Chapter 9 The Breast
A. Generalities



(1) Inspection
9 Which areas should be examined?
Breast tissue is contained in an imaginary pentagon, whose lateral border follows the midaxillary line, from the middle of the axilla down to the inframammary (or bra) line (fifth to sixth interspace); the lower border crosses along the inframammary fold toward the xiphoid process; the medial border ascends the midsternal line toward the suprasternal notch; and the upper border follows the clavicle before turning down toward the midaxilla. This pentagon can then be divided into four quadrants (Fig. 9-1). Most cancers originate in the upper outer quadrant of the breast, and also below the areola and nipple, two areas containing a large amount of glandular tissue. Always inspect first and palpate later.

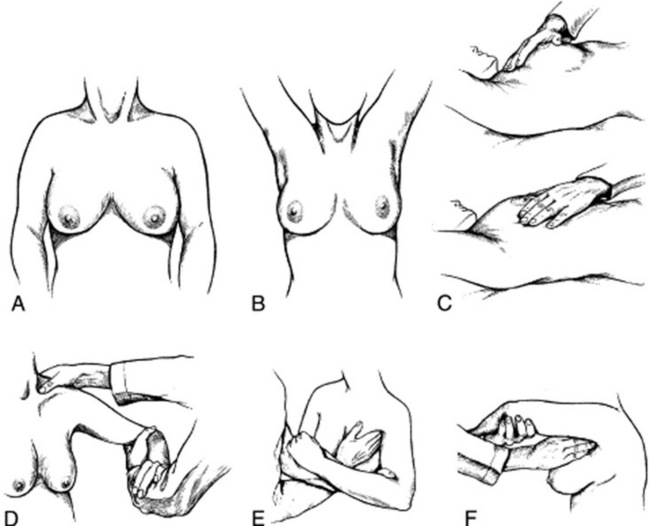
11 Which bedside maneuver can help to detect breast abnormalities on inspection?
The most commonly taught and used maneuvers include a change in position of the patient’s arms and hands, first described by Haagensen (Fig. 9-2). To do so, ask the patient to carry out the following sequence:
1. >Rest the hands on the lap (to relax the pectoralis muscles).
2. Press them over the hips (to tense the pectoralis muscles and make dimpling and retraction more visible).
3. Raise them above the head, clasping them behind it (to also trigger skin dimpling, an important harbinger of cancer).
4. Lean forward (to allow the breasts to hang out pendulous from the chest).



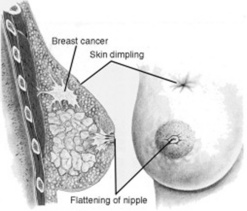
13 What is skin dimpling?
A slight depression or indentation in the breast’s surface (Fig. 9-3). This is an important clue to an underlying infiltrating carcinoma, causing fibrosis and retraction of the breast tissue. The same mechanism is responsible for nipple deviation.
21 What is meant by an adequate examination pattern?
Although two fifths of physicians may use no discernible pattern, proper technique is key for lesion detection. The two traditional methods are the radial spoke pattern and the concentric circles pattern (Fig. 9-4). However, the vertical strip pattern has been found to be more thorough. Begin your palpation in the axilla, and extend it in a straight line down the midaxillary line toward the bra line. Then move your fingers medially, continuing palpation up the chest, and in a straight line to the clavicle. Cover the entire breast, going up and down between the clavicle and bra line in a vertical strip pattern (or lawnmower technique). To cover all breast tissue, overlap rows.

22 Describe the correct finger position, movement, and pressure.




23 What are the final steps in the CBE?
Complete the exam by palpating for adenopathy in the supraclavicular and axillary fossae (Fig. 9-5). Then examine the nipple, through palpation and a squeeze. Although search for adenopathy is a routine component of the CBE, breast cancer is present in only 10–30% of women with isolated axillary lymphadenopathy and an otherwise normal CBE.

26 How should a breast lump (or nodule) be described?







27 What are the characteristics of malignant breast tissue?
A carcinomatous lesion is typically painless, irregular in contour and shape, hard in consistency, not mobile, and not well demarcated from the surrounding tissues. Retraction signs are usually a late phenomenon. A serous (or serosanguineous) nipple discharge can be an important sign of intraductal carcinomas (see questions 37–40).
32 What are the most common benign breast lesions?


34 What is the differential diagnosis of an inflammatory breast mass?


35 How can one separate acute mastitis from inflammatory breast carcinoma?


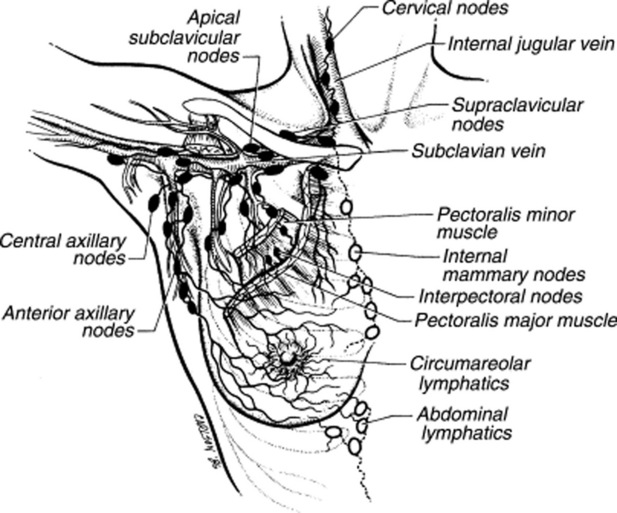
36 Describe the lymphatic drainage of the breasts.
 The superficial and central areas are drained by lymphatics that radiate from the areola and then converge toward the low/central axillary nodes and the subclavian nodes.
The superficial and central areas are drained by lymphatics that radiate from the areola and then converge toward the low/central axillary nodes and the subclavian nodes.

 Finally, other breast lymphatics drain into hepatic and subdiaphragmatic nodes (Fig. 9-6).
Finally, other breast lymphatics drain into hepatic and subdiaphragmatic nodes (Fig. 9-6).
B. Nipple Discharge
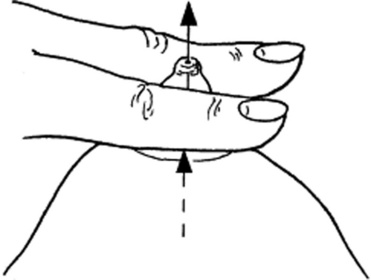
37 How do you assess for nipple discharge?
By applying gentle pressure at the base of the nipple, with the thumb and first or second finger (Fig. 9-7). Note that a discharge that occurs only with nipple compression/squeezing is usually physiologic. In a study of 448 women complaining of discharge, none of the 178 who had it only after expression was found to have cancer. Conversely, cancer was present in 2% (3/151) of those with spontaneous discharge but otherwise normal CBE.
C. Breast Self Examination (BSE)
1 Atkins H, Wolff B. Discharges from the nipple. Br J Surg. 1964;51:602-606.
2 Baines CJ, Wall C, Risch HA, et al. Changes in breast self-examination behaviour in a cohort of 8214 women in the Canadian National Breast Screening study. Cancer. 1986;57:1209-1216.
3 Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? JAMA. 1999;282:1270-1280.
4 Boyd NF, Sutherland HJ, Fish EB, et al. Physical examination of the breast. Am J Surg. 1981;142:307-426.
5 Chaudary MA, Millis RR, Davies GC, Hayward JL. Nipple discharge: The diagnostic value of testing for occult blood. Ann Surg. 1982;196:651-655.
6 De Gowin RL. Diagnostic Examination, 6th ed. New York: McGraw-Hill, 1994.
7 Egan RL, Goldstein GT, McSweeney MM, et al. Conventional mammography, physical examination, thermography, and xeroradiography in the detection of breast cancer. Cancer. 1997;39:1984-1992.
8 Fletcher SW, O’Malley MS, Bumce LA. Physicians’ abilities to detect lumps in silicone breast models. JAMA. 1985;253:2224-2228.
9 Gump FE. Sensitivity and specificity in silicone breast models. JAMA. 1985;254:2409.
10 Hicks MJ, Davis JR, Layton JM, Present AJ. Sensitivity of mammography and physical examination of the breast for detecting breast cancer. JAMA. 1979;242:2080-2083.
11 Mushlin AI. Diagnostic tests in breast cancer. Clinical strategies based on diagnostic probabilities. Ann Intern Med. 1985;103:79-85.
12 Newman HF, Klein M, Northrup JD, et al. Nipple discharge: Frequency and pathogenesis in an ambulatory population. N Y State J Med. 1983;83:928-933.
13 Nydick M, Bustos J, Dale JHJr, et al. Gynecomastia in adolescent boys. JAMA. 1961;178:449-454.
14 O’Malley MS, Fletcher SW. US Preventive Services Task Force. Screening for breast cancer with breast self-examination. A critical review. JAMA. 1987;257:2196-2203.


