[level-membership-for-orthopaedics-category]
CHAPTER 7 Surgical Exposures of the Elbow
INTRODUCTION
It is not the purpose of this chapter to discuss all of the approaches to the joint but rather to provide a comprehensive collection and critique of those relevant exposures that should prove helpful to the practicing orthopedic surgeon.33
GENERAL PRINCIPLES
Rigorous adherence to the principles of good surgical technique is of no greater importance in any anatomic part than at the elbow.6,8,35 The most appropriate surgical approach depends on the specific goal of the surgical intervention and on the lesion. As for any orthopedic procedure, the choice of the surgical approach should be based on the following criteria (Box 7-1):
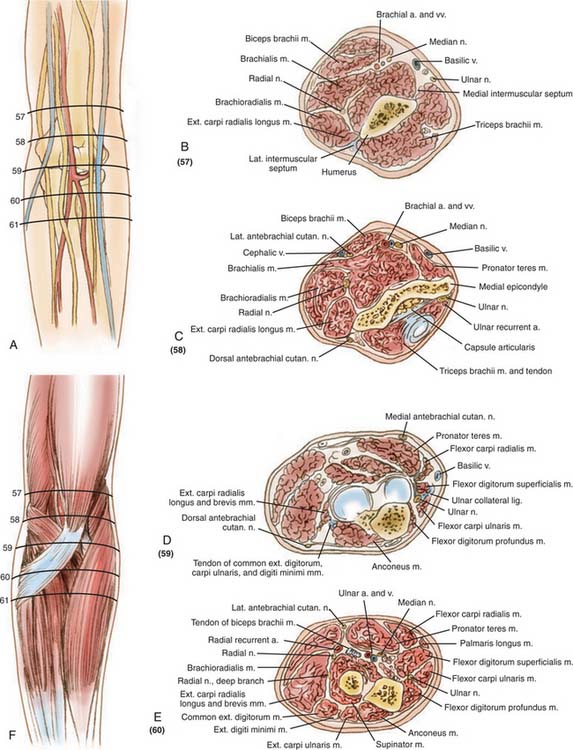
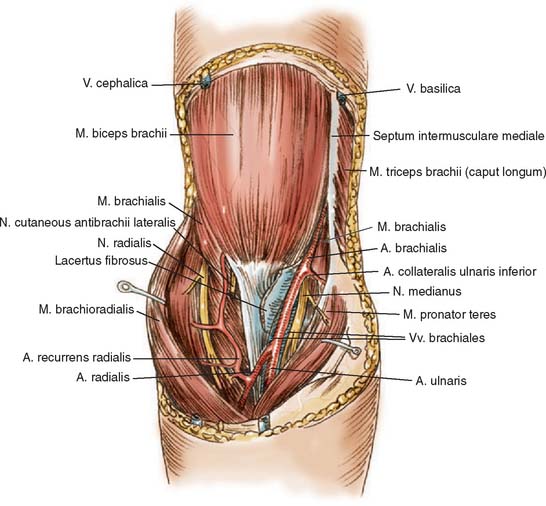
A thorough understanding of the anatomy of the elbow region and the relationship of the nerves and vessels is particularly important to selecting the exposure that best satisfies these requirements (Fig. 7-1).
LATERAL APPROACHES
A lateral exposure, probably the most commonly used approach to the elbow joint, offers many variations. It is used for radial head excision, removal of loose bodies, and repair of lateral ligaments, to fix condylar and Monteggia fractures, to release the joint capsule, and to remove osteophytes. Access to the radiohumeral articulation has been described by several authors.7,18,21,24,36 The techniques differ according to the muscle interval entered and the means of reflecting the muscle mass from the proximal ulna. With any of the lateral exposures to the joint or to the proximal radius, the surgeon must be constantly aware of the possibility of injury to the posterior interosseous or recurrent branch of the radial nerve.
Kaplan has described an approach through the interval between the extensor digitorum communis and the extensor carpi radialis longus and brevis muscles. Because of the proximity of the radial nerve, pronation of the forearm during exposure has been recommended to assist in carrying the radial nerve out of the surgical field. The effect of this maneuver has been quantified by Strachan and Ellis, who found that approximately 1 cm of mediolateral radial nerve translation can occur with forearm pronation (Fig. 7-2).42
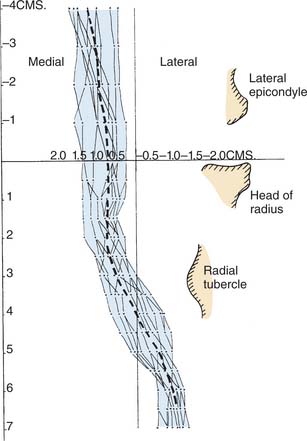
Even with this maneuver, however, the radial nerve is precariously close to the surgical field, so this approach is used less often than that described by Kocher. Knowledge of Kaplan’s interval24 is useful to expose the posterior interosseous nerve when decompression is performed in conjunction with tennis elbow release (see Chapter 44).41
THE KOCHER APPROACH AND ITS VARIATIONS
Some variation of the Kocher exposure is the most frequently used approach to the lateral aspect of the joint. This has the advantage of being extensile, affording a full complement of surgical options as the exposure is extended. This approach enters the joint through the interval of the anconeus and extensor carpi ulnaris, thus providing protection to the deep radial nerve. The interval is also anterior to the lateral ulnar collateral ligament, which reduces the likelihood of severing it at arthrotomy. In addition to providing a limited exposure for radial head excision and loose body removal, the particular value of this technique is that it may be converted to an extensile posterolateral approach to the entire distal humerus. If an extensile exposure is anticipated, a posterior incision is made. The same deep exposure can be accomplished by extending the posterior lateral skin incision and elevating the lateral skin cutaneous flap.
Limited Distal Lateral Approach: Kocher “J”
Landmarks
Lateral epicondyle, radial head, palpate interval between anconeus and extensor carpi ulnaris.
Skin Incision
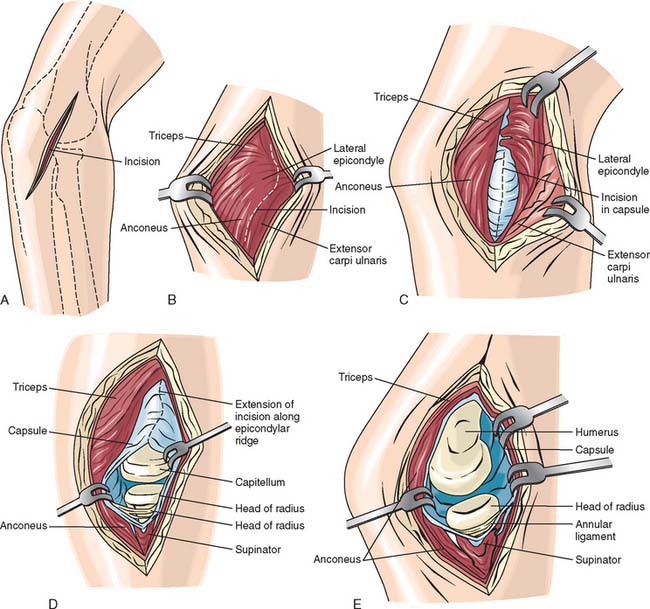
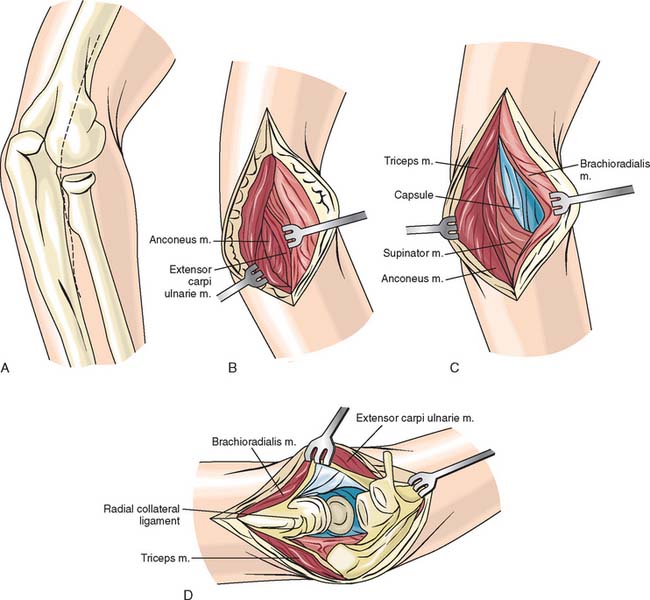
The skin incision is made from the subcutaneous border of the ulna obliquely across the posterolateral aspect of the elbow in line with Kocher’s interval and ends at or just proximal to the lateral epicondyle (Fig. 7-3A).
Interval
The interval between the anconeus and extensor carpi ulnaris is identified and entered (Fig. 7-3B). For excision of the radial head, the extensor carpi ulnaris and a small portion of the supinator muscle are dissected free of the capsule and retracted anteriorly (see Fig. 7-3C). The annular ligament is then identified and entered. Care should be taken to enter the annular ligament approximately 1 cm above the crista supinatoris to avoid injury to the lateral ulnar collateral ligament (see Fig. 7-3D).
Expanding the Distal Lateral Exposure
Indication
Reconstruction of the lateral ulnar collateral ligament, harvest anconeus for anconeus arthroplasty.31
Interval
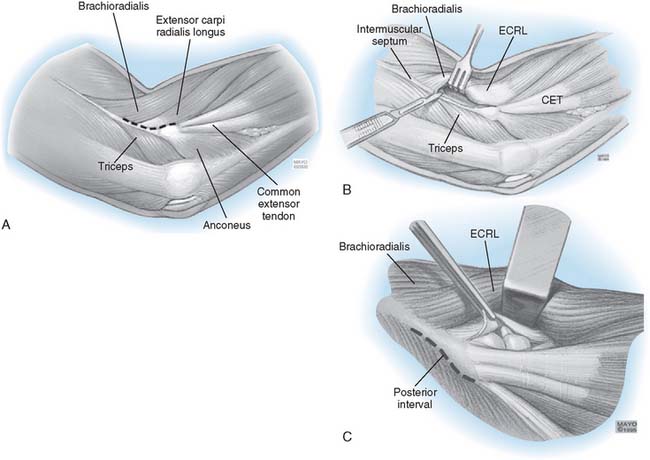
After the interval is entered, the anconeus is more completely reflected from its ulnar insertion (Fig. 7-4A). The lateral collateral ligament complex is identified by first elevating the extensor carpi ulnaris from the annular ligament just distal to the lateral epicondyle (see Fig. 7-4B). The fleshy attachment of the extensor carpi radialis longus is identified just above the common extensor tendon. This origin is freed from the supracondylar ridge. The dissection then elevates the common extensor tendon and the posterior edge of the extensor carpi radialis brevis from the lateral ligament complex (see Fig. 7-4D). This is done very carefully to identify and leave intact the lateral collateral ligament complex, and thus, reconstruction of the lateral ulnar collateral ligament can take place (see Chapter 48).
The Limited Proximal Lateral Exposure (Column Approach)
Skin Incision and Technique
This limited exposure of the anterior (and posterior) capsule has been described by Mansat and Morrey.28 The skin incision is over the lateral column, extending distally over the lateral epicondyle to the radial head (Fig. 7-5A). The extensor carpi radialis longus and distal fibers of the brachial radialis are elevated from the lateral column and epicondyle (see Fig. 7-5B). The brachialis muscle is separated from the anterior capsule, which can be safely performed if the joint has been entered at the radiocapitellar articulation. Since the arthrotomy provides accurate spatial orientation across the joint, damage to neurovascular structures is avoided. The procedure then continues as described in Chapter 44.
POSTEROLATERAL EXPOSURES
THE BOYD POSTEROLATERAL EXPOSURE7
Exposure of the lateral ulnohumeral and radiohumeral joint is accomplished with several variations of a posterolateral approach described by Boyd. Depending on the need to expose the proximal ulna or the distal humerus, these approaches can be extended and thus provide significant versatility.40
Skin Incision
Begin the incision just posterior to the lateral epicondyle and lateral to the triceps tendon, and continue the incision distally to the lateral tip of the olecranon and then down the subcutaneous border of the ulna to the junction of its proximal and middle thirds or as necessary in order to expose the fracture (Fig. 7-6A).
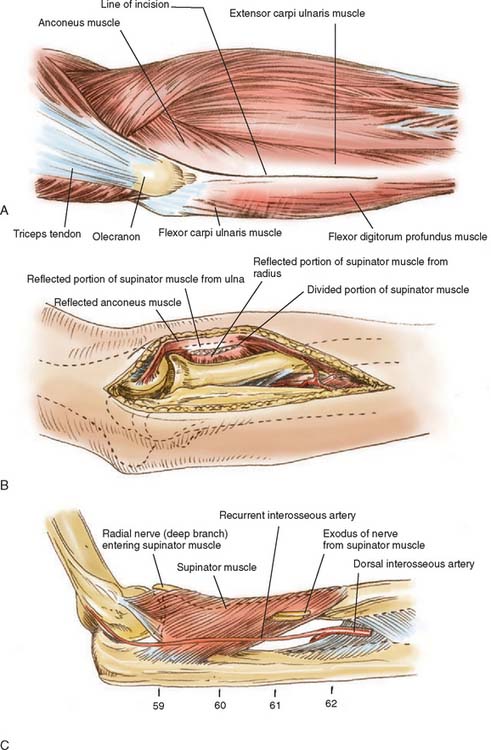
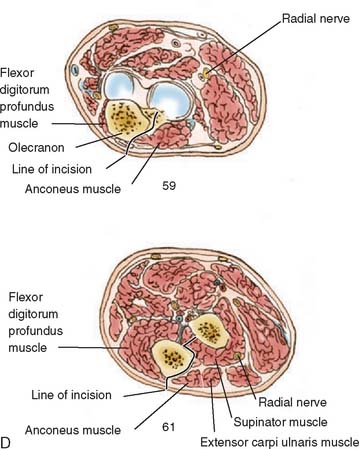
Technique
The anconeus and extensor carpi ulnaris are stripped subperiosteally from the ulna, beginning on the lateral subcutaneous crest of the bone and reflecting the muscles volarward. The supinator is released subperiosteally from its ulnar insertion, and the entire muscle mass is reflected anteriorly (see Fig. 7-6B). Be careful not to detach the ulnar attachment of the lateral ulnar collateral ligament. Thus, the lateral surface of the ulna and the proximal portion of the radius are adequately exposed (see Fig. 7-6C). The substance of the reflected supinator protects the deep branch of the radial nerve (see Fig. 7-6D). If greater exposure of the radius is desired, the recurrent interosseous artery (not the dorsal interosseous artery) is divided in the proximal portion of the wound, and the muscle mass is further reflected volarward to expose the interosseous membrane. The deep branch of the radial nerve remains protected.
EXTENSILE POSTEROLATERAL EXPOSURE (KOCHER)
This is an extension of the limited exposures described above involving the release of collateral ligament and capsule.24
Skin Incision and Technique
The triceps may be elevated from the posterior aspect of humerus by extending the skin incision proximally up the lateral column (Fig. 7-7A). This may proceed 6 to 7 cm proximal to the lateral epicondyle without fear of violence to the radial nerve.
Proceed as shown in Figure 7-7B by completely elevating the anconeus from the ulna. The triceps is easily elevated from the posterior humerus in the normal situation, and even in post-traumatic contractures, the triceps can be elevated with a periosteal elevator without much additional difficulty (see Fig. 7-7C). The lateral collateral ligament is released from the humeral origin as a separate structure or if prior surgery has caused scarring, with the common extensor tendon complex. The anterior capsule is then incised. A varus stress is applied to the elbow, which opens like a book hinging on the medial ulnar collateral ligament and common flexor muscles (see Fig. 7-7D). The triceps remains attached to the ulna.
MAYO MODIFIED KOCHER EXTENSILE POSTEROLATERAL EXPOSURE
Essential Characteristic
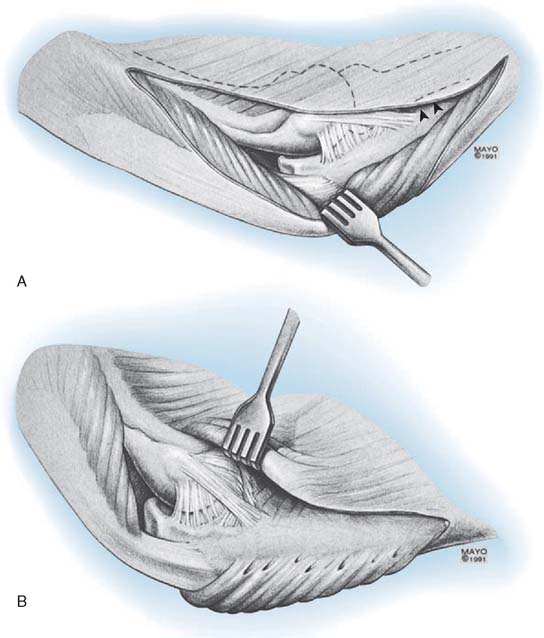
The triceps attachment is further released from the olecranon and the triceps mechanism is reflected from lateral to medial (Fig. 7-8A).
Technique
If more extensile exposure is required than has been obtained with the previous steps (see Figs. 7-5 and 7-6), a medial skin flap is elevated and the ulnar nerve identified. It is protected or translocated according to the merits of the case and after the release has proceeded according to the steps shown in Figure 7-6. The triceps and anconeus muscle sleeve is reflected from the tip of the olecranon by releasing Sharpey’s fibers (see Fig. 7-8A). The entire extensor mechanism including anconeus is thus reflected from lateral to medial (see Fig. 7-8B). After the triceps has been reflected and the posterior capsule released, the lateral collateral ligament may be detached from the humerus depending on the goal of the specific procedure and the additional exposure required. By flexing the elbow and removing the tip of the olecranon, the articular surface and the entire posterior humerus can be exposed.
POSTERIOR EXPOSURES
Extensile posterior exposure implies effective management of the triceps mechanism.5,37 In recent years, there has been a marked increased interest in revisiting and modifying previously described posterior surgical approaches.
Several skin incisions and techniques have been described. Although MacAusland27 used a transverse incision, most posterior skin incisions are longitudinal. The S incision of Ollier today is not as often used as the straighter incision recommended by Langenbeck.25 Probably the most important aspect of any incision is that it should not cross the tip of the olecranon. Smith also attributed better healing to a medial incision as compared with a lateral one.38
Releasing the triceps transverse section of the triceps mechanism at its musculotendinous junction has been described but does not afford adequate repair for optimal rehabilitation.46 Releasing the triceps at its attachment to the olecranon26 is not advisable, owing to the difficulty of adequate repair and possible disruption during rehabilitation.9 Today we categorize triceps management into four categories: (1) triceps splitting, (2) triceps reflecting, (3) triceps preserving, and (4) olecranon osteotomy (Fig. 7-9). A midline splitting incision was described as early as 1918 by James Thompson to expose the distal humerus for fractures, but it did not include release from the ulna to provide exposure of the joint itself.44
Splitting the triceps in line with the muscle fibers and at its insertion to expose the humerus and the elbow joint was described by Langenback25 and Campbell.10 This approach has had considerable resurgence of interest in recent years. When contracture is present, Campbell first separated the tendon from the muscle as an inverted V and then released the muscle fibers longitudinally. This technique, recommended later by Van Gorder46 for distal humerus fractures, allows lengthening of the musculotendinous unit, which may be necessary to fully mobilize the ankylosed joint. This triceps torque exposure has also faced a renewed interest and popularity in recent years.
POSTERIOR TRICEPS SPLITTING (CAMPBELL)10
Indications
Elbow arthroplasty,1 unreduced elbow dislocation, distal humeral fracture, posterior exposure of the joint for ankylosis, sepsis, synovectomy, and ulnohumeral arthroplasty.
Technique
The skin incision begins in the midline over the triceps, approximately 10 cm above the joint line, curves gently laterally or medially at the tip of the olecranon, and continues distally over the lateral aspect of the subcutaneous border of the proximal ulna for a distance of approximately 5 to 6 cm. If the incision is curved medially at the olecranon, the scar may have less tendency to contract.38
The triceps is exposed along with the proximal 6 cm of the ulna. A midline incision is made through the triceps, fascia, and tendon and is continued distally across the insertion of the triceps tendon at the tip of the olecranon and down the subcutaneous crest of the ulna (Fig. 7-10). The muscle is elevated medially and laterally exposing the distal humerus. Sharp dissection releases the triceps and the anconeus, which are reflected subperiosteally laterally. The insertion of the triceps is carefully released from the medial olecranon, leaving the flexor mechanism in continuity with the forearm fascia. The ulnar nerve is visualized and protected in the cubital tunnel. Only closure of the triceps fascia is required proximally, but the triceps insertion may be supplemented with a suture passed through the tip of the olecranon. The incision is then closed in layers.
TRICEPS SPLITTING, REFLECTION OF TRICEPS APONEUROSIS
Indications
Same as those for the midline-splitting approach described earlier, plus elbow contracture and unreduced elbow dislocations (see Chapter 30).10,47
Technique
The skin incision is begun 10 cm proximal to the olecranon and extends over the lateral aspect of the proximal ulna, ending 4 cm distal to the joint (Fig. 7-11). The triceps fascia and aponeurosis are isolated along with the tendinous insertion into the ulna. The aponeurosis is elevated and reflected from the muscle from proximal to distal, freeing the underlying muscle fibers while preserving the tendinous attachment to the olecranon. Proximally, the triceps muscle is then split in the midline, and the distal humerus is exposed subperiosteally. The dissection continues distally to the olecranon fossa, exposing the posterior aspect of the joint. If more extensive exposure is desired, the subperiosteal dissection is extended to the level of the joint, exposing the condyles both medially and laterally. The ulnar nerve should be identified and protected.
REFLECTION OF THE TRICEPS IN CONTINUITY
The triceps mechanism may be preserved in continuity and simply reflected to one side or the other. Three surgical approaches have been described that preserve the triceps muscle and tendon in continuity with the distal musculature and forearm fascia and expose the entire joint. These exposures were designed to allow rapid rehabilitation while limiting the risk of triceps disruption.
Mayo Modified Kocher’s Posterolateral, Extensile Triceps-Sparing Approach
This technique has been described earlier, along with the family of Kocher exposures (see Fig. 7-7).23
Mayo Triceps Reflection Technique of Bryan and Morrey
Indications
Ankylosis release, semiconstrained total elbow arthroplasty, ORIF medial column, distal humerus fractures.9
Skin Incision and Technique
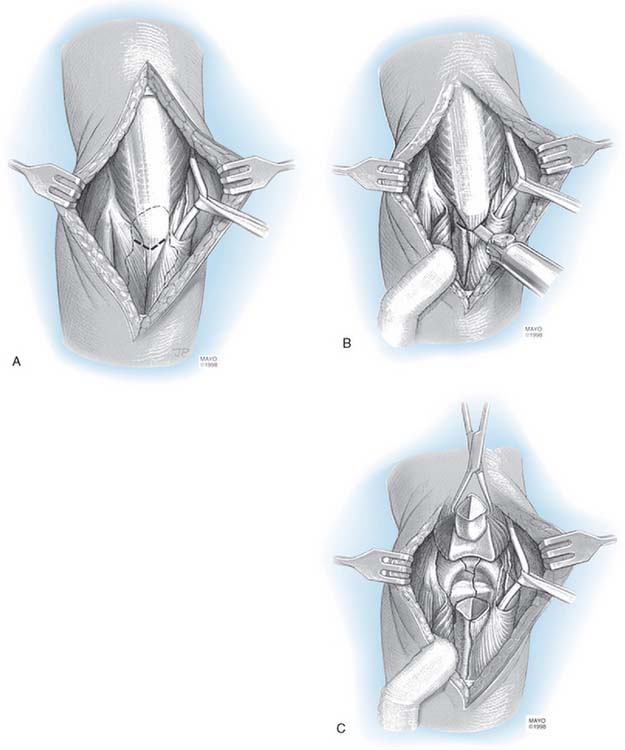
A 14-cm skin incision is made just medial to the tip of the olecranon. The dissection is carried to the medial aspect of the triceps 6 cm proximal and 4 cm distal to the tip of the olecranon. The ulnar nerve is identified, and if a femoral translocation is carried out, it is released from the margin of the triceps and elevated from its bed (Fig. 7-12A). The cubital tunnel retinaculum is split and the nerve released to the first motor branch. A subcutaneous pocket is developed, the intermuscular septum removed (see Fig. 7-12B), and the nerve is translocated anteriorly. The triceps is released from the entire posterior aspect of the distal humerus. Forearm fascia and ulna periosteum are elevated from the medial margin of the ulna. The Sharpey fiber attachment of the triceps to the olecranon is released by sharp dissection (see Fig. 7-12C). The distal forearm fascia and ulnar periosteum is elevated from the ulna. The lateral margin of the proximal ulna is then identified and the anconeus is elevated from its ulnar bed (see Fig. 7-12D). The extensor mechanism and capsule continues to be reflected from the margin of the lateral epicondyle (see Fig. 7-12E). If a medial column fracture has occurred, the tip of the olecranon is removed and the fracture may be addressed. For semiconstrained total elbow arthroplasty, the lateral and medial collateral ligaments are released and the extensor mechanism is reflected lateral to the epicondyle. The elbow is flexed and the tip of the olecranon is removed to expose the joint (see Fig. 7-12F).
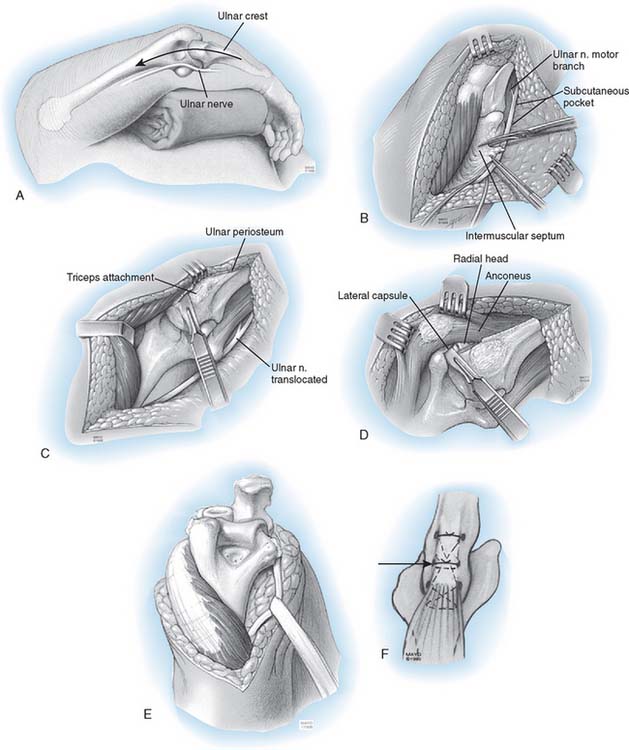
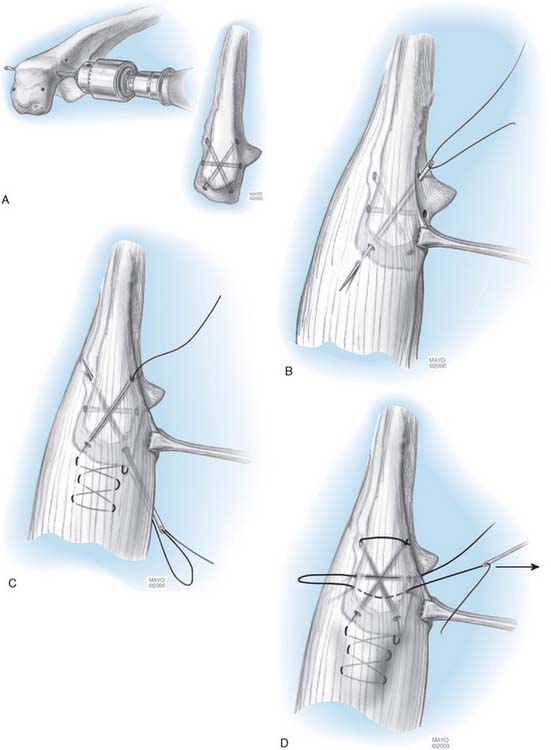
In every instance in which the triceps has been completely reflected either from lateral to medial (see Fig. 7-7) or medial to lateral (see Fig. 7-12), it is always securely reattached to the olecranon with a locked crisscross type of suture. Drill holes about 3 cm in length are placed in a cruciate fashion in the olecranon from proximal to distal (Fig. 7-13). A third transverse hole is drilled through the olecranon to secure a second stabilizing suture. The margin of the triceps is first grasped with an Allis clamp and brought over the olecranon. It is important to over correct the reattachment medially to ensure that the sleeve of tissue does not sublux laterally with flexion. A No. 5 nonabsorbable suture is introduced with a straight needle from distal to proximal for the modified Kocher and from distal medial to proximal lateral for the Mayo exposure. The suture is first brought through the osseous tunnel emerging at the tip of the olecranon and passes through the triceps tissue at its anatomic attachment site with the elbow flexed 70 degrees. The suture is locked at this site. It is then brought across the tendinous portion and locked medially. The suture then enters the medial hole in the olecranon and is passed from proximal medial to distal lateral. After the suture has emerged from the second hole in the olecranon, it is brought back over the top of the ulna through the soft tissue distal expansion of the extensor sleeve. Care is taken to leave the knot off to the side of the subcutaneous border of the ulna to avoid irritation or skin erosion. The second suture, which is very important to hold the triceps tendon securely applied to the olecranon attachment, is placed transversely across the ulna again beginning on the side from which the triceps reflection began. It is simply brought back across the triceps tendon in a transverse fashion and is locked in the midline to snugly stabilize the triceps insertion against the olecranon. All sutures are tied with the elbow in 70 to 90 degrees of flexion, again with the knots off the subcutaneous border.
OSTEOCUTANEOUS FLAP
One variation of the Mayo approach reflects the triceps with a sliver of bone while executing the same basic exposure philosophy.48
Triceps Release (Wolfe and Ranawat)
Technique
The triceps attachment is released from the ulna by osteotomizing the attachment with a thin wafer of bone that continues the attachment of the triceps tendon. This is the essential difference from the Mayo approach. The medial aspect of the triceps is elevated proximally, and the triceps attachment, with the wafer of bone, is elevated from the lateral aspect of the ulna in continuity with the anconeus muscle and the fascia (see Fig. 7-12).
Triceps-Preserving Technique
It is possible to elevate the triceps from the medial and lateral intramuscular septae while leaving the triceps attached to the olecranon.2,30
Several variations are included with this description.
Indications
Absence of distal humerus such as tumor resection, joint reconstruction for resection of humeral nonunion, or revision joint replacement.30
Technique
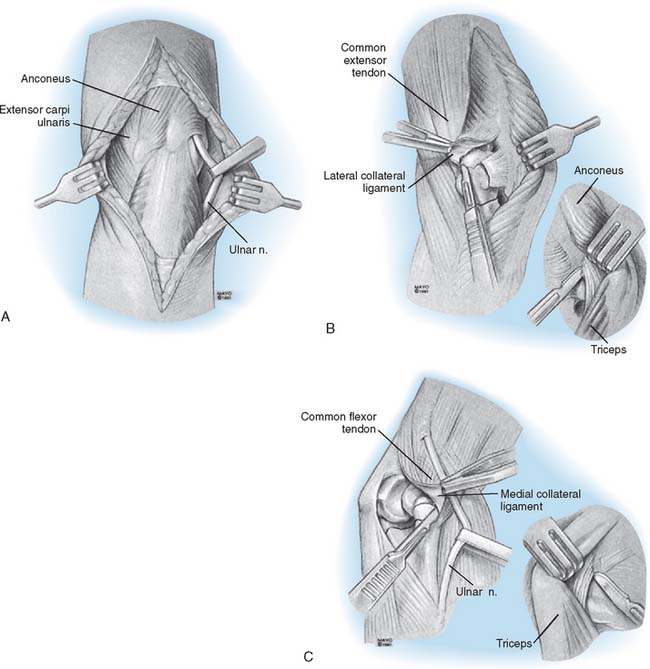
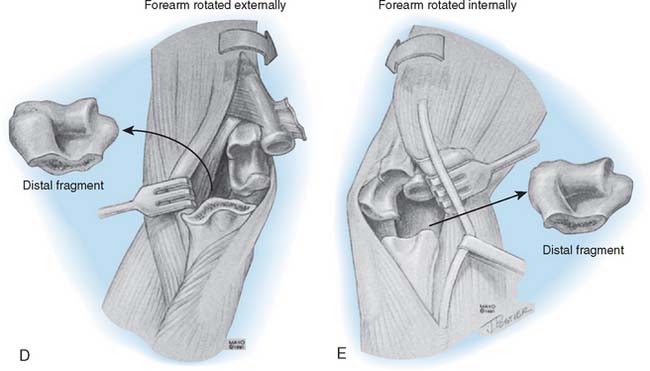
The technique is usually used for failed reconstructive procedures, so the previous skin incision is followed when possible. Otherwise, a posterior incision is made either medial or lateral to the tip of the olecranon. Medial and lateral skin flaps are elevated with as much subcutaneous tissue and fascia as possible. The medial and lateral aspects of the triceps are identified, and the ulnar nerve is isolated unless it was previously translocated anteriorly (Fig. 7-14A). The distal humeral nonunion or acute fracture fragments are sharply mobilized. The lateral collateral attachment to the humerus is severed, along with the common extensor tendon (see Fig. 7-14B). The common flexor tendon and muscle mass are elevated from the medial epicondyle along with the medial collateral ligament, and the distal segment is removed (see Fig. 7-14C). The distal aspect of the humerus usually is buttonholed laterally to the margin of the triceps (see Fig. 7-14D). Occasionally, the humerus is brought through the medial interval between the triceps muscle and the ulnar nerve. Regardless of the side to which the humerus is delivered, distal traction on the forearm must be avoided because it could stretch the ulnar nerve. The ulna is rotated appropriately to allow exposure to prepare and insert the ulnar component. At this point, a portion of the triceps attachment can be released to better expose the ulna (see Fig. 7-14E).
Comment
I have employed this exposure since 1989 in cases in which the distal humeral articulation is absent or resected. I have expanded the application, which was first used for nonunions29 to treat acute fractures and type IV rheumatoid arthritis. Because the triceps is not detached from its insertion at the tip of the olecranon, rapid rehabilitation is possible. It is expected that complete sparing of the triceps attachment will be used more frequently in the future and that the indications will increase. The most important caution is to avoid axial traction to the ulnar nerve from forearm manipulation.
POSTERIOR TRANSOSSEOUS EXPOSURES
OBLIQUE OSTEOTOMY
Technique
A 14-cm incision is made just lateral to the midline, extending past the tip of the olecranon. The insertion of the triceps tendon to the proximal ulna is carefully identified, and a 3.2-mm hole is drilled through the tip of the olecranon, centered down the medullary canal and on the insertion of the triceps tendon (Fig. 7-15). The triceps attachment is then carefully isolated and osteotomized in an oblique fashion with an oscillating saw. With its attachment to the osteotomized segment, the muscle is reflected proximally. At the completion of the procedure, the osteotomized fragment is reattached with a lag screw and the wound is closed in layers.
CHEVRON TRANSOLECRANON OSTEOTOMY
Indications
Ankylosed joints; T or Y condylar fracture.27
Comment
The intra-articular osteotomy first described by MacAusland was originally recommended for ankylosed joints. It has been adopted by some20 for radial head excision and synovectomy and used or modified by others12 for T and Y condylar fractures. However, in persons with rheumatoid arthritis, this portion of the bone may be thin, and therefore, this is not a suitable exposure for total elbow arthroplasty. The chevron design markedly enhances the repair and thus allows early motion.
Technique
Originally, a transverse incision across the elbow was described for the transverse osteotomy. At the present time, a straight incision is recommended (Fig. 7-16A). It is made posteriorly just lateral to the midline and measures approximately 14 cm centered on the olecranon. The ulnar nerve is isolated, dissected from the cubital tunnel, and protected. A 3.2-mm drill hole crosses the proposed osteotomy site for anatomic replacement at the completion of the procedure (see Fig. 7-16B). The joint is exposed at the midportion of the greater sigmoid notch. An apex distal chevron, or V, osteotomy initiated with the saw and completed with an osteotomy. By allowing the subchondral bone to “crack” facilitates accurate repositioning with the interdigitated surfaces. The capsular attachments, including the posterior portion of the ulnar collateral ligament, are released. The triceps tendon, along with the osteotomized portion of the olecranon, may then be retracted proximally, and by flexing the elbow joint, the tendon can be exposed (see Fig. 7-16C). Occasionally, the radial or medial collateral ligament may be released for better exposure, but it must later be reattached to the bone to avoid instability. At the completion of the procedure, the tip of the olecranon is secured with a single cancellous screw. The elbow usually is immobilized for 2 to 3 weeks, at which time a gentle, active rehabilitation program is instituted when clinically indicated.
COMBINED OSTEOTOMY PLUS TRICEPS SPLITTING
A recent report14 has suggested the value of combining the chevron osteotomy with a triceps-splitting technique. This would seem to offer little advantage over the chevron osteotomy as described with the associated triceps reflection techniques.
ANCONEUS SPARING OLECRANON OSTEOTOMY (MAYO TECHNIQUE)
Comment
Concern with regard to transecting the anconeus attachment to the triceps has prompted the development of an olecranon osteotomy that preserves the anconeus origin and viability. The attractiveness of this exposure is that the anconeus dissection can be done very safely and quickly. This does preserve the anconeus triceps continuity in the event that a later reconstructive procedure may be necessary that uses the anconeus.
TECHNIQUE
The patient is supine with the arm across the chest.28
The interval is entered and the anconeus is identified and isolated (Fig. 7-17A).
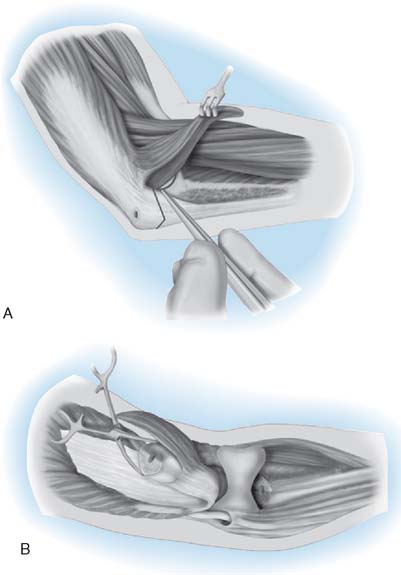
FIGURE 7-17 A, The anconeus interval is exposed through a mid-line incision of the distal forearm and extended laterally and distally over the anconeus. The muscle is elevated and the midportion of the lateral ulnohumeral joint identified. B, The medial ulnohumeral joint is entered as the ulnar nerve is protected, and a Chevron osteotomy as described in Figure 7-16 is completed. The olecranon and anconeus are reflected proximally.
The anconeus is elevated from its bed by sharp dissection leaving the attachment of its origin at the fascial expansion of the triceps; the mid portion of the sigmoid notch is identified laterally (see Fig. 7-17B).
Medially, the ulnar nerve is identified, and the midportion of the articulation is exposed (see Fig. 7-17C).
A V-shaped Chevron osteotomy is carried out as described earlier with an oscillating saw. The osteotomy is completed with an osteotome (see Fig. 7-17D).
The osteotomized olecranon, along with the attached anconeus, is elevated proximally.
Pitfalls
Avoid osteotomy in rheumatoid arthritis because the thin olecranon compromises healing if an osteotomy is carried out.31 The transverse osteotomy of McAusland is associated with an approximately 5% nonunion rate.31 Although for distal humeral fractures the Chevron osteotomy may improve these results and decrease the nonunion rate, I personally have not had the clinical need to osteotomize the olecranon in the last 14 years, and osteotomy should be avoided if the olecranon is resorbed.
MEDIAL APPROACHES
There are relatively few indications for medial exposure of the elbow joint, which has been superseded by arthroscopic approaches. The transcondylar approach described independently by Molesworth and Campbell provides excellent exposure of the joint, but it involves dissection of the ulnar nerve and healing of the osteotomized epicondyle, both of which increase the complexity, and thus limit the use, of this approach. In 1969, Taylor and Scham43 described a medial approach to the proximal ulna that was used for fractures in this region. The most valuable contribution to medial joint exposure is that described by Hotchkiss.21 This extensile exposure provides great flexibility, particularly for exposure of the coronoid and for contracture release.
TRANSEPICONDYLAR APPROACH
Indications
Medial epicondylar fractures, loose bodies, medial lesions whose symptoms require ulnar nerve exploration, and resurfacing arthroplasty.10,29
Technique
With the elbow flexed at 90 degrees, a medial incision is made from 5 cm above to approximately 5 cm below the elbow over the medial epicondyle. The ulnar nerve is identified, released, and retracted from the medial epicondyle, which is freed from soft tissue. It is helpful to make a longitudinal incision in the capsule just anterior to the ulnar collateral ligament and to place a periosteal elevator under the ligament as a landmark before performing the osteotomy. In this way, healing of the osteotomy restores the integrity of the ulnar collateral ligament. With a small osteotome, the epicondyle is freed and turned downward with its muscular attachments. Blunt dissection allows distal retraction of the flexor muscles, and careful technique avoids injury to the innervation of the muscle mass. The medial aspect of the coronoid process is exposed, along with the anterior and posterior capsules, which may be reflected from the humerus as necessary for additional exposure. Valgus stress hinges the joint on the lateral ligament and the remaining portions of the capsule, and provides generous exposure of virtually the entire elbow joint. Care must be taken to protect the median nerve as it passes over the anterior aspect of the joint. The epicondyle is returned to its anatomic position and secured with a small screw or with sutures placed through the bone. This step is important, because the quality of the repair affects the integrity of the ulnar collateral ligament, which is essential to the stability of the elbow joint.
EXTENSILE MEDIAL APPROACH (“OVER-THE-TOP” [HOTCHKISS])
Technique
The surface of the flexor pronator muscle mass origin is found by sweeping the subcutaneous tissue laterally with the medial antebrachial cutaneous nerve in this flap of subcutaneous tissue. The medial intermuscular septum is excised from the supracondylar ridge about 5 cm proximally (Fig. 7-18A). The ulnar nerve is protected, and the veins at the base of the septum are cauterized.
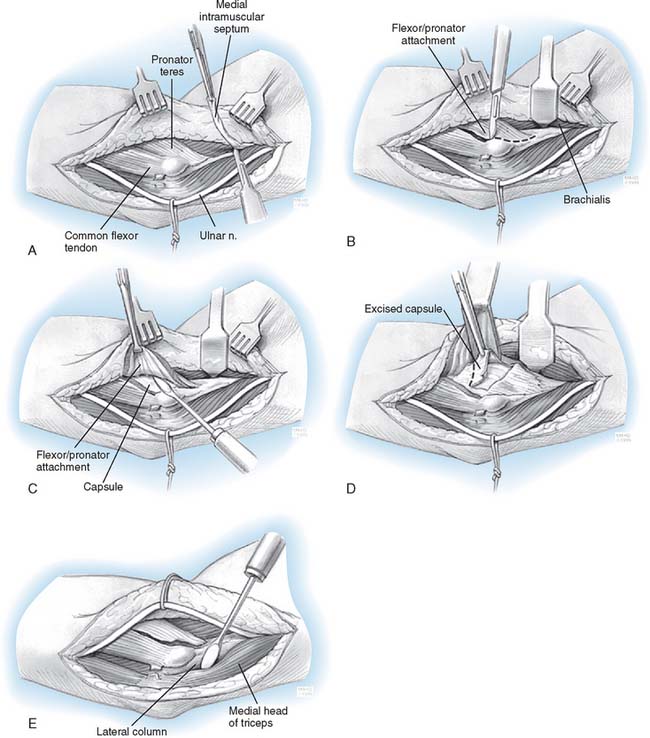
The supracondylar ridge is located, and elevation of the anterior muscle begins with a wide Cobb elevator. Subperiosteally, all of the anterior structures of the distal humeral region are elevated enough to allow placement of a wide Bennett retractor. The median nerve and brachial vein and artery are superficial to the brachialis muscle. Once the septum is excised, the flexor pronator muscle mass should be divided parallel to the fibers, leaving approximately a 1.5-cm span of flexor carpi ulnaris tendon attached to the epicondyle (see Fig. 7-18B). A small cuff of fibrous tissue of the origin can be left on the supracondylar ridge as the muscle is elevated. This facilitates reattachment when closing. A proximal, transverse incision in the lacertus fibrosus may also be needed to adequately mobilize this layer of muscle. The flexor pronator origin should be dissected down to the level of bone but superficial to the joint capsule. As this plane is developed, the brachialis muscle is encountered from the underside. This muscle should be kept anterior and elevated from the capsule and anterior surface of the distal humerus. Dissection of the capsule proceeds laterally and distally to separate it from the brachialis muscle (see Fig. 7-18C).
At this point, it is helpful to feel for the coronoid process by gently flexing and extending the elbow. A deep, narrow retractor is used and, after capsular excision, the radial head and capitellum can be visualized. In the case of contracture, the capsule, once separated from the overlying brachialis and brachioradialis, can be sharply excised (see Fig. 7-18D). The radial nerve is identified running between the brachialis and the brachioradialis. Care should be taken to stay deep to these two muscles when elevating over to the lateral side.
In a contracture release, the anteromedial portion of the capsule often requires release. To expose this area, a small narrow retractor can be inserted to pull the attached flexor carpi ulnaris medially. This affords adequate visualization and protection of the anteromedial collateral ligament.
The ulnar nerve is mobilized to permit anterior transposition with a dissection carried distally to the first motor branch to allow the nerve to rest in the anterior position without being sharply angled as it enters the flexor carpi ulnaris. With the Cobb elevator, the triceps is elevated from the posterior distal surface of the humerus (see Fig. 7-18E). The posterior capsule can be separated from the triceps as the elevator sweeps from proximal to distal.
ANTERIOR EXPOSURES
Because of the vulnerability of the brachial artery and median nerve, the anterior medial approach to the elbow is not recommended (Fig. 7-19). The extensile exposure described by Henry, as modified from Fiolle and Delmas, is the best known and the most useful for anterior exposure of the joint. Minor modifications of the Henry approach have been described,22,39 and a limited anterolateral exposure has been described by Darrach.14
Technique
The skin incision begins about 5 cm proximal and lateral to the flexor crease of the elbow joint and extends distally along the anterior margin of the brachioradialis muscle (Fig. 7-20A). Below the elbow joint, the incision turns medially to avoid crossing the flexor crease at a right angle, thus discouraging hypertrophic scar formation. The incision continues transversely to the biceps tendon and then turns distally over the medial volar aspect of the forearm, ending approximately 6 or 7 cm distal to the flexion crease. The interval between the brachioradialis laterally and the biceps and brachialis medially is identified and entered. The fascia is released distally between the brachioradialis and the pronator teres (see Fig. 7-20B).
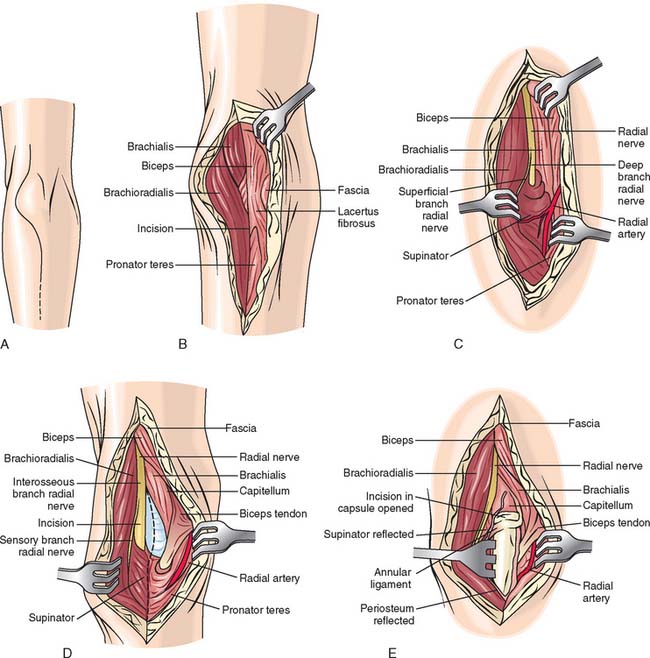
The interval then is entered proximally, and gentle, blunt dissection demonstrates the radial nerve coursing on the inner surface of the brachioradialis muscle. Care is taken to avoid injuring the superficial sensory branch of the radial nerve. Because the radial nerve gives off its branches laterally, it can safely be retracted with the brachioradialis muscle. At the level of the elbow joint, as the brachioradialis is retracted laterally and the pronator is gently retracted medially, the radial artery can be observed where it emerges from the medial aspect of the biceps tendon, giving off its muscular and recurrent branches in a mediolateral direction (see Fig. 7-20C). The muscle branch is ligated, but the recurrent radial artery should be sacrificed only if the lesion warrants the more extensive exposure that can be realized with this maneuver.
If more distal exposure is needed, the forearm is fully supinated, demonstrating the insertion of the supinator muscle on the proximal radius. This insertion is incised, and the supinator is subperiosteally retracted laterally (see Fig. 7-20D). The supinator serves as protection to the deep interosseous branch of the radial nerve, but excessive retraction of the muscle should be avoided. The proximal aspect of the radius and the capitellum are thus exposed. Additional visualization may be obtained both proximally and distally, because the radial nerve has been identified and can be avoided proximally. The posterior interosseous nerve is protected distally by the supinator muscle, and the radial artery is visualized and protected medially if a more extensile exposure is required (see Fig. 7-20E).
RESULTS
There have been limited attempts to document the efficacy of one or the other of the various types of triceps-sparing approaches. In the original description, we compared the clinical result of the Mayo approach to that of the triceps splitting or transverse release of the triceps reattachment.9 There were no triceps disruptions after approximately 75 procedures done with the triceps being released in continuity (Mayo approach) compared with an approximately 20% complication rate when the triceps was released transversely. Wolfe and Ranawat48 have also observed no instances of triceps insufficiency with their modification of this approach. The use of the Mayo medial exposure was also shown to have improved triceps strength after total elbow arthroplasty.32 This manner of exposing the elbow was found to be associated with approximately 20% greater extension strength than with the Campbell (Van Gorder) type of exposure.
An additional consideration in those with rheumatoid arthritis is the thin olecranon that compromises healing if an osteotomy is carried out.20 The transverse osteotomy of McAusland is associated with an approximately 5% nonunion rate.31 Although for fractures the chevron osteotomy may improve these results and decrease the nonunion rate, I personally have not had the clinical need for osteotomized the olecranon in the last 20 years and this should be avoided if the olecranon has been thinned.
COMPLICATIONS
WOUND HEALING
Difficult ankylosis release procedures are associated with a significant amount of swelling as often occurs in patients undergoing total elbow arthroplasty. Wound healing is generally not a problem, however, and is related to the presence of prior incisions and the magnitude of the dissection as is typical for release of the stiff elbow.
INFECTION
The infection rate after total elbow arthroplasty has been reduced at our institution from a high of 11% in 1970 to approximately 3% over the last 10 years.32 This reduction is coincident with adopting the Mayo approach to the elbow but other technique changes have occurred in this period, including using antibiotic-impregnated cement and splinting the elbow in extension.
ULNAR NERVE INJURY
Injury to the ulnar nerve appears to be more common in those instances in which the ulnar nerve is not exposed and the elbow is flexed on the medial collateral ligament such as with the classic extensile Kocher approach.16,45 Simply exposing the ulnar nerve, while decreasing this complication, does not completely obviate it. The theoretical disadvantage of the Mayo approach, which allows translocation of the ulnar nerve, is that this maneuver devascularizes the nerve, and the dissection itself may cause ulnar nerve irritation. Having used this particular exposure in more than 500 cases, the incidence of permanent ulnar nerve injury with motor dysfunction is less than 1%. Therefore, I am comfortable in exposing and moving the ulnar nerve in a subcutaneous pocket as an essential and integral part of the Mayo triceps-sparing approach.
RADIAL NERVE INJURY
Although posterior interosseous nerve palsy is known to occur with some approaches to the radial nerve,21 the complication is virtually unheard of when the joint is exposed through Kocher’s interval.
TRICEPS DISRUPTION
Triceps disruption is uncommon in our experience with either the Mayo modified extensile Kocher exposure or the Mayo medial to lateral type of approach. The incidence of triceps disruption is less than 1% in our experience. If, however, the triceps should become disrupted after either of the procedures described above, if adequate tissue is present, it may be reattached as described for the primary procedure. If the remaining tissue is inadequate, triceps power is restored either by an anconeus slide or achilles tendon allograft reconstruction (see Chapter 35).
1 Albee F.H. Arthroplasty of the elbow. J. Bone Joint Surg. 1933;15:979.
2 AlonsoLlames M. Bilaterotricipital approach to the elbow. Acta Orthop. Scand. 1972;42:479.
3 Anson B.J., Maddock W.G. Callander’s Surgical Anatomy, 4th ed. Philadelphia: W. B. Saunders Co., 1958.
4 Banks S.W., Laufman H. An Atlas of Surgical Exposures of the Extremities. Philadelphia: W. B. Saunders Co., 1953.
5 Boorman R.S., Page W.T., Weldon E.J., Lippitt S., Matsen F.A.III. A triceps-on approach to semi-constrained total elbow arthroplasty. Techniques in Shoulder & Elbow Surgery. 2003;4:139.
6 Bost F.C., Schottstaedt E.R., Larsen L., Abbott L.. Surgical approaches to the elbow joint. American Academy of Orthopaedic Surgeons: Instructional Course Lectures, Vol. 10. J. W. Edwards, Ann Arbor, 1953;180.
7 Boyd H.B. Surgical exposure of the ulna and proximal third of the radius through one incision. Surg. Gynecol. Obstet. 1940;71:86.
8 Boyd H.B. Surgical approaches to the elbow joint. Instruct. Course Lect. 1947;4:147.
9 Bryan R.S., Morrey B.F. Extensive posterior exposure of the elbow: a triceps sparing approach. Clin. Orthop. 1982;166:188.
10 Campbell W.C. Incision for exposure of the elbow joint. Am. J. Surg. 1932;15:65.
11 Campbell W.C., Edmonson A.S., Crenshaw A.H., editors. Campbell’s Operative Orthopedics, 5th ed.. Surgical Approaches, Vol. I. C. V. Mosby Co., St. Louis, 1971;119.
12 Casselbaum W.H. Operative treatment of T and Y fractures of the lower end of the humerus. Am. J. Surg. 1952;83:265.
13 Crenshaw A.H. Surgical approaches. In Edmonson A.S., Crenshaw A.H., editors: Campbell’s Operative Orthopaedics, 6th ed., St. Louis: C. V. Mosby, 1980.
14 Darrach W. Surgical approaches for surgery of the extremities. Am. J. Surg. 1945;67:93.
15 Ebraheim N.A., Andreshak T.G., Yeasting R.A., Saunders R.C., Jackson W.T. Posterior extensile approach to the elbow joint and distal humerus. Orthop. Rev. 1993;22:578.
16 Ewald F.C., Jacobs M.A. Total elbow arthroplasty. Clin. Orthop. 1984;182:137.
17 Eycleshymer A.C., Schoemaker D.M. A Cross Section Anatomy. New York: D. Appleton and Co., 1930.
18 Gordon M.L. Monteggia fracture. A combined surgical approach employing a single lateral incision. Clin. Orthop. 1967;50:87.
19 Henry A.K. Extensile Exposure, 2nd ed. Baltimore: Williams & Wilkins Co., 1957.
20 Inglis A.E., Ranawat C.S., Straub L.R. Synovectomy and debridement of the elbow in rheumatoid arthritis. J. Bone Joint Surg. 1971;53A:652.
21 Kaplan E.B. Surgical approaches to the proximal end of the radius and its use in fractures of the head and neck of the radius. J. Bone Joint Surg. 1941;23:86.
22 Kasparyan N.G., Hotchkiss R.N. Dynamic skeletal fixation in the upper extremity. Hand Clin. 1997;13:643.
23 Kelly R.P., Griffin T.W. Open reduction of T condylar fractures of the humerus through an anterior approach. J. Trauma. 1969;9:901.
24 Kocher T. Textbook of Operative Surgery, 3rd ed. London: A. and C. Black, 1911.
25 Langenbeck M. Bilaterotricipital approach to the elbow. Acta Orthop. Scand. 1972;43:479. (1864): Cited by Alonso Llames
26 Lexer B. Cited by Alonso Llames, M.: Bilaterotricipital approach to the elbow. Acta Orthop. Scand.. 1972;43:479.
27 MacAusland W.R. Ankylosis of the elbow: with report of four cases treated by arthroplasty. J. A. M. A. 1915;64:312.
28 Mansat P., Morrey B.F. The column procedure: a limited lateral approach for extrinsic contracture of the elbow. J. Bone Joint Surg. 1998;80A:1603.
29 Molesworth W.H.L. Operation for complete exposure of the elbow joint. Br. J. Surg. 1930;18:303.
30 Morrey B.F. Revision total elbow arthroplasty. In: Morrey B.F., editor. Joint Replacement Arthroplasty. New York: Churchill Livingstone; 1991:345-360.
31 Morrey B.F. Surgical exposures of the elbow. In: Morrey B.F., editor. The Elbow and Its Disorders. 3rd ed. Philadelphia: W. B. Saunders Co.; 2000:109.
32 Morrey B.F., Askew L.J., An K.N. Strength function after elbow arthroplasty. Clin. Orthop. 1988;234:43.
33 Morrey B.F., Morrey M.C. Relevant surgical exposures. In Master’s Techniques in Orthopedic Surgery. Philadelphia: Lippincott, Williams & Wilkins; 2008.
34 Muller M.E., Allgower M., Willenegger H. Manual of Internal Fixation: Technique Recommended by the AO Group. New York: Springer-Verlag, 1970.
35 Ogilvie W.H. Discussion of minor injuries of the elbow joint. Proc. Roy. Soc. Med. 1929;23:306.
36 Pankovich A.M. Anconeus approach to the elbow joint and the proximal part of the radius and ulna. J. Bone Joint Surg. 1977;59A:124.
37 Schildhauer T.A., Nork S.E., Mills W.J., Henley M.B. Extensor mechanism-sparing paratricipital posterior approach to the distal humerus. J. Orthop. Trauma. 2003;17:374.
38 Smith F.M. Surgery of the Elbow, 2nd ed. Philadelphia: W. B. Saunders Co., 1972.
39 Sorrell E., Longuet Y.J. La voie transbrachiale anterieure dans la chirurgie des fractures supracondyliennes de l’humerus chez l’enfant. Rev. Orthop. 1946;32:117.
40 Speed J.S., Boyd H.B. Treatment of fractures of ulna with dislocation of head of radius (Monteggia fracture). J.A.M.A. 1940;115:1699.
41 The radial nerve. In: Spinner M., editor. Injuries to the Major Branches of Peripheral Nerves of the Forearm. 2nd ed. Philadelphia: WB Saunders; 1978:85-91.
42 Strachan J.H., Ellis B.W. Vulnerability of the posterior interosseous nerve during radial head reaction. J. Bone Joint Surg. 1971;53B:320.
43 Taylor T.K.F., Scham S.M. A posteromedial approach to the proximal end of the ulna for the internal fixation of olecranon fractures. J. Trauma. 1969;9:594.
44 Thompson J.E. Anatomical methods of approach in operations on the long bones of the extremities. Ann. Surg. 1918;68:309.
45 Trancik T., Wilde A.H., Borden L.S. Capitellocondylar elbow arthroplasty. Two to eight year experience. Clin. Orthop. 1987;112:175.
46 Van Gorder G.W. Surgical approach in old posterior dislocation of the elbow. J. Bone Joint Surg. 1932;14:127.
47 Van Gorder G.W. Surgical approach in supracondylar “T” fractures of the humerus requiring open reduction. J. Bone Joint Surg. 1940;22:278.
48 Wolfe S.W., Ranawat C.S. The osteoanconeus flap: an approach for total elbow arthroplasty. J. Bone Joint Surg. 1990;72A:684.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
CHAPTER 7 Surgical Exposures of the Elbow
INTRODUCTION
It is not the purpose of this chapter to discuss all of the approaches to the joint but rather to provide a comprehensive collection and critique of those relevant exposures that should prove helpful to the practicing orthopedic surgeon.33
GENERAL PRINCIPLES
Rigorous adherence to the principles of good surgical technique is of no greater importance in any anatomic part than at the elbow.6,8,35 The most appropriate surgical approach depends on the specific goal of the surgical intervention and on the lesion. As for any orthopedic procedure, the choice of the surgical approach should be based on the following criteria (Box 7-1):
A thorough understanding of the anatomy of the elbow region and the relationship of the nerves and vessels is particularly important to selecting the exposure that best satisfies these requirements (Fig. 7-1).
LATERAL APPROACHES
A lateral exposure, probably the most commonly used approach to the elbow joint, offers many variations. It is used for radial head excision, removal of loose bodies, and repair of lateral ligaments, to fix condylar and Monteggia fractures, to release the joint capsule, and to remove osteophytes. Access to the radiohumeral articulation has been described by several authors.7,18,21,24,36 The techniques differ according to the muscle interval entered and the means of reflecting the muscle mass from the proximal ulna. With any of the lateral exposures to the joint or to the proximal radius, the surgeon must be constantly aware of the possibility of injury to the posterior interosseous or recurrent branch of the radial nerve.
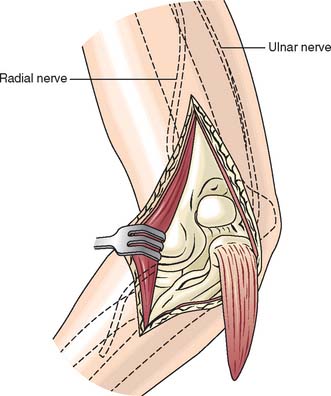
Kaplan has described an approach through the interval between the extensor digitorum communis and the extensor carpi radialis longus and brevis muscles. Because of the proximity of the radial nerve, pronation of the forearm during exposure has been recommended to assist in carrying the radial nerve out of the surgical field. The effect of this maneuver has been quantified by Strachan and Ellis, who found that approximately 1 cm of mediolateral radial nerve translation can occur with forearm pronation (Fig. 7-2).42
Even with this maneuver, however, the radial nerve is precariously close to the surgical field, so this approach is used less often than that described by Kocher. Knowledge of Kaplan’s interval24 is useful to expose the posterior interosseous nerve when decompression is performed in conjunction with tennis elbow release (see Chapter 44).41
THE KOCHER APPROACH AND ITS VARIATIONS
Some variation of the Kocher exposure is the most frequently used approach to the lateral aspect of the joint. This has the advantage of being extensile, affording a full complement of surgical options as the exposure is extended. This approach enters the joint through the interval of the anconeus and extensor carpi ulnaris, thus providing protection to the deep radial nerve. The interval is also anterior to the lateral ulnar collateral ligament, which reduces the likelihood of severing it at arthrotomy. In addition to providing a limited exposure for radial head excision and loose body removal, the particular value of this technique is that it may be converted to an extensile posterolateral approach to the entire distal humerus. If an extensile exposure is anticipated, a posterior incision is made. The same deep exposure can be accomplished by extending the posterior lateral skin incision and elevating the lateral skin cutaneous flap.
Limited Distal Lateral Approach: Kocher “J”
Landmarks
Lateral epicondyle, radial head, palpate interval between anconeus and extensor carpi ulnaris.
Skin Incision
The skin incision is made from the subcutaneous border of the ulna obliquely across the posterolateral aspect of the elbow in line with Kocher’s interval and ends at or just proximal to the lateral epicondyle (Fig. 7-3A).
Interval
The interval between the anconeus and extensor carpi ulnaris is identified and entered (Fig. 7-3B). For excision of the radial head, the extensor carpi ulnaris and a small portion of the supinator muscle are dissected free of the capsule and retracted anteriorly (see Fig. 7-3C). The annular ligament is then identified and entered. Care should be taken to enter the annular ligament approximately 1 cm above the crista supinatoris to avoid injury to the lateral ulnar collateral ligament (see Fig. 7-3D).
Expanding the Distal Lateral Exposure
Indication
Reconstruction of the lateral ulnar collateral ligament, harvest anconeus for anconeus arthroplasty.31
Interval
After the interval is entered, the anconeus is more completely reflected from its ulnar insertion (Fig. 7-4A). The lateral collateral ligament complex is identified by first elevating the extensor carpi ulnaris from the annular ligament just distal to the lateral epicondyle (see Fig. 7-4B). The fleshy attachment of the extensor carpi radialis longus is identified just above the common extensor tendon. This origin is freed from the supracondylar ridge. The dissection then elevates the common extensor tendon and the posterior edge of the extensor carpi radialis brevis from the lateral ligament complex (see Fig. 7-4D). This is done very carefully to identify and leave intact the lateral collateral ligament complex, and thus, reconstruction of the lateral ulnar collateral ligament can take place (see Chapter 48).
The Limited Proximal Lateral Exposure (Column Approach)
Skin Incision and Technique
This limited exposure of the anterior (and posterior) capsule has been described by Mansat and Morrey.28 The skin incision is over the lateral column, extending distally over the lateral epicondyle to the radial head (Fig. 7-5A). The extensor carpi radialis longus and distal fibers of the brachial radialis are elevated from the lateral column and epicondyle (see Fig. 7-5B). The brachialis muscle is separated from the anterior capsule, which can be safely performed if the joint has been entered at the radiocapitellar articulation. Since the arthrotomy provides accurate spatial orientation across the joint, damage to neurovascular structures is avoided. The procedure then continues as described in Chapter 44.
POSTEROLATERAL EXPOSURES
THE BOYD POSTEROLATERAL EXPOSURE7
Exposure of the lateral ulnohumeral and radiohumeral joint is accomplished with several variations of a posterolateral approach described by Boyd. Depending on the need to expose the proximal ulna or the distal humerus, these approaches can be extended and thus provide significant versatility.40
Skin Incision
Begin the incision just posterior to the lateral epicondyle and lateral to the triceps tendon, and continue the incision distally to the lateral tip of the olecranon and then down the subcutaneous border of the ulna to the junction of its proximal and middle thirds or as necessary in order to expose the fracture (Fig. 7-6A).
Technique
The anconeus and extensor carpi ulnaris are stripped subperiosteally from the ulna, beginning on the lateral subcutaneous crest of the bone and reflecting the muscles volarward. The supinator is released subperiosteally from its ulnar insertion, and the entire muscle mass is reflected anteriorly (see Fig. 7-6B). Be careful not to detach the ulnar attachment of the lateral ulnar collateral ligament. Thus, the lateral surface of the ulna and the proximal portion of the radius are adequately exposed (see Fig. 7-6C). The substance of the reflected supinator protects the deep branch of the radial nerve (see Fig. 7-6D). If greater exposure of the radius is desired, the recurrent interosseous artery (not the dorsal interosseous artery) is divided in the proximal portion of the wound, and the muscle mass is further reflected volarward to expose the interosseous membrane. The deep branch of the radial nerve remains protected.
EXTENSILE POSTEROLATERAL EXPOSURE (KOCHER)
This is an extension of the limited exposures described above involving the release of collateral ligament and capsule.24
Skin Incision and Technique
The triceps may be elevated from the posterior aspect of humerus by extending the skin incision proximally up the lateral column (Fig. 7-7A). This may proceed 6 to 7 cm proximal to the lateral epicondyle without fear of violence to the radial nerve.
Proceed as shown in Figure 7-7B by completely elevating the anconeus from the ulna. The triceps is easily elevated from the posterior humerus in the normal situation, and even in post-traumatic contractures, the triceps can be elevated with a periosteal elevator without much additional difficulty (see Fig. 7-7C). The lateral collateral ligament is released from the humeral origin as a separate structure or if prior surgery has caused scarring, with the common extensor tendon complex. The anterior capsule is then incised. A varus stress is applied to the elbow, which opens like a book hinging on the medial ulnar collateral ligament and common flexor muscles (see Fig. 7-7D). The triceps remains attached to the ulna.
MAYO MODIFIED KOCHER EXTENSILE POSTEROLATERAL EXPOSURE
Essential Characteristic
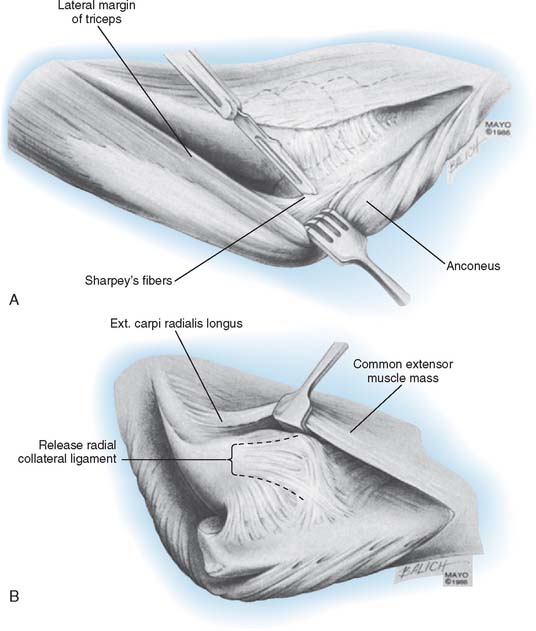
The triceps attachment is further released from the olecranon and the triceps mechanism is reflected from lateral to medial (Fig. 7-8A).
Technique
If more extensile exposure is required than has been obtained with the previous steps (see Figs. 7-5 and 7-6), a medial skin flap is elevated and the ulnar nerve identified. It is protected or translocated according to the merits of the case and after the release has proceeded according to the steps shown in Figure 7-6. The triceps and anconeus muscle sleeve is reflected from the tip of the olecranon by releasing Sharpey’s fibers (see Fig. 7-8A). The entire extensor mechanism including anconeus is thus reflected from lateral to medial (see Fig. 7-8B). After the triceps has been reflected and the posterior capsule released, the lateral collateral ligament may be detached from the humerus depending on the goal of the specific procedure and the additional exposure required. By flexing the elbow and removing the tip of the olecranon, the articular surface and the entire posterior humerus can be exposed.
POSTERIOR EXPOSURES
Extensile posterior exposure implies effective management of the triceps mechanism.5,37 In recent years, there has been a marked increased interest in revisiting and modifying previously described posterior surgical approaches.
Several skin incisions and techniques have been described. Although MacAusland27 used a transverse incision, most posterior skin incisions are longitudinal. The S incision of Ollier today is not as often used as the straighter incision recommended by Langenbeck.25 Probably the most important aspect of any incision is that it should not cross the tip of the olecranon. Smith also attributed better healing to a medial incision as compared with a lateral one.38
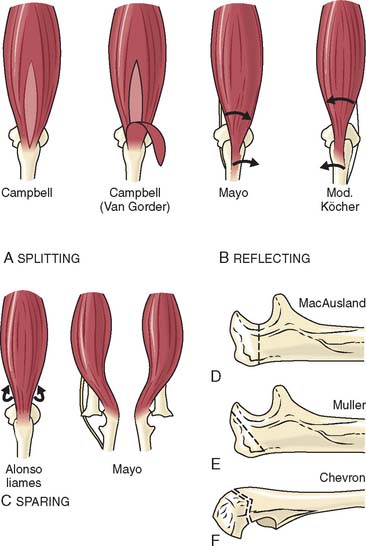
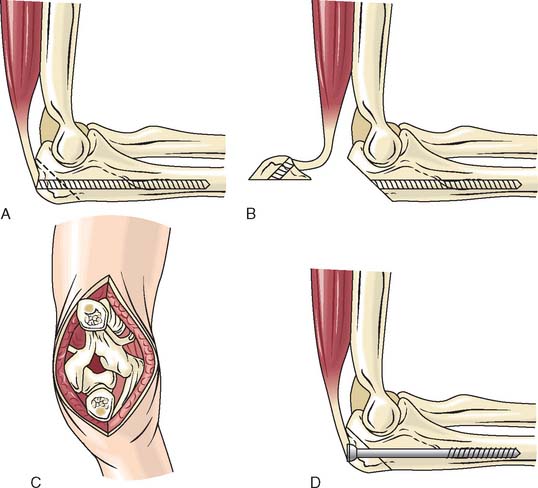
Releasing the triceps transverse section of the triceps mechanism at its musculotendinous junction has been described but does not afford adequate repair for optimal rehabilitation.46 Releasing the triceps at its attachment to the olecranon26 is not advisable, owing to the difficulty of adequate repair and possible disruption during rehabilitation.9 Today we categorize triceps management into four categories: (1) triceps splitting, (2) triceps reflecting, (3) triceps preserving, and (4) olecranon osteotomy (Fig. 7-9). A midline splitting incision was described as early as 1918 by James Thompson to expose the distal humerus for fractures, but it did not include release from the ulna to provide exposure of the joint itself.44
Splitting the triceps in line with the muscle fibers and at its insertion to expose the humerus and the elbow joint was described by Langenback25 and Campbell.10 This approach has had considerable resurgence of interest in recent years. When contracture is present, Campbell first separated the tendon from the muscle as an inverted V and then released the muscle fibers longitudinally. This technique, recommended later by Van Gorder46 for distal humerus fractures, allows lengthening of the musculotendinous unit, which may be necessary to fully mobilize the ankylosed joint. This triceps torque exposure has also faced a renewed interest and popularity in recent years.
