[level-membership-for-opthalmology-category]16.2
Stargardt Disease
Clinical Features:
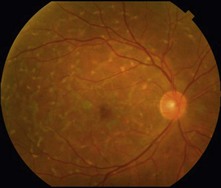
There are characteristic ‘pisciform’ flecks or yellowish deposits that can be in the shape of a fish tail at the level of the RPE. These deposits collect in the posterior pole, usually within the macula, but can be outside the arcades (Fig. 16.2.1). The peripapillary region is characteristically spared. Some cases show severe macular atrophy as the prominent feature.
OCT Features:
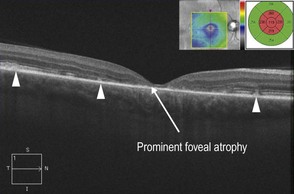
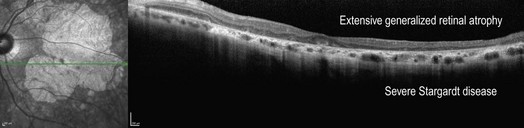
OCT confirms the RPE as the location of the abnormal deposits and shows associated outer retinal atrophy, which may be present parafoveally (Fig. 16.2.2) or involve the fovea (Fig. 16.2.3). In more advanced stages of the disease, there is more widespread outer retinal atrophy that can lead to geographic atrophy (Fig. 16.2.4).
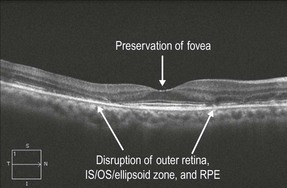
Figure 16.2.2 OCT in a patient with mild Stargardt disease shows a characteristic bulls-eye maculopathy with preservation of the central fovea. There is disruption of the outer retina, IS–OS/ellipsoid zone, and RPE in a parafoveal ring.
Ancillary Testing:
Fluorescein angiography and fundus autofluorescence (FAF) can help in confirming the diagnosis. FA can show a characteristic dark choroid (Fig. 16.2.5), present in about 70% of cases. FAF highlights the abnormal RPE deposits and best demonstrates the peripapillary sparing (Figs 16.2.6 and 16.2.7).
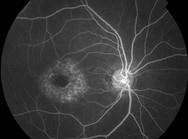
Figure 16.2.5 Mid-phase fluorescein angiography shows staining of central pisciform flecks in addition to a dark choroid.
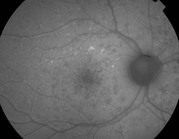
Figure 16.2.6 FAF corresponding to Figures 16.2.1 and 16.2.2 shows areas of both hyperautofluorescence and hypo-autofluorescence corresponding to pisciform flecks. The characteristic peripapillary sparing is well demonstrated.
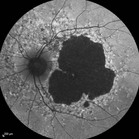
Figure 16.2.7 FAF corresponding to Figure 16.2.3 shows areas of both hyperautofluorescence and hypo-autofluorescence corresponding to pisciform flecks. There is a large area of profound central hypo-autofluorescence corresponding to the geographic atrophy. Again, there is characteristic peripapillary sparing.
[/level-membership-for-opthalmology-category][not-level-membership-for-opthalmology-category]16.2
Stargardt Disease
Clinical Features:
There are characteristic ‘pisciform’ flecks or yellowish deposits that can be in the shape of a fish tail at the level of the RPE. These deposits collect in the posterior pole, usually within the macula, but can be outside the arcades (Fig. 16.2.1). The peripapillary region is characteristically spared. Some cases show severe macular atrophy as the prominent feature.
OCT Features:
OCT confirms the RPE as the location of the abnormal deposits and shows associated outer retinal atrophy, which may be present parafoveally (Fig. 16.2.2) or involve the fovea (Fig. 16.2.3
[/not-level-membership-for-opthalmology-category]
