Chapter 8 The First Year
Advances in imaging permit us to understand the anatomic and physiologic correlates of the physical growth, maturation, acquisition of competence, and psychologic reorganization that characterizes infancy and radically change the infant’s behavior and social relationships. Some activities previously thought to be “primitive” or “reflexive” result from complex systems. Swallowing, rather than a simple reflex, results from a complex highly coordinated process involving multiple levels of neural control distributed among several physiologic systems whose nature and relationships mature throughout the 1st year of life. Substantial learning of the basic tools of language (phonology, word segmentation) occurs during infancy. Speech processing in older individuals requires defined and precise neuronal networks; imaging studies have revealed that the infant brain possesses a structural and functional organization similar to that of adults, leading to the belief that structural neurologic processing of speech may guide infants to discover the properties of his or her native language. Myelination of the cortex begins at 8 mo gestation and is nearly complete by age 2 yr; much of this process occurs during infancy. Given the importance of iron and other nutrients in myelination, adequate stores throughout infancy are critical (Chapter 42). Inadequate dietary intake, insufficient interactions with caregivers, or both may alter experience-dependent processes that are critical to brain structure development and function during infancy. Although some of these processes may be delayed, as the periods of plasticity close during the rapid developmental changes occurring in infancy, more permanent deficits may result.
The infant acquires new competences in all developmental domains. The concept of developmental trajectories recognizes that complex skills build on simpler ones; it is also important to realize how development in each domain affects functioning in all of the others. Physical growth parameters and normal ranges for attainable weight, length, and head circumference are found in the Centers for Disease Control and Prevention growth charts (see Figs. 9-1 and 9-2 on the Nelson Textbook of Pediatrics website at www.expertconsult.com  ). Table 8-1 presents an overview of key milestones by domain; Table 8-2 presents similar information arranged by age. Table 8-3 presents age at time of appearance on x-ray of centers of ossification. Parents often seek information about “normal development” during this period and should be directed to reliable sources, including the American Academy of Pediatrics website (www.AAP.org).
). Table 8-1 presents an overview of key milestones by domain; Table 8-2 presents similar information arranged by age. Table 8-3 presents age at time of appearance on x-ray of centers of ossification. Parents often seek information about “normal development” during this period and should be directed to reliable sources, including the American Academy of Pediatrics website (www.AAP.org).
Table 8-1 DEVELOPMENTAL MILESTONES IN THE FIRST 2 YR OF LIFE
| MILESTONE | AVERAGE AGE OF ATTAINMENT (MO) | DEVELOPMENTAL IMPLICATIONS |
|---|---|---|
| GROSS MOTOR | ||
| Holds head steady while sitting | 2 | Allows more visual interaction |
| Pulls to sit, with no head lag | 3 | Muscle tone |
| Brings hands together in midline | 3 | Self-discovery of hands |
| Asymmetric tonic neck reflex gone | 4 | Can inspect hands in midline |
| Sits without support | 6 | Increasing exploration |
| Rolls back to stomach | 6.5 | Truncal flexion, risk of falls |
| Walks alone | 12 | Exploration, control of proximity to parents |
| Runs | 16 | Supervision more difficult |
| FINE MOTOR | ||
| Grasps rattle | 3.5 | Object use |
| Reaches for objects | 4 | Visuomotor coordination |
| Palmar grasp gone | 4 | Voluntary release |
| Transfers object hand to hand | 5.5 | Comparison of objects |
| Thumb-finger grasp | 8 | Able to explore small objects |
| Turns pages of book | 12 | Increasing autonomy during book time |
| Scribbles | 13 | Visuomotor coordination |
| Builds tower of 2 cubes | 15 | Uses objects in combination |
| Builds tower of 6 cubes | 22 | Requires visual, gross, and fine motor coordination |
| COMMUNICATION AND LANGUAGE | ||
| Smiles in response to face, voice | 1.5 | More active social participant |
| Monosyllabic babble | 6 | Experimentation with sound, tactile sense |
| Inhibits to “no” | 7 | Response to tone (nonverbal) |
| Follows one-step command with gesture | 7 | Nonverbal communication |
| Follows one-step command without gesture | 10 | Verbal receptive language (e.g., “Give it to me”) |
| Says “mama” or “dada” | 10 | Expressive language |
| Points to objects | 10 | Interactive communication |
| Speaks first real word | 12 | Beginning of labeling |
| Speaks 4-6 words | 15 | Acquisition of object and personal names |
| Speaks 10-15 words | 18 | Acquisition of object and personal names |
| Speaks 2-word sentences (e.g., “Mommy shoe”) | 19 | Beginning grammaticization, corresponds with 50 word vocabulary |
| COGNITIVE | ||
| Stares momentarily at spot where object disappeared | 2 | Lack of object permanence (out of sight, out of mind [e.g., yarn ball dropped]) |
| Stares at own hand | 4 | Self-discovery, cause and effect |
| Bangs 2 cubes | 8 | Active comparison of objects |
| Uncovers toy (after seeing it hidden) | 8 | Object permanence |
| Egocentric symbolic play (e.g., pretends to drink from cup) | 12 | Beginning symbolic thought |
| Uses stick to reach toy | 17 | Able to link actions to solve problems |
| Pretend play with doll (e.g., gives doll bottle) | 17 | Symbolic thought |
Table 8-2 EMERGING PATTERNS OF BEHAVIOR DURING THE 1ST YEAR OF LIFE*
| NEONATAL PERIOD (1ST 4 WK) | |
| Prone: | Lies in flexed attitude; turns head from side to side; head sags on ventral suspension |
| Supine: | Generally flexed and a little stiff |
| Visual: | May fixate face on light in line of vision; “doll’s-eye” movement of eyes on turning of the body |
| Reflex: | Moro response active; stepping and placing reflexes; grasp reflex active |
| Social: | Visual preference for human face |
| AT 1 MO | |
| Prone: | Legs more extended; holds chin up; turns head; head lifted momentarily to plane of body on ventral suspension |
| Supine: | Tonic neck posture predominates; supple and relaxed; head lags when pulled to sitting position |
| Visual: | Watches person; follows moving object |
| Social: | Body movements in cadence with voice of other in social contact; beginning to smile |
| AT 2 MO | |
| Prone: | Raises head slightly farther; head sustained in plane of body on ventral suspension |
| Supine: | Tonic neck posture predominates; head lags when pulled to sitting position |
| Visual: | Follows moving object 180 degrees |
| Social: | Smiles on social contact; listens to voice and coos |
| AT 3 MO | |
| Prone: | Lifts head and chest with arms extended; head above plane of body on ventral suspension |
| Supine: | Tonic neck posture predominates; reaches toward and misses objects; waves at toy |
| Sitting: | Head lag partially compensated when pulled to sitting position; early head control with bobbing motion; back rounded |
| Reflex: | Typical Moro response has not persisted; makes defensive movements or selective withdrawal reactions |
| Social: | Sustained social contact; listens to music; says “aah, ngah” |
| AT 4 MO | |
| Prone: | Lifts head and chest, with head in approximately vertical axis; legs extended |
| Supine: | Symmetric posture predominates, hands in midline; reaches and grasps objects and brings them to mouth |
| Sitting: | No head lag when pulled to sitting position; head steady, tipped forward; enjoys sitting with full truncal support |
| Standing: | When held erect, pushes with feet |
| Adaptive: | Sees pellet, but makes no move to reach for it |
| Social: | Laughs out loud; may show displeasure if social contact is broken; excited at sight of food |
| AT 7 MO | |
| Prone: | Rolls over; pivots; crawls or creep-crawls (Knobloch) |
| Supine: | Lifts head; rolls over; squirms |
| Sitting: | Sits briefly, with support of pelvis; leans forward on hands; back rounded |
| Standing: | May support most of weight; bounces actively |
| Adaptive: | Reaches out for and grasps large object; transfers objects from hand to hand; grasp uses radial palm; rakes at pellet |
| Language: | Forms polysyllabic vowel sounds |
| Social: | Prefers mother; babbles; enjoys mirror; responds to changes in emotional content of social contact |
| AT 10 MO | |
| Sitting: | Sits up alone and indefinitely without support, with back straight |
| Standing: | Pulls to standing position; “cruises” or walks holding on to furniture |
| Motor: | Creeps or crawls |
| Adaptive: | Grasps objects with thumb and forefinger; pokes at things with forefinger; picks up pellet with assisted pincer movement; uncovers hidden toy; attempts to retrieve dropped object; releases object grasped by other person |
| Language: | Repetitive consonant sounds (“mama,” “dada”) |
| Social: | Responds to sound of name; plays peek-a-boo or pat-a-cake; waves bye-bye |
| AT 1 YR | |
| Motor: | Walks with one hand held (48 wk); rises independently, takes several steps (Knobloch) |
| Adaptive: | Picks up pellet with unassisted pincer movement of forefinger and thumb; releases object to other person on request or gesture |
| Language: | Says a few words besides “mama,” “dada” |
| Social: | Plays simple ball game; makes postural adjustment to dressing |
* Data are derived from those of Gesell (as revised by Knobloch), Shirley, Provence, Wolf, Bailey, and others.
From Knobloch H, Stevens F, Malone AF: Manual of developmental diagnosis, Hagerstown, MD, 1980, Harper & Row.
Table 8-3 TIME OF APPEARANCE IN X-RAYS OF CENTERS OF OSSIFICATION IN INFANCY AND CHILDHOOD
| BOYS—AGE AT APPEARANCE* | BONES AND EPIPHYSEAL CENTERS | GIRLS—AGE AT APPEARANCE* |
|---|---|---|
| HUMERUS, HEAD | ||
| 3 wk | 3 wk | |
| CARPAL BONES | ||
| 2 mo ± 2 mo | Capitate | 2 mo ± 2 mo |
| 3 mo ± 2 mo | Hamate | 2 mo ± 2 mo |
| 30 mo ± 16 mo | Triangular† | 21 mo ± 14 mo |
| 42 mo ± 19 mo | Lunate† | 34 mo ± 13 mo |
| 67 mo ± 19 mo | Trapezium† | 47 mo ± 14 mo |
| 69 mo ± 15 mo | Trapezoid† | 49 mo ± 12 mo |
| 66 mo ± 15 mo | Scaphoid† | 51 mo ± 12 mo |
| No standards available | Pisiform† | No standards available |
| METACARPAL BONES | ||
| 18 mo ± 5 mo | II | 12 mo ± 3 mo |
| 20 mo ± 5 mo | III | 13 mo ± 3 mo |
| 23 mo ± 6 mo | IV | 15 mo ± 4 mo |
| 26 mo ± 7 mo | V | 16 mo ± 5 mo |
| 32 mo ± 9 mo | I | 18 mo ± 5 mo |
| FINGERS (EPIPHYSES) | ||
| 16 mo ± 4 mo | Proximal phalanx, 3rd finger | 10 mo ± 3 mo |
| 16 mo ± 4 mo | Proximal phalanx, 2nd finger | 11 mo ± 3 mo |
| 17 mo ± 5 mo | Proximal phalanx, 4th finger | 11 mo ± 3 mo |
| 19 mo ± 7 mo | Distal phalanx, 1st finger | 12 mo ± 4 mo |
| 21 mo ± 5 mo | Proximal phalanx, 5th finger | 14 mo ± 4 mo |
| 24 mo ± 6 mo | Middle phalanx, 3rd finger | 15 mo ± 5 mo |
| 24 mo ± 6 mo | Middle phalanx, 4th finger | 15 mo ± 5 mo |
| 26 mo ± 6 mo | Middle phalanx, 2nd finger | 16 mo ± 5 mo |
| 28 mo ± 6 mo | Distal phalanx, 3rd finger | 18 mo ± 4 mo |
| 28 mo ± 6 mo | Distal phalanx, 4th finger | 18 mo ± 5 mo |
| 32 mo ± 7 mo | Proximal phalanx, 1st finger | 20 mo ± 5 mo |
| 37 mo ± 9 mo | Distal phalanx, 5th finger | 23 mo ± 6 mo |
| 37 mo ± 8 mo | Distal phalanx, 2nd finger | 23 mo ± 6 mo |
| 39 mo ± 10 mo | Middle phalanx, 5th finger | 22 mo ± 7 mo |
| 152 mo ± 18 mo | Sesamoid (adductor pollicis) | 121 mo ± 13 mo |
| HIP AND KNEE | ||
| Usually present at birth | Femur, distal | Usually present at birth |
| Usually present at birth | Tibia, proximal | Usually present at birth |
| 4 mo ± 2 mo | Femur, head | 4 mo ± 2 mo |
| 46 mo ± 11 mo | Patella | 29 mo ± 7 mo |
| FOOT AND ANKLE‡ | ||
Values represent mean ± standard deviation, when applicable.
† Except for the capitate and hamate bones, the variability of carpal centers is too great to make them very useful clinically.
‡ Standards for the foot are available, but normal variation is wide, including some familial variants, so this area is of little clinical use.
The norms present a composite of published data from the Fels Research Institute, Yellow Springs, OH (Pyle SI, Sontag L: AJR Am J Roentgenol 49:102, 1943), and unpublished data from the Brush Foundation, Case Western Reserve University, Cleveland, OH, and the Harvard School of Public Health, Boston, MA. Compiled by Lieb, Buehl, and Pyle.
Age 0-2 Months
Physical Development
A newborn’s weight may initially decrease 10% below birthweight in the 1st wk as a result of excretion of excess extravascular fluid and limited nutritional intake. Nutrition improves as colostrum is replaced by higher-fat breast milk, as infants learn to latch on and suck more efficiently, and as mothers become more comfortable with feeding techniques. Infants regain or exceed birthweight by 2 wk of age and should grow at approximately 30 g (1 oz)/day during the 1st mo (see Table 13-1). This is the period of fastest postnatal growth. Limb movements consist largely of uncontrolled writhing, with apparently purposeless opening and closing of the hands. Smiling occurs involuntarily. Eye gaze, head turning, and sucking are under better control and thus can be used to demonstrate infant perception and cognition. An infant’s preferential turning toward the mother’s voice is evidence of recognition memory.
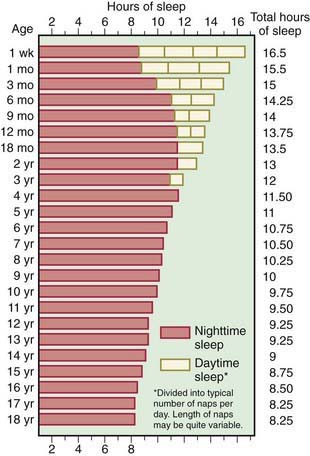
Six behavioral states have been described (Chapter 7). Initially, sleep and wakefulness are evenly distributed throughout the 24-hr day (Fig. 8-1). Neurologic maturation accounts for the consolidation of sleep into blocks of 5 or 6 hr at night, with brief awake, feeding periods. Learning also occurs; infants whose parents are consistently more interactive and stimulating during the day learn to concentrate their sleeping during the night.
Emotional Development
The infant is dependent on the environment to meet his or her needs. The consistent availability of a trusted adult to meet the infant’s urgent needs creates the conditions for secure attachment. Basic trust vs mistrust, the first of Erikson’s psychosocial stages (Chapter 6), depends on attachment and reciprocal maternal bonding. Crying occurs in response to stimuli that may be obvious (a soiled diaper), but are often obscure. Infants who are consistently picked up and held in response to distress cry less at 1 yr and show less aggressive behavior at 2 yr. Cross-cultural studies show that in societies in which infants are carried close to the mother, babies cry less than in societies in which babies are only periodically carried. Crying normally peaks at about 6 wk of age, when healthy infants may cry up to 3 hr/day, then decreases to 1 hr or less by 3 mo.
The emotional significance of any experience depends on both the individual child’s temperament and the parent’s responses (see Table 6-1); differing feeding schedules produce differing reactions. Hunger generates increasing tension; as the urgency peaks, the infant cries, the parent offers the breast or bottle and the tension dissipates. Infants fed “on demand” consistently experience this link between their distress, the arrival of the parent, and relief from hunger. Most infants fed on a fixed schedule quickly adapt their hunger cycle to the schedule. Those who cannot because they are temperamentally prone to irregular biologic rhythms experience periods of unrelieved hunger as well as unwanted feedings when they already feel full. Similarly, infants who are fed at the parents’ convenience, with neither attention to the infant’s hunger cues nor a fixed schedule may not consistently experience feeding as the pleasurable reduction of tension. These infants often show increased irritability and physiologic instability (spitting, diarrhea, poor weight gain) as well as later behavioral problems.
Implications for Parents and Pediatricians
Success or failure in establishing feeding and sleep cycles determines parents’ feelings of efficacy. When things go well, the parents’ anxiety and ambivalence, as well as the exhaustion of the early weeks, decrease. Infant issues (colic) or familial conflict will prevent this from occurring. With physical recovery from delivery and endocrinologic normalization, the mild postpartum depression that affects many mothers passes. If the mother continues to feel sad, overwhelmed, and anxious, the possibility of moderate to severe postpartum depression, found in 10% of postpartum women, needs to be considered. Major depression that arises during pregnancy or in the postpartum period threatens the mother-child relationship and is a risk factor for later cognitive and behavioral problems. The pediatrician may be the first professional to encounter the depressed mother and should be instrumental in assisting her in seeking treatment (Chapter 7).
Age 2-6 Months
Physical Development
Between 3 and 4 mo of age, the rate of growth slows to approximately 20 g/day (see Table 13-1; see Figs. 9-1 and 9-2 on the Nelson Textbook of Pediatrics website  at www.expertconsult.com). By 4 mo, birthweight is doubled. Early reflexes that limited voluntary movement recede. Disappearance of the asymmetric tonic neck reflex means that infants can begin to examine objects in the midline and manipulate them with both hands (Chapter 584). Waning of the early grasp reflex allows infants both to hold objects and to let them go voluntarily. A novel object may elicit purposeful, although inefficient, reaching. The quality of spontaneous movements also changes, from larger writhing to smaller, circular movements that have been described as “fidgety.” Abnormal or absent fidgety movements may constitute a risk factor for later neurologic abnormalities.
at www.expertconsult.com). By 4 mo, birthweight is doubled. Early reflexes that limited voluntary movement recede. Disappearance of the asymmetric tonic neck reflex means that infants can begin to examine objects in the midline and manipulate them with both hands (Chapter 584). Waning of the early grasp reflex allows infants both to hold objects and to let them go voluntarily. A novel object may elicit purposeful, although inefficient, reaching. The quality of spontaneous movements also changes, from larger writhing to smaller, circular movements that have been described as “fidgety.” Abnormal or absent fidgety movements may constitute a risk factor for later neurologic abnormalities.
In this period, infants achieve stable state regulation and regular sleep-wake cycles. Total sleep requirements are approximately 14-16 hr/24 hr, with about 9-10 hr concentrated at night and 2 naps/day. About 70% of infants sleep for a 6-8 hr stretch by age 6 mo (see Fig. 8-1). By 4-6 mo, the sleep electroencephalogram shows a mature pattern, with demarcation of rapid eye movement (REM) and 4 stages of non-REM sleep. The sleep cycle remains shorter than in adults (50-60 min vs approximately 90 min). As a result, infants arouse to light sleep or wake frequently during the night, setting the stage for behavioral sleep problems (Chapter 17).
Age 6-12 Months
Physical Development
Growth slows more (see Table 13-1; see Figs. 9-1 and 9-2 on the Nelson Textbook of  Pediatrics website at www.expertconsult.com). By the 1st birthday, birthweight has tripled, length has increased by 50%, and head circumference has increased by 10 cm. The ability to sit unsupported (6-7 mo) and to pivot while sitting (around 9-10 mo) provides increasing opportunities to manipulate several objects at a time and to experiment with novel combinations of objects. These explorations are aided by the emergence of a thumb-finger grasp (8-9 mo) and a neat pincer grasp by 12 mo. Many infants begin crawling and pulling to stand around 8 mo, followed by cruising. Some walk by 1 yr. Motor achievements correlate with increasing myelinization and cerebellar growth. These gross motor skills expand infants’ exploratory range and create new physical dangers as well as opportunities for learning. Tooth eruption occurs, usually starting with the mandibular central incisors. Tooth development reflects skeletal maturation and bone age, although there is wide individual variation (see Table 8-3 and Chapter 299).
Pediatrics website at www.expertconsult.com). By the 1st birthday, birthweight has tripled, length has increased by 50%, and head circumference has increased by 10 cm. The ability to sit unsupported (6-7 mo) and to pivot while sitting (around 9-10 mo) provides increasing opportunities to manipulate several objects at a time and to experiment with novel combinations of objects. These explorations are aided by the emergence of a thumb-finger grasp (8-9 mo) and a neat pincer grasp by 12 mo. Many infants begin crawling and pulling to stand around 8 mo, followed by cruising. Some walk by 1 yr. Motor achievements correlate with increasing myelinization and cerebellar growth. These gross motor skills expand infants’ exploratory range and create new physical dangers as well as opportunities for learning. Tooth eruption occurs, usually starting with the mandibular central incisors. Tooth development reflects skeletal maturation and bone age, although there is wide individual variation (see Table 8-3 and Chapter 299).
Cognitive Development
The 6 mo old infant has discovered his hands and will soon learn to manipulate objects. At first, everything goes into the mouth. In time, novel objects are picked up, inspected, passed from hand to hand, banged, dropped, and then mouthed. Each action represents a nonverbal idea about what things are for (in Piagetian terms, a schema; Chapter 6). The complexity of an infant’s play, how many different schemata are brought to bear, is a useful index of cognitive development at this age. The pleasure, persistence, and energy with which infants tackle these challenges suggest the existence of an intrinsic drive or mastery motivation. Mastery behavior occurs when infants feel secure; those with less secure attachments show limited experimentation and less competence.
Barlow SM. Central pattern generation involved in oral and respiratory control for feeding in the term infant. Curr Opin Otolaryngol Head Neck Surg. 2009;17(3):187-193.
Brazelton TB. Touchpoints: the essential reference. Reading, MA: Addison-Wesley; 1992.
Carlson EA, Sampson MC, Sroufe LA. Implications of attachment theory and research for developmental-behavioral pediatrics. J Dev Behav Pediatr. 2003:364-379.
Carberry AE, Colditz PB, Lingwood BE. Body composition from birth to 4.5 months in infants born to non-obese women. Pediatr Res. 2010;68(1):84-88.
Centers for Disease Control. Use of World Health Organization and CDC growth charts for children aged 0–59 months in the United States. MMWR. 2010;59(No. RR-9):1-15.
Dehaene-Lambertz G, Hertz-Pannier L, Dubois J. Nature and nurture in language acquisition: anatomical and functional brain-imaging studies in infants. Trends Neurosci. 2006;29(7):367-373.
Dorea JG. Breastfeeding is an essential complement to vaccination. Acta Paediatr. 2009;98:1244-1250.
Fernald LCH, Gertler PJ, Neufeld LM. 10-year effect of oportunidades, Mexico’s conditional cash transfer programme, on child growth, cognition, language and behavior: a longitudinal follow-up study. Lancet. 2009;374:1997-2005.
Hunziker UA, Barr RG. Increased carrying reduces infant crying: a randomized controlled trial. Pediatrics. 1986;77:641-648.
Jusczyk PW. Chunking language input to find patterns. In: Rakison DH, Oakes LM, editors. Early category and concept development: making sense of the blooming, buzzing confusion. New York: Oxford University Press, 2003.
Kelly Y, Sacker A, Schoon I, et al. Ethic differences in achievement of developmental milestones by 9 months of age: the millennium cohort study. Dev Med Child Neurol. 2006;48:825-830.
Kuhl PK. Human speech and birdsong: communication and the social brain. Proc Natl Acad Sci U S A. 2003;100:9645-9646.
Lozoff B, Beard J, Connor J, et al. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr Rev. 2006;64(5 Pt 2):S34-S43.
McLearn KT, Minkovitz CS, Strobino DM, et al. The timing of maternal depressive symptoms and mothers’ parenting practices with young children: implications for pediatric practice. Pediatrics. 2006;118:e174-e182.
Mindell JA, Owens JA. A clinical guide to pediatric sleep: diagnosis and management of sleep problems. Philadelphia: Lippincott Williams & Wilkins; 2003.
Rollins JD, Collins JS, Holden KR. United States head circumferance growth reference charts: birth to 21 years. J Pediatr. 2010;156:907-913.
Stern D. The interpersonal world of the infant. New York: Basic Books; 1985.
Williams N, Mughal S, Blair M. ‘Is my child developing normally?’: a critical review of web-based resources for parents. Dev Med Child Neurol. 2008;50(12):893-897.
Wright CM, Williams AF, Elliman D, et al. Using the new UK-WHO growth charts. BMJ. 2010;340:c1140.




