in HIV-infected patients: Often difficult to diagnose, with negative serology, increased incidence of neurosyphilis, and persistence of disease even after adequate treatment.
 Congenital syphilis: Due to transplacental spirochetal transmission. Infection is latent, becoming apparent during childhood and, in some cases, during adult life. The first symptom of early prenatal syphilis (before age 2) is rhinitis (snuffles), soon followed by cutaneous lesions. Manifestations of late prenatal syphilis (after age 2) include hearing and language abnormalities and vision problems. Facial and dental abnormalities also may be present (see Chapter 6, question 125, Hutchinson teeth and triad).
Congenital syphilis: Due to transplacental spirochetal transmission. Infection is latent, becoming apparent during childhood and, in some cases, during adult life. The first symptom of early prenatal syphilis (before age 2) is rhinitis (snuffles), soon followed by cutaneous lesions. Manifestations of late prenatal syphilis (after age 2) include hearing and language abnormalities and vision problems. Facial and dental abnormalities also may be present (see Chapter 6, question 125, Hutchinson teeth and triad).
Insect Infestations
255 What are the most common insect infestations?



Skin Manifestations of Systemic Disorders
268 Which sarcoid patients get EN?
Child-bearing women, especially those of North European lineage (particularly Scandinavians).
269 What is Löfgren’s syndrome?
A characteristic and febrile form of acute sarcoid that includes:




Acute and benign, the syndrome resolves spontaneously in 6–8 weeks.



275 Describe the skin lesions of BD.
Variously appearing. They occur in 58–97% of patients and include erythema nodosum-like manifestations (the most common), acneiform nodules, erythema multiforme-like lesions, and papulopustular eruptions. Often there is a positive pathergy test (see question 278).






Diabetes Mellitus



292 What about Raynaud’s phenomenon?
Raynaud’s phenomenon of the digits (but also the lips, nose, and ears) occurs in 5–15% of the general population and quite commonly in postmenopausal women. Of these, only 5% develop a connective tissue disease. In scleroderma, it may precede obvious skin changes by months or even years (see also Chapter 22, questions 5–9).
Sweet’s Syndrome
297 What is Sweet’s syndrome?
An acute febrile neutrophilic dermatosis that can be idiopathic or paraneoplastic. It was first described in 1964 by the British dermatologist Robert D. Sweet, who reported eight patients with fever, leukocytosis, and tender, erythematous plaques. Diagnostic criteria were eventually proposed in 1986 by Su and Liu, and subsequently modified by von den Driesch and colleagues. Both major criteria and at least two minor criteria are necessary for diagnosis (Table 3-7).
| Sweet’s Syndrome | |
|---|---|
| Major Criteria | Minor Criteria |
| • Abrupt onset of tender or painful erythematous or violaceous plaques or nodules | • Preceding fever or infection |
| • Predominantly neutrophilic infiltration in the dermis without leukocytoclastic vasculitis | • Accompanying fever, arthralgia, conjunctivitis, or underlying malignant lesion |
| • Leukocytosis, increased erythrocyte sedimentation rate | |
| • Good response to systemically administered corticosteroid but not to antibiotics | |
298 What are the skin lesions of Sweet’s syndrome?
They are edematous, tender, beefy-red or violaceous plaques or nodules that suddenly erupt over the face, neck, and extremities (Fig. 3-38). They often have a purulent base, with central clearing and ultimately ulceration. They also may be papular, pustular, vesicular, or bullous. Systemic signs and symptoms (such as fever, myalgias, arthralgias, or ocular involvement—like conjunctivitis) usually accompany the skin eruption. Neutrophilic leukocytosis and elevated sedimentation rate are common, too. Less common are pulmonary infiltrates and hepatic and renal involvement.
304 What are the unusual patterns of skin metastases?



1 Abbasi NR, Shaw HM, Rigel DS, et al. Early diagnosis of cutaneous melanoma: Revisiting the ABCD criteria. JAMA. 2004;292:2771-2776.
2 Arnold HL, Odom RB, James WD. Andrews’ Diseases of the Skin, 8th ed. Philadelphia: W.B. Saunders, 1990.
3 Conn RD, Smith RH. Malnutrition, myoedema and Muehrcke’s lines. Arch Intern Med. 1965;116:875-878.
4 Daniel CRIII, Osment LS. Nail pigmentation abnormalities. Cutis. 1980;25:595-607.
5 Daniel CR, Sams WM, Scher RK. Nails in systemic disease. Dermatol Clin. 1985;3:465-485.
6 Fawcett RS, et al. Nails as clues to systemic disease. Am Fam Physician. 2004;69:1417-1424.
7 Katta R. Cutaneous sarcoidosis: A dermatologic masquerader. Am Fam Physician. 2002;8:1581-1584.
8 Lynch PJ. Dermatology for the House Officer. Baltimore: Williams & Wilkins, 1982.
9 Mathur SK, Bhargava P. Insulin resistance and skin tags. Dermatology. 1997;195:184.
10 Muehrcke RC. The finger-nails in chronic hypoalbuminaemia. Br Med J. 1956;1:1327-1328.
11 Varma JR. Skin tags—a marker for colon polyps? J Am Board Fam Pract. 1990;3:175-180.
12 Whited JD, Grichnik JM, et al. Does this patient have a mole or a melanoma? JAMA. 1998;279:696-701.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
Chapter 3 The Skin
Basic Terminology and Diagnostic Techniques
1 How many skin diseases exist? What are the two main categories of skin lesions?
There are more than 1400 skin diseases. Yet, only 30 are important, common, and worth knowing. The first step toward their recognition is the separation of primary from secondary lesions (Table 3-1).
Primary lesions result only from disease and have not been changed by additional events (such as trauma, scratching, or medical treatment; see Table 3-1). To better identify primary lesions, pay attention to their colors, shape, arrangement, and distribution.
| skin lesions | ||
|---|---|---|
| Primary | Secondary | Special |
| Solid (Nonpalpable) | Crusts | Purpurae |
| • Macules (≤0.5 cm) | Scales | Petechiae |
| • Patches (>0.5 cm) | Ulcers | Ecchymoses |
| Fissures | Teleangiectasias | |
| Solid (Palpable) | Excorations | Comedones |
| • Papules (≤0.5 cm) | Scars | Burrows |
| • Plaques (>0.5 cm) | Erosions | Target lesions |
| • Nodules (deeper plaques) | Lichenification | |
| • Wheals (pruritic plaques) | Atrophy | |
| • Tumors (larger nodules) | Scars | |
| Sinuses | ||
| Fluid-Lesions | ||
| • Vesicles (fluid-filled papules) | ||
| • Pustules (pus-filled papules) | ||
| • Bullae (fluid-filled plaques) | ||
| • Cysts (fluid-filled nodules) | ||
2 What are the major primary lesions?
Macules: Flat, nonpalpable, circumscribed areas of discoloration ≤0.5 cm in diameter. Typical macules are the familiar freckles.
Tumors: Nodules that are either >2 cm in diameter or poorly demarcated. Usually neoplastic.
Pustules: Pus-filled papules. Typically seen in patients with impetigo or acne.
3 What are the major secondary lesions?
Excoriations: Linear erosions produced by scratching. Often raised, scratch marks may also present as crust on top of a primary lesion that has been partially scratched off. They are almost exclusively confined to the eczematous diseases.
Sinuses: Connective channels between the surface of the skin and deeper components.
4 Are there other ways to classify skin lesions?
Many ways. One divides lesions into four groups based on the relationship with the surrounding skin:
6 What is the configuration of a skin lesion?
It is the outline of the lesion as observed from above. The most common configurations are:
9 And so, what are the required components of a dermatologic diagnosis?
Morphology: Color, shape, dimensions (width and height, if necessary), elevation/depression, and palpable features (smoothness, induration, tenderness, scaling, and crusting)
Distribution (body location): Generalized versus localized
Distribution (arrangement to one another): Clustered, confluent, dermatomal
14 How should fingernails and toenails be assessed?
If covered by polish, clean them first with a solvent like acetone. Then pay attention to color and shape but also to anatomic details (Fig. 3-25):
15 What systemic conditions are associated with changes in nail shape or growth?
Clubbing: Inflammatory bowel disease, pulmonary malignancy, asbestosis, chronic bronchitis, chronic obstructive pulmonary disease, cirrhosis, congenital heart disease, endocarditis, atrioventricular malformation and fistulas (see also question 19)
Koilonychia (spoon nails) (Fig. 3-26): Iron deficiency anemia, hemochromatosis, Raynaud’s disease, systemic lupus disease, trauma, nail-patella syndrome
Pitting: Psoriasis, Reiter’s syndrome, incontinentia pigmenti, alopecia areata
Beau’s lines (see Fig. 3-26): Any severe systemic illness that disrupts nail growth, Raynaud’s disease, pemphigus, trauma
16 What systemic conditions are associated with changes in nail color?
Terry’s nails (see Fig. 3-26): Hepatic failure, cirrhosis, diabetes, congestive heart failure, hyperthyroidism, malnutrition
Azure lunula: Wilson’s disease, silver poisoning, quinacrine
Lindsay’s nails (half-and-half nails) (see Fig. 3-26): Specific for renal failure
Muehrcke’s lines: Specific for hypoalbuminemia
Lines of Mees’ (see Fig. 3-26): Arsenic poisoning, Hodgkin’s disease, congestive heart failure, leprosy, malaria, chemotherapy, carbon monoxide poisoning, other systemic insults
Longitudinal striations: Alopecia areata, vitiligo, atopic dermatitis, psoriasis
Telangiectasia: Rheumatoid arthritis, systemic lupus erythematosus, dermatomyositis, scleroderma
Nails
19 What is clubbing?
A condition that can be (1) idiopathic; (2) congenital (dominant trait); or (3) a clue to serious underlying pathology, including cardiovascular, hepatobiliary, mediastinal, endocrine, gastrointestinal, neoplastic, infectious, and, especially, pulmonary (see Chapter 13, questions 101–116).
22 What are the nail findings of psoriasis?
Pitting (previously discussed)
Beau’s lines in the proximal nail matrix (see later)
Leukonychia: Areas of white nail plate; due to parakeratotic foci in the mid-matrix
Subungual hyperkeratosis: Excessive proliferation of the nail bed that can lead to onycholysis
Nail plate crumbling: Weakened nail plate, bed, and matrix from diseased underlying structures
Dilated tortuous capillaries in the dermal papillae
Spotted lunula: Distal matrix involvement characterized by erythema of the lunula
26 What is longitudinal ridging (Reedy nails)?
A normal variant of patients older than 50, but one that also can occur in younger subjects. It may even represent a brittle nail variation. Ridges typically extend from the proximal nail fold to the distal plate, with some being very prominent, especially in older women. They are usually multiple, but at times may be single—like in patients with lichen planus (see questions 38 and 210–216).
38 What is lichen planus of the nail?
A condition present in 10% of patients with lichen planus. The most common finding is thinning of the nail plate, leading to longitudinal grooving and ridging (see also question 26). Hyperpigmentation, subungual hyperkeratosis, onycholysis, and longitudinal melanonychia can also be present.
41 What are azure half-moons in nail beds?
The nails of Wilson’s disease (hepatolenticular degeneration). Lunulae are not white, but bluish.
48 What is paronychia?
An acute or chronic inflammation of the perionychium, with redness, swelling, and tenderness.
Fluid-Filled Lesions: PUS (Pustules)—Table 3-2
Acne
54 What does acne look like?
| Fluid-Filled Lesions | ||
|---|---|---|
| Pus-Filled | Clear Fluid | |
| Pustular | Vesiculo-Bullous | Bullous |
| Acne vulgaris | H. simplex | Pemphygus vulgaris |
| Acne rosacea | H. zoster/varicella | Pemphygoid |
| Steroid acne | Dermatophytoses | Drug reactions |
| • Erythema multiforme | ||
| • Stevens-Johnson | ||
| • TEN | ||
| Folliculitis (bacterial/fungal) | Insect bites | Poison ivy/contact dermatitis |
| Intertriginous candidiasis | Dermatitis herpetiformis | Bullous impetigo |
| Porphyria cutanea tarda | ||
| Lupus erythematosus | ||
Fluid-Filled Lesions: Clear Fluid (Vesiculobullous Diseases)
62 What is the typical clinical course of herpes simplex?
63 What are the other clinical presentations of herpes simplex?
66 Who develops varicella?
Mostly children younger than 10 years. Only 5% of cases occur in subjects older than 15.
73 What are the other presentations of herpes zoster?
79 Are there any other causes of PV?
A form of PV (but also BP, see question 80) can be drug induced, resulting from penicillamine, captopril, thiol-containing compounds, and rifampin. Emotional stress can also trigger it. Finally, PV may occur in other autoimmune diseases, including myasthenia gravis and thymoma.
82 What is Asboe-Hansen sign?
Another sign of PV; lateral pressure on the edge of a blister may spread it into unaffected skin.
84 What is erythema multiforme (EM)?
A relatively benign process characterized by target or targetoid lesions, with or without blisters, in a symmetric and acral distribution. In fact, the rash favors palms and soles, dorsum of hands, face, and extensor surfaces of extremities (Fig. 3-27). It is often associated with oral lesions, but rarely involves more than one mucosal surface. Although it can be caused by drugs, it is most commonly a sequela of herpes virus infection. It has low morbidity, no mortality, but frequent recurrences. It may be associated with epidermal detachment, yet denudation always involves <10% of BSA.
85 What is Stevens-Johnson syndrome (SJS)?
A potential dermatologic emergency. First described in 1922 by the American pediatricians Albert Stevens and Frank Johnson, SJS is characterized by widespread purpuric macules and targetoid lesions, usually more common on face and torso, and with concomitant mucosal involvement of more than one site (usually the eyes, mouth, and genitalia; Fig. 3-28). Lesions may undergo full-thickness epidermal necrosis, although this is limited by definition to <10% of cutaneous surface. Hence, mortality is much less than in TEN (only 5%).
86 What is toxic epidermal necrolysis (TEN)?
Also known as Lyell’s syndrome, this is a true dermatologic emergency characterized by widespread skin and mucosal denudation. Skin lesions are erythematous and target-like macules associated with full-thickness epidermal necrosis and detachment of >30% BSA (Fig. 3-29). It is fatal in 50% of the cases, usually because of sepsis and respiratory distress. Mortality is related to BSA involvement: 11% for BSA (which is actually more of a SJS-TEN transitional form), and 35% for BSA >30%.
