TEMPOROMANDIBULAR JOINT
SELECTED MOVEMENTS


• To observe any asymmetries, the examiner must make sure the patient opens and closes the mouth slowly.
• Most clicking sensations occur during the second phase. Clicking is often an indication of the disc displacing as the condyle rolls and glides within the fossa.
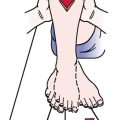
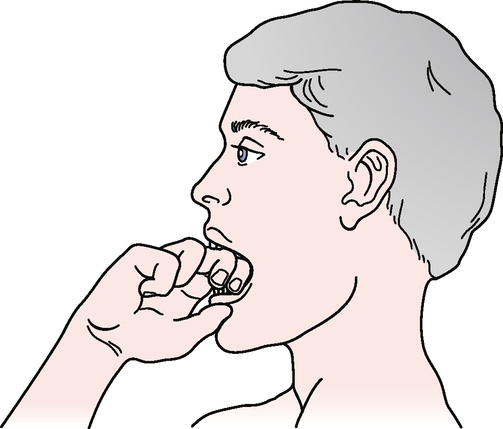
• The functional or full active opening is determined by having the patient try to place two or three flexed proximal interphalangeal joints within the mouth opening (see Functional Opening [Knuckle] Test later in the chapter).
• Normally, only about 25 to 35 mm of opening is needed for everyday activity.
• Kropmans et al.2 have pointed out that for treatment purposes, at least 6 mm of change is required for a detectable difference when more than one measurement is taken or to determine the effect of treatment.
Lateral Deviation or Excursion of the Mandible
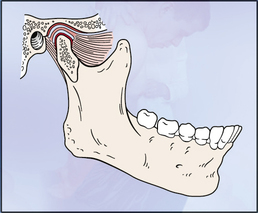
• During lateral deviation, the opposite condyle moves forward, down, and toward the motion side. The condyle on the motion side (i.e., left condyle on left lateral deviation) remains relatively stationary (rotating/spinning in place) and becomes more prominent.
• Any lateral deviation from the normal opening position or abnormal protrusion to one side indicates that the lateral pterygoid, masseter, or temporalis muscle; the disc; or the lateral ligament on the opposite side is affected.
FUNCTIONAL OPENING (KNUCKLE) TEST3–5 
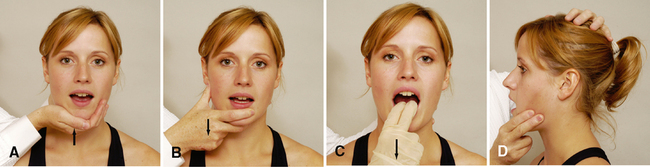
Closing of the mouth (elevation or occlusion). The examiner places one hand over the back of the head or neck to stabilize the head. The other hand is placed under the chin, with the patient’s mouth slightly open. A downward force is placed upon the chin as the patient resists this motion. The examiner may alternatively place a gloved hand over the teeth and provide the downward force to the teeth.
Lateral deviation of the jaw. The examiner places one hand over the side of the head above the temporomandibular joint to stabilize the head. The other hand is placed along the jaw of the patient’s slightly open. mouth, and the patient pushes out against it. Each side is tested individually.