Chapter 14 Technique for Harvesting a Mid-Third Patella Tendon Graft for Anterior Cruciate Ligament Reconstruction
Skin Incision
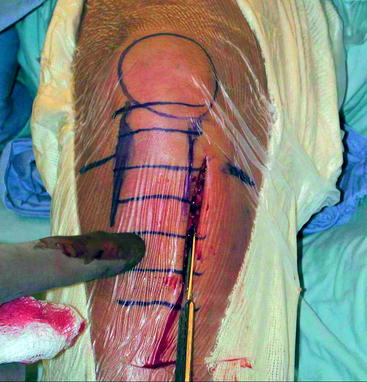
A vertical skin incision is made medial to the tibial tubercle approximately 0.5 cm medial to the medial edge of the patella tendon (Fig. 14-1). The upper end of the incision begins near the level of the joint line. The incision is extended distally to the level of the lower end of the tibial tubercle, approximately 6 to 8 cm below the joint line. Do not place this vertical incision in the midline of the knee: this leaves an unsightly scar, and it is difficult to reach the tibial tunnel from this midline position. This anteromedial incision is placed distally, which is necessary to allow positioning of the tibial guide and drilling of the tibial tunnel (Fig. 14-2). It is not necessary to extend the incision very far proximally beyond the level of the joint; when the knee is extended and a single spike retractor is placed at the superior pole of the patella, the patella is pushed distally. The patella can thus be reached through this short, distally placed incision.

Exposure
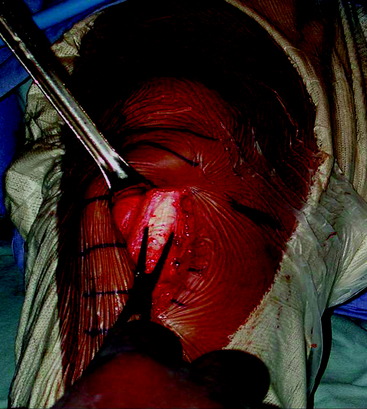
Incise the deep fascial layer lengthwise over the center of the underlying patella tendon. This deep fascial layer is thin but becomes even thinner over the tibial tubercle. Divide the deep fascial layer proximally to the level of the upper portion of the patella (Fig. 14-3). This exposes the underlying patella, patella tendon, and tibial tuberosity. Enlarge the prepatella bursa to gain access to the patella.
Taking the Graft
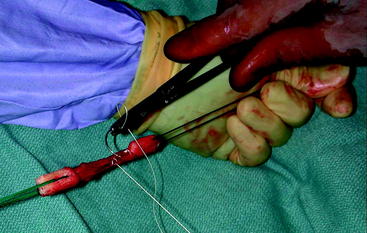
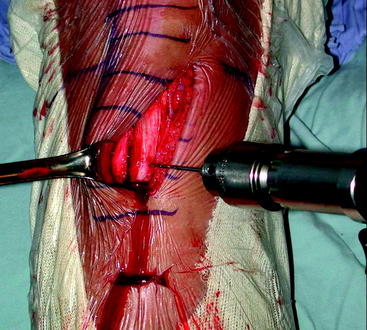
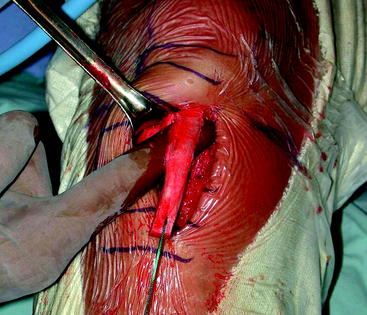
An osteotome 3 cm in length is used to make two parallel vertical cuts in the tibial tubercle to fashion a 9-cm-wide bone plug (Fig. 14-4). The ⅜-inch osteotome is used to make a transverse cut in the bone at the level of the distal end of the graft. The resulting bone plug is about 30 mm in length. Use the wide osteotome to extend the cuts in the tibial tubercle proximal to the tibial tubercle almost to the level of the joint; otherwise, the plug might crack proximally near the tendon-bone junction. Drill a single small hole in the distal end of the tibial bone plug, slightly less than 1 cm from the end of the tibial bone plug (Fig. 14-5). Pass a single suture of #5 Fiberwire through the tibial bone plug.

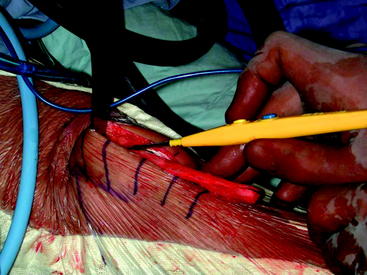
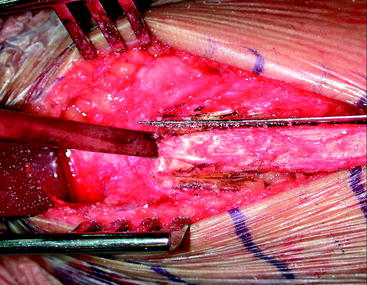
Apply traction to the tibial bone plug, and slightly incise the superficial surface of the patellar tendon in line with the tibial tubercle bone plug. Use your finger to separate the edges of the patella tendon graft from the adjacent patella tendon (Fig. 14-6). This blunt dissection avoids cutting fibers of the patella tendon graft.
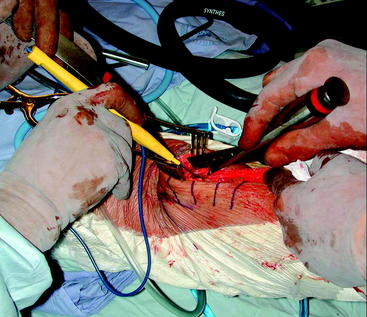
Insert a single spike retractor under the proximal edge of the skin incision. The prepatella bursa provides space to reach the superior pole of the patella. The spike of the retractor is set into the quadriceps tendon at the superior pole of the patella and is used to lever the patella distally (Fig. 14-7).
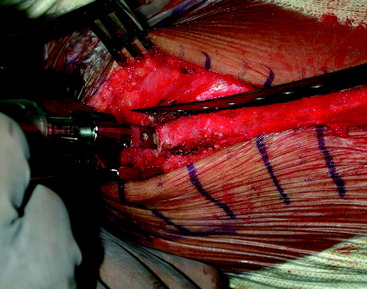
Using the cutting current of the cautery device, mark the line of the proposed first cut in the patella (see Fig. 14-7). Use a fine reciprocating saw to cut a slot in the patella for a length of about 25 mm and to a depth of 1 cm. Insert a metal ruler into this kerf (the cut made by a saw) and use it as a guide from which to measure. Using the ⅜-inch-wide osteotome as a template, mark the proposed cuts in the patella using electrocautery, which will achieve an 11-mm-wide plug that will be about 30 mm long (Fig. 14-8). Drill the corners of the graft to create round stress risers. Drill two small holes in the patella bone plug for later passage of sutures. Make the remaining cuts in the patella using the fine reciprocating saw to a depth of 1 cm (Fig. 14-9).
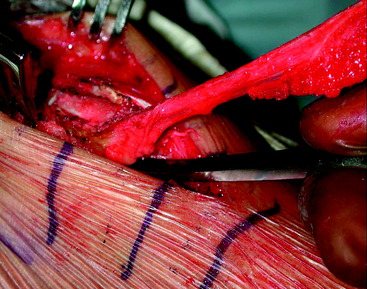
To loosen the bone plug from the patella, use a ¼-inch-wide curved osteotome inserted into the kerf at the superior end of the plug (Fig. 14-10). Never insert the osteotome into the medial or lateral kerfs along the edges of the patella bone plug, which will likely fracture the patella. Apply tension to the distal end of the graft, and use the ¼-inch-wide curved osteotome from below (starting at the inferior pole of the patella) to lift the patella bone plug from its bed (Fig. 14-11).
Fashioning the Graft
Use a bone cutter or rongeur to remove excess bone from both bone plugs to fashion a 9-mm-diameter bone plug from the tibial tubercle and an 11-mm-diameter bone plug from the patella (Fig. 14-12). Use a bone sizer to compress any excess cancellous bone. Do not use the bone sizer to compress cortical bone; doing so may fracture the patella. Place the extra pieces of bone into the defect in the patella. Close the deep fascial layer over the patella to prevent the bone pieces from falling out. Leave the edges of the patella tendon defect open for the time being.

At a side table, fashion the graft. To prevent dropping the graft, keep the suture that is attached to the graft wrapped around your little finger. Pass #5 Fiberwire sutures through each of the two holes and clamp the ends of the sutures. Use a 2–0 Vicryl running suture to tubularize the tendon at the end attached to the tibial bone plug (which will become the leading end of the graft) (Fig. 14-13). This will make it easier to place the interference screw into the femoral tunnel. Measure the total length of the graft and the lengths of the bone plugs. Use a colored marker pen to mark the bone-tendon junctions of the graft. Also mark the tendon side of the trailing end of the patella bone plug; this will aid in positioning the tibial interference screw on the opposite (cancellous) side of the plug (Fig. 14-14).