Chapter 4 The Incidence of Anterior Cruciate Ligament Injury as a Function of Gender, Sport, and Injury-Reduction Programs
Methods
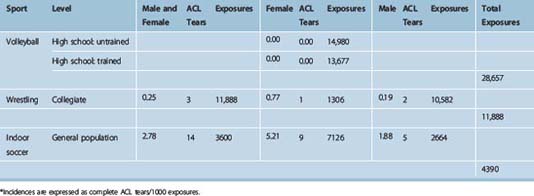
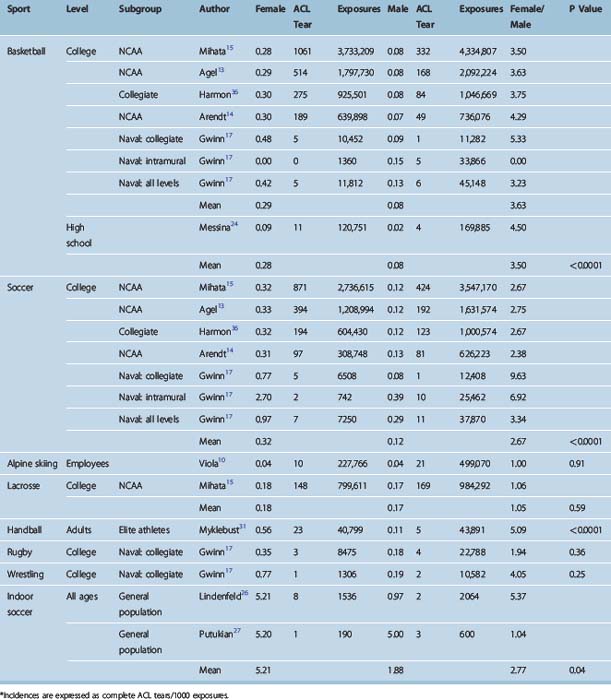
A computerized search of all papers in the peer-reviewed literature that had a possibility of dealing with the incidence of ACL tears was performed using a variety of indexing terms. Searches were then carried out by individual sports. This produced 793 articles that had some relation to knee or ACL injuries. These articles were reviewed, and bibliographies were cross-referenced for other papers, which were also reviewed for the purpose of identifying studies that had actual numerical incidences of complete ACL tears; this eliminated the overwhelming majority of papers. However, 33 papers were found that did have such quantitative data, and they form the basis for this chapter. Of these 33 papers, 25 had data that either used, or could be converted into, the preferred ACL injury incidence reporting method, namely: “ACL tears/1000 exposures.” An exposure is defined as either a practice or a game. These studies are listed in Table 4-1. They are divided by sport and then subdivided by level of competition, gender, and whether an ACL injury-reduction training program had been applied. The ratio of injury of females versus males is also listed for studies in which there were cohorts for both genders. These data form the basis for the analyses present in this chapter.
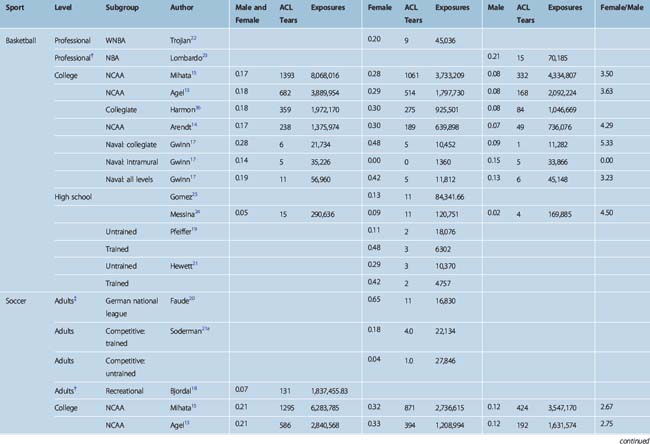
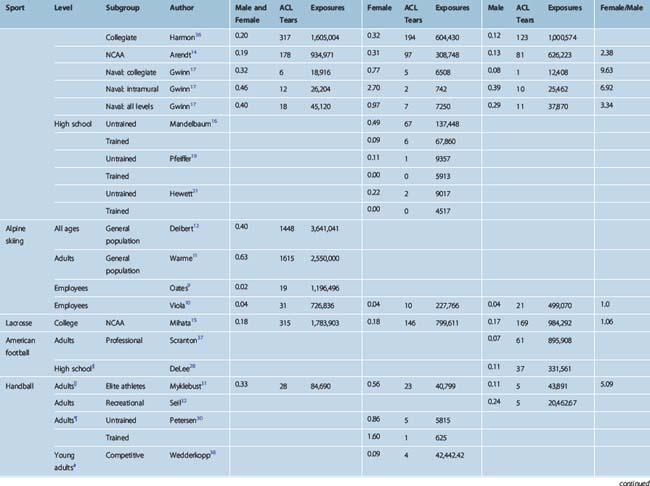
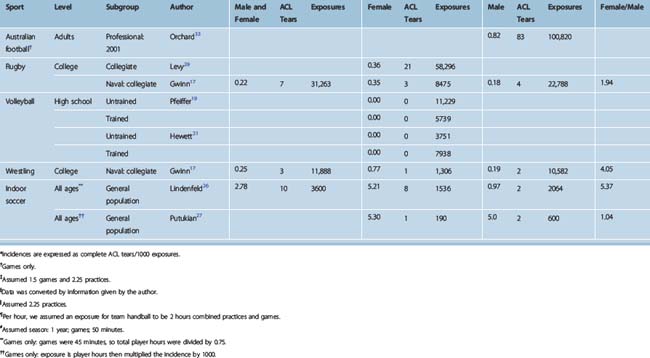
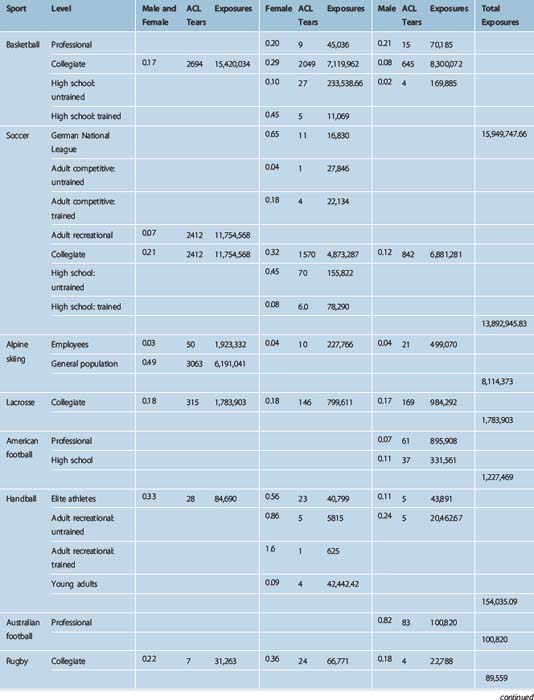
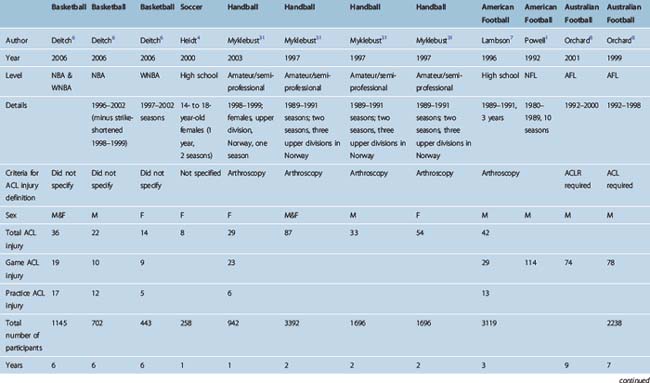
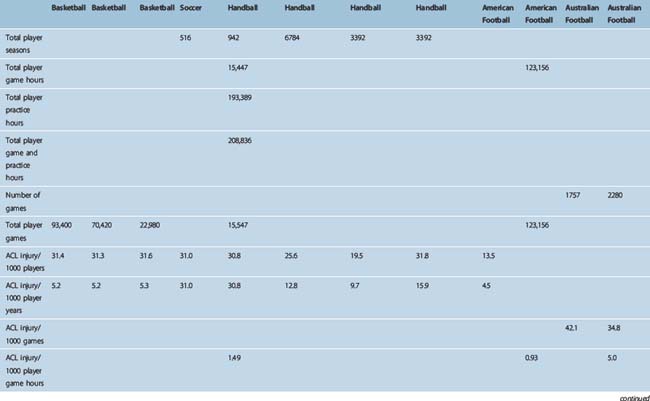
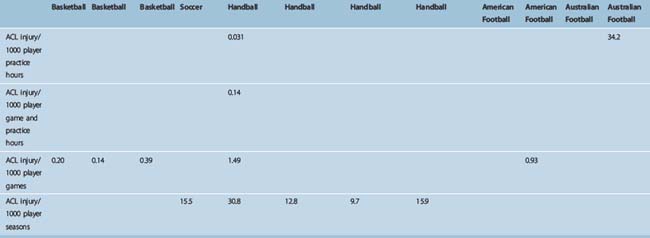
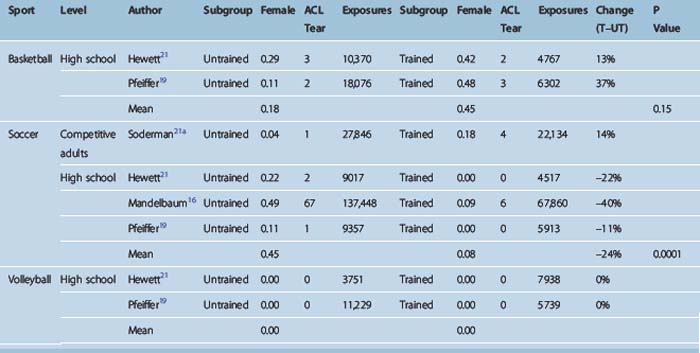
Table 4-2 aggregates like subgroups from Table 4-1 and provides mean injury rates weighted according to the number of exposures. Table 4-3 lists the remaining studies, which use methods other than “tears/1000 exposures”1–8. Table 4-4 aggregates the like populations from studies that compared incidences by gender. Table 4-5 lists all the studies that involved training regimens designed to reduce ACL tear incidence.
Data Conversions
A number of studies report their incidence by dividing the number of ACL tears by hours of participation instead of practices. In these studies the hourly incidence was therefore used to calculate an incidence per 1000 exposures by converting hours to practices or games and adjusting the incidence accordingly. Doing so allowed these series to be used in the comparative analysis with the other studies, which used the tear per exposure methodology. Without this method, a large number of useful studies would have been lost from the analysis. If an exact practice length was not listed, we assumed a practice length of 2.25 hours. In the study by DeLee,28 the data were presented in tears per hour, but exact data were given on number of practices and games and their lengths, so the data could be directly transformed into tears per 1000 exposures.
Individual Sports
Alpine Skiing
The alpine skiing data are notable for the large disparity in incidence between ski lodge employees, who are assumed to be expert skiers, and recreational skiers. The two studies of ski lodge employees by Oates and Viola show rates of 0.02 and 0.04, respectively.9,10 The two general population studies by Warme and Deibert show tenfold higher rates of 0.63 and 0.40, respectively.11,12 Although the rate for the expert skiers is the lowest for any of the high-risk sports studied, the rate for the recreational skiers is overall one of the highest (P < 0.001). It is remarkable that this huge disparity is produced by two independent studies in each group, each with a very large number of exposures. These observations are thus of high reliability and statistical power.
The lack of a gender difference in the large study by Viola10 is also remarkable. Aside from lacrosse, alpine skiing is the only sport studied with a large enough number of exposures to generate reliable numbers to find this lack of a gender difference.
Soccer
The soccer data are dominated by the three extremely large studies of Mihata, Agel, and Arendt.13–21 These data are remarkable for their amazing similarity. The female rates in the Mihata, Agel, and Arendt studies are 0.32, 0.33, and 0.31, respectively; the male rates are 0.12, 0.12, and 0.13, respectively. The female–male ratios are all also in the 2.5 to 1 range. The overall female to male difference was highly significant (P < 0.0001). Soccer is also notable in that in all three high school studies with ACL injury-reduction training program cohorts, the programs were apparently successful. (These studies were carried out only in females.) In other words, the trained athletes had significantly lower ACL injury rates (P = 0.0001) than the untrained athletes. These data are dominated by the landmark Mandelbaum et al study,16 which showed a 24% reduction in ACL tear incidence. It should be noted that the one adult study showed no reduction in ACL tear incidence with training.21a
Basketball
As was the case with soccer, the basketball rates are dominated by the three large studies of Mihata, Agel, and Arendt.* Also similar to soccer, the basketball numbers are amazingly similar among the studies. The female rates are 0.28, 0.29, and 0.30. The male rates are 0.08, 0.08, and 0.07. The female to male ratios are 3.5, 3.6, and 4.2. The overall difference in rate between females and males was highly significant (P < 0.0001). Interestingly, and unlike the case with soccer, the two studies that included a cohort in which athletes had completed a program to diminish the ACL tear incidence showed no reduction in ACL tear rate as a result of training. In fact, the trained athletes in both studies showed increased ACL tear rates versus the untrained athletes, although this difference was not significant.
Indoor Soccer
The two studies of indoor soccer are included for the sake of completeness, but with only about 3600 total exposures, they have negligible statistical power by comparison to the more than 10 million soccer exposures by the three large studies cited earlier for outdoor soccer.27,28 Thus the very high female incidence of 5.2 tears per 1000 exposures, more than 10 times the outdoor rate, should be interpreted with caution, although the difference between females and males was statistically significant (P = 0.04). Nonetheless it is of interest that two separate studies arrived at almost identically high rates. If these increased rates were real, there would be two obvious potential causes: first, the fact that this study included only games, not practices, implying a higher risk with competition. Second, the fact that indoor soccer is played on artificial turf, whereas outdoor soccer is played on grass, may upwardly influence the injury rate.
Volleyball
The two volleyball studies have only 28,000 exposures, again too small to make reliable incidence conclusions.19,21 However, it is remarkable that no ACL tears were recorded in either study. Basketball and soccer are often included with volleyball as high-risk sports for females. The rates of the six cohorts for basketball and soccer from each of the three large cited studies are all clustered between 0.28 and 0.33. If the average rate of 0.30 is applied to the 28,000 volleyball exposures, about 9 ACL tears would be expected. The fact that none were recorded may support a lower incidence of ACL tears in volleyball than in soccer and basketball.
Football
The one large football study, all in high school males, produced an injury rate of 0.11.29 This is very similar to the male rate found in college soccer (0.12) and basketball (0.08). With more than 331,000 exposures, this study is of high statistical power.
Rugby
The 0.35 and 0.36 rates for women and the 0.18 rate for men from the two published studies are very similar to the 0.32 rate for women and 0.12 rate for men found in soccer.17,30 This is not unexpected given the similarities of the sports, which involve running and pivoting on a grass surface. It is of interest that the higher level of contact in rugby did not produce a higher ACL tear rate. The 89,000 total exposures are a significant number, although far less than the soccer exposure numbers. Further supporting the validity of the data, however, is the fact that two separate rugby studies produced almost identical ACL tear incidences.
Wrestling
With just under 12,000 exposures, the one wrestling study is of low power.17 It showed a rate of 0.77 in females and 0.19 in males.
Lacrosse
There is one published study with usable data for our analysis.15 The 0.17 rate of ACL tear for men is similar to that of soccer, rugby, and basketball. The female rate of 0.18, however, is substantially lower than the female rates for these three sports. With 1,783,903 exposures, this study is of high statistical power. Lacrosse stands as the only sport aside from alpine skiing for which the rates for males and females are roughly the same. There is no obvious explanation. The argument has been made that the carrying of the stick is ACL tear protective and may be at least part of the reason for the lower injury rate in females. However, if this were true there would be no obvious explanation for the fact that such an effect does not serve to lower the rate in males compared with other similar sports.
Handball
The two published female cohorts both have very high incidences of 0.56 and 0.86.30,31 The two male cohorts of 0.24 and 0.11 are relatively unremarkable.31,32 The gender difference is significant (P < 0.0001).
Australian Rules Football
The one large published study with usable data showed a quite high ACL tear rate of 0.82 per 1000 exposures (games only in this study).33 This is quite high in relation to other sports for males. The 100,000 exposures represent a substantial number, although not as large as some studies. It is interesting to note that the indoor soccer study, which was also a games-only study, also had an unusually high tear rate of 0.97. This suggests the possibility that games have a higher risk of ACL tear than practices, although there are far too little data to make this conclusion. If this is not a contributing factor, other explanations would include an intrinsically high rate for Australian Rules football or that the rate is high due to chance in this modest-sized study.
The Overall Risk of Anterior Cruciate Ligament Tear
This chapter has focused on the rate per exposure in determining ACL risk. However, the number of exposures is equally, if not more, important. The proliferation of club teams for high-risk sports, especially soccer, thus combines a relatively high-incidence sport with a high yearly number of exposures, leading to an overall high risk. The year-round club soccer player’s ACL tear risk will be much higher than the now nearly extinct three-sport athlete of years past, many of whom would have engaged in at least one lower-risk sport such as softball, baseball, tennis, or swimming during the year. Hewett’s prospective study,34 for example, found a 4.4% 1-year chance of ACL tear in girls engaged in high-risk sports. For the injury rate of about 0.3 seen in girls’ basketball and soccer, a 5% yearly ACL risk would be seen after 167 yearly exposures–not an excessive number for a year-round player.1 Equipped with the incidence contained in this chapter, one need only plug in a putative number of yearly exposures to generate an approximate risk of yearly ACL tear.
Female–Male Injury Risk Ratio
The female–male ratio for the five sports for which there are reliable data is as follows: basketball, 3.5; soccer, 2.67; rugby, 2.0; lacrosse, 1.05; expert alpine skiers, 1.0. Soccer and basketball dwarf the other sports in level of participation and are the sports usually thought of when this topic is discussed. For these two sports, the increased risk versus males is overall about 3 to 1. This is obviously a higher rate of ACL tear in females versus males but is much less than the rates of 6 or even 8 to 135 that are sometimes cited.
Anterior Cruciate Ligament Tear-Prevention Programs
The published data have shown ACL injury-prevention programs to be effective in high school soccer. The data in this study, however, have shown no significant benefit in other sports. In this regard, Pfeiffer et al speculate that significant benefit may require strength and possibly flexibility training in addition to landing and agility training.19
Conclusions
The following conclusions can be made:
1 Powell JW, Schootman M. A multivariate risk analysis of selected playing surfaces in the national football league: 1980 to 1989. Am J Sports Med. 1992;20:686-694.
2 Myklebust G, Engebretsen L, Braekken IH, et al. Prevention of anterior cruciate ligament injuries in female team handball players. A prospective intervention study over three seasons. Clin J Sport Med. 2003;13:71-78.
3 Mykelbust G, Maehlum S, Engebretsen L, et al. Registration of cruciate ligament injuries in Norwegian top level team handball. A prospective study covering two seasons. Scand J Med Sci Sports. 1997;7:289-292.
4 Heidt RS, Sweeterman LM, Carlonas RL, et al. Avoidance of soccer injuries with preseason conditioning. Am J Sports Med. 2000;28:659-662.
5 Orchard J, Seward H, McGivern J, et al. Rainfall, evaporation and the risk of non-contact anterior cruciate ligament injury in the Australian football league. Med J Aust. 1999;170:304-306.
6 Deitch JR, Starkey C, Walters SL, et al. Injury risk in professional basketball players. Am J Sports Med. 2006;10:1-7.
7 Lambson RB, Barnhill BS, Higgins RW. Football cleat design and its effect on anterior cruciate ligament injuries. Am J Sports Med. 1996;24:155-159.
8 Orchard J. The AFL penetrometer study: work in progress. Aust J Sci Med Sport. 2001;4:220-232.
9 Oates KM, Van Eenenaam PV, Briggs K, et al. Comparative injury rates of uninjured, anterior cruciate ligament-deficient, and reconstructed knees in a skiing population. Am J Sports Med. 1999;27:606-610.
10 Viola RW, Steadman JR, Mair SD, et al. Anterior cruciate ligament injury incidence among male and female professional alpine skiers. Am J Sports Med. 1999;27:792-795.
11 Warme WJ, Feagin JA, King P, et al. Ski injury statistics, 1982 to 1993, Jackson Hole Ski Resort. Am J Sports Med. 1995;23:597-600.
12 Deibert MC, Aronsson DD, Johnson RJ, et al. Skiing injuries in children, adolescents, and adults. J Bone Joint Surg Am. 1998;80A:25-32.
13 Agel J, Arendt EA, Bershadsky B. Anterior cruciate ligament injury in national collegiate athletic association basketball and soccer. Am J Sports Med. 2005;33:524-531.
14 Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. Am J Sports Med. 1995;23:694-701.
15 Mihata LC, Beutler AI, Boden BP. Comparing the incidence of anterior cruciate ligament injury in collegiate lacrosse, soccer, and basketball players. Am J Sports Med. 2006;34:899-904.
16 Mandelbaum BR, Silvers HJ, Watanabe DS, et al. Effectiveness of a neuromuscular and proprioceptive training program in preventing the incidence of anterior cruciate ligament injuries in female athletes. Am J Sports Med. 2005;33:1-7.
17 Gwinn DE, Wilckens JH, McDevitt ER, et al. The relative incidence of anterior cruciate ligament injury in men and women at the United States Naval Academy. Am J Sports Med. 2000;28:98-102.
18 Bjordal JM, Arnoy F, Hannestad B, et al. Epidemiology of anterior cruciate ligament injuries in soccer. Am J Sports Med. 1997;25:341-345.
19 Pfeiffer RP, Shea KG, Roberts D, et al. Lack of effect of a knee ligament injury prevention program on the incidence of noncontact anterior cruciate ligament injury. J Bone Joint Surg. 2006;88:1769-1774.
20 Faude O, Junge A, Kindermann W, et al. Injuries in female soccer players. Am J Sports Med. 2005;33:1694-1700.
21 Hewett TE, Lindenfeld TN, Riccobene JV, et al. The effect of neuromuscular training on the incidence of knee injury in female athletes. Am J Sports Med. 1999;27:699-706.
21a Soderman K, Werner S, Pietila T, et al. Balance board training: Prevention of traumatic injuries of the lower extremities in female soccer players? Knee Surg Sports Traumatol Arthrosc. 2000;8:356-363.
22 Trojian TH, Collins S. The anterior cruciate ligament tear rate varies by race in professional women’s basketball. Am J Sports Med. 2006;10:1-4.
23 Lombardo S, Sethi PM, Starkey C. Intercondylar notch stenosis is not a risk factor for anterior cruciate ligament tears in professional male basketball players. Am J Sports Med. 2005;33:29-34.
24 Messina DF, Farney WC, DeLee JC. The incidence of injury in Texas high school basketball. Am J Sports Med. 1999;27:294-299.
25 Gomez E, DeLee JC, Farney WC. Incidence of injury in Texas girls’ high school basketball. Am J Sports Med. 1996;24:684-687.
26 Lindenfeld TN, Schmitt DJ, Hendy MP, et al. Incidence of injury in indoor soccer. Am J Sports Med. 1994;22:364-371.
27 Putukian M, Knowles WK, Swere S, et al. Injuries in indoor soccer. Am J Sports Med. 1996;24:317-322.
28 DeLee JC, Farney WC. Incidence of injury in Texas high school football. Am J Sports Med. 1992;20:575-580.
29 Levy AS, Wetzler MJ, Lewars M, et al. Knee injuries in women collegiate rugby players. Am J Sports Med. 1997;25:360-362.
30 Petersen W, Braun C, Bock W, et al. A controlled prospective case control study of a prevention training program in female team handball players: the German experience. Arch Orthop Trauma Surg. 2005;9:614-621.
31 Myklebust G, Maehlum S, Holm I, et al. A prospective cohort study of anterior cruciate ligament injuries in elite Norwegian team handball. Scand J Med Sci Sports. 1998;8:149-153.
32 Seil R, Rupp S, Tempelhof S, et al. Sports injuries in team handball. Am J Sports Med. 1998;26:681-687.
33 Orchard J, Seward H, McGivern J, et al. Intrinsic and extrinsic risk factors for anterior cruciate ligament injury in Australian footballers. Am J Sports Med. 2001;29:196-200.
34 Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes. Am J Sports Med. 2005;33:492-501.
35 Toth AP, Cordasco FA. Anterior cruciate ligament injuries in the female athlete. J Gend Specif Med. 2001;4:25-34.
36 Harmon KG, Dick R. The relationship of skill level to anterior cruciate ligament injury. Clin J Sport Med. 1998;8:260-265.
37 Scranton PEJr., Whitesel JP, Powell JW, et al. A review of selected noncontact anterior cruciate ligament injuries in the National Football League. Foot Ankle Int. 1997;18:772-776.
38 Wedderkopp N, Kaltoft M, Lundgaard B, et al. Injuries in young female players in European team handball. Scand J Med Sci Sports. 1997;7:342-347.






