Chapter 61 Status Epilepticus
3 Describe the classification and clinical presentation of SE
 Generalized convulsive SE involves tonic flexion of the axial muscles, flexion in the arms and legs followed by extension, clenching of teeth, forced expiration, dilation of the pupils or sluggish pupillary light responses, and upward or lateral eye deviation. The uninterrupted jerking or shivering during the clonic phase may gradually resolve, but tonic spasm may occur again with a similar pattern of jerking and resolution. As the duration of the seizures increases, the movements and muscle contractions may become reduced despite continued generalized electrical activity in the brain.
Generalized convulsive SE involves tonic flexion of the axial muscles, flexion in the arms and legs followed by extension, clenching of teeth, forced expiration, dilation of the pupils or sluggish pupillary light responses, and upward or lateral eye deviation. The uninterrupted jerking or shivering during the clonic phase may gradually resolve, but tonic spasm may occur again with a similar pattern of jerking and resolution. As the duration of the seizures increases, the movements and muscle contractions may become reduced despite continued generalized electrical activity in the brain.


7 Name general treatment measures for SE
 An oral airway can be used if feasible, although most patients with prolonged SE may benefit from early endotracheal intubation.
An oral airway can be used if feasible, although most patients with prolonged SE may benefit from early endotracheal intubation.

 Vital signs should be recorded regularly.
Vital signs should be recorded regularly.
 A blood sample should be collected as soon as possible to rule out hypoglycemia.
A blood sample should be collected as soon as possible to rule out hypoglycemia.


 Whenever appropriate, vasopressor agents should be used to support the circulation.
Whenever appropriate, vasopressor agents should be used to support the circulation.


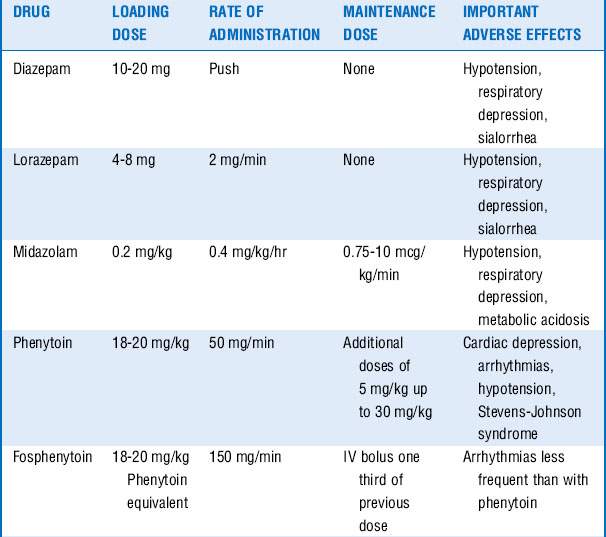
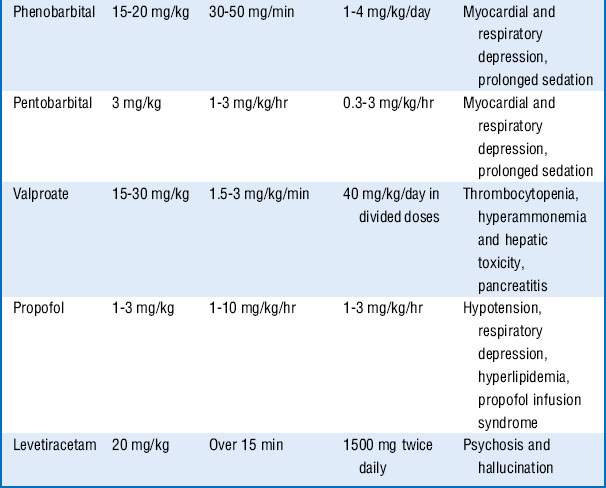
10 What are the third-line treatments for SE ?
These drugs are often associated with hemodynamic changes when administered in the doses mentioned and may require vasopressors to maintain adequate blood pressures. Prolonged infusion of high doses of propofol may also result in a rare complication known as the propofol infusion syndrome, with refractory bradycardia, metabolic acidosis, rhabdomyolysis, renal failure, and cardiovascular collapse. Treatment includes discontinuation of the propofol infusion and supportive care. Additional drugs that may be tried, if seizures continue, include carbamazepine, oxcarbazepine, topiramate, lamotrigine, and gabapentin. See Table 61-1.
14 What general measures should be considered after control of the seizures?
Key Points Status Epilepticus
1. SE is defined as seizures lasting ≥5 minutes or two or more seizures between which there is incomplete recovery of consciousness or function.
2. Morbidity and mortality are high in SE, and aggressive treatment strategies should be instituted immediately.
3. The most common cause of SE in a patient with known seizure disorder is low AED levels, whereas de novo SE is usually a manifestation of structural brain injuries or an illness that may require immediate diagnosis and treatment.
4. Treatment for SE is directed at stabilizing the patient’s condition, controlling the seizure, and identifying the cause. The underlying disease should be treated promptly.
5. First-line treatment to control the seizures often includes a benzodiazepine, for example, IV lorazepam. Second-line antiepileptic drug (phenytoin or fosphenytoin) can be given simultaneously with the first-line drug, or 1 minute after its administration if seizure persists. If third-line antiepileptic drugs (phenobarbital, valproate, or levetiracetam) do not stop the seizures, proceed to continuous infusion therapy with midazolam, pentobarbital, or propofol.
1 Bleck T.P. Intensive care unit management of patients with status epilepticus. Epilepsia. 2007;48(Suppl 8):59–60.
2 Chen J.W., Wasterlain C.G. Status epilepticus: pathophysiology and management in adults. Lancet Neurol. 2006;5:246–256.
3 Costello D.J., Cole A.J. Treatment of acute seizures and status epilepticus. J Intensive Care Med. 2007;22:319–347.
4 DeLorenzo R.J., Pellock J.M., Towne A.R., et al. Epidemiology of status epilepticus. J Clin Neurophysiol. 1995;12:316–325.
5 Fountain N.B., Lothman E.W. Pathophysiology of status epilepticus. J Clin Neurophysiol. 1995;12:326–342.
6 Huff J.S., Fountain N.B. Pathophysiology and definitions of seizures and status epilepticus. Emerg Med Clin North Am. 2011;29:1–13.
7 Lowenstein D.H., Bleck T., Macdonald R.L. It’s time to revise the definition of status epilepticus. Epilepsia. 1999;40:120–122.
8 Lucas M.J., Leveno K.J., Cunningham F.G. A comparison of magnesium sulfate with phenytoin for the prevention of eclampsia. N Engl J Med. 1995;333:201–205.
9 Mayer S.A., Claassen J., Lokine J., et al. Refractory status epilepticus: frequency, risk factors, and impact on outcome. Arch Neurol. 2002;59:205–210.
10 Mayhue F.E. IM midazolam for status epilepticus in the emergency department. Ann Emerg Med. 1988;17:643–645.
11 Neligan A., Shorvon S.D. Frequency and prognosis of convulsive status epilepticus of different causes: a systematic review. Arch Neurol. 2010;67:931–940.
12 Phillips S.A., Shanahan R.J. Etiology and mortality of status epilepticus in children. A recent update. Arch Neurol. 1989;46:74–76.
13 Pritchard J.A. The use of the magnesium ion in the management of eclamptogenic toxemia. Surg Gynecol Obstet. 1955;100:131–140.
14 Treiman D.M., Meyers P.D., Walton N.Y., et al. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med. 1998;339:792–798.
15 Wijdicks E.F., Parisi J.E., Sharbrough F.W. Prognostic value of myoclonus status in comatose survivors of cardiac arrest. Ann Neurol. 1994;35:239–243.
