Strictures may resemble normal plicae circulares on enteroclysis
• CT findings
Strictures: Short segmental narrowing of lumen with dilation of bowel upstream
Mucosal inflammation: Mucosal hyperenhancement and submucosal edema
• Capsule endoscopy can confirm diagnosis
TOP DIFFERENTIAL DIAGNOSES
• Crohn disease
Longer segments of transmural involvement
• Celiac-sprue disease
Jejunoileal fold pattern reversal
• Ischemic enteritis
Bowel wall thickening; strictures can be late result
• Radiation enteritis
Longer strictures; pelvic SB segments
• Small intestine vasculitis
Long segments of submucosal edema
PATHOLOGY
• All NSAID (including aspirin) formulations can cause enterocolitis
Slow-release formulations affect distal SB and colon
CLINICAL ISSUES
• Often asymptomatic; may have symptoms of bowel obstruction
• May require surgery or endoscopic balloon dilation for bowel obstruction
(Left) Axial NECT in a 40-year-old man shows a dilated proximal, mid small bowel and collapsed colon.
(Right) Axial NECT in the same patient shows an abrupt transition from dilated to collapsed small bowel in the ileum . There was no history of prior abdominal surgery, making adhesive bowel obstruction a less likely etiology.
(Left) Small bowel follow-through in the same patient shows dilation of the proximal small bowel and a short stricture in the ileum with collapsed bowel distal to this point.
(Right) Spot film from the small bowel study in the same patient shows a short stricture in the ileum. At surgery, the stricture was confirmed, resected, and determined to be due to injury from chronic use of NSAIDs.
TERMINOLOGY
Abbreviations
• Nonsteroidal anti-inflammatory drugs (NSAIDs)
Synonyms
• Diaphragm disease
Definitions
• Focal strictures in small bowel (SB) secondary to NSAID use










 and collapsed colon.
and collapsed colon.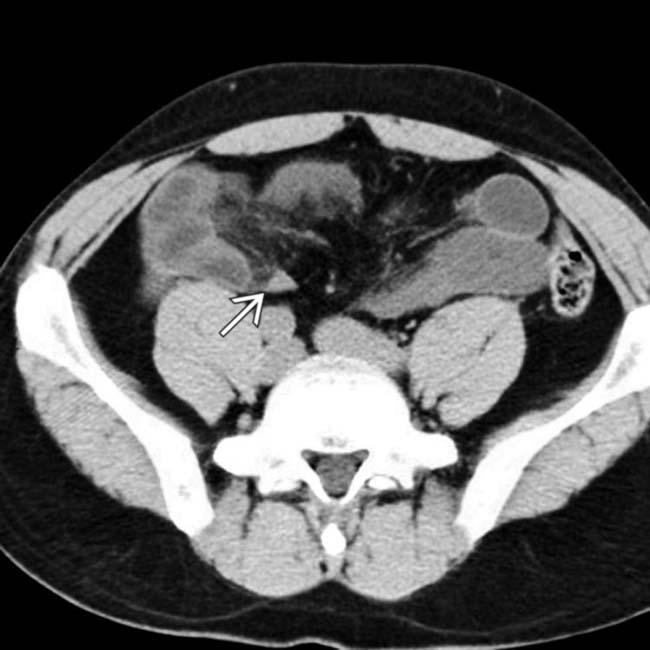
 . There was no history of prior abdominal surgery, making adhesive bowel obstruction a less likely etiology.
. There was no history of prior abdominal surgery, making adhesive bowel obstruction a less likely etiology.
 with collapsed bowel distal to this point.
with collapsed bowel distal to this point.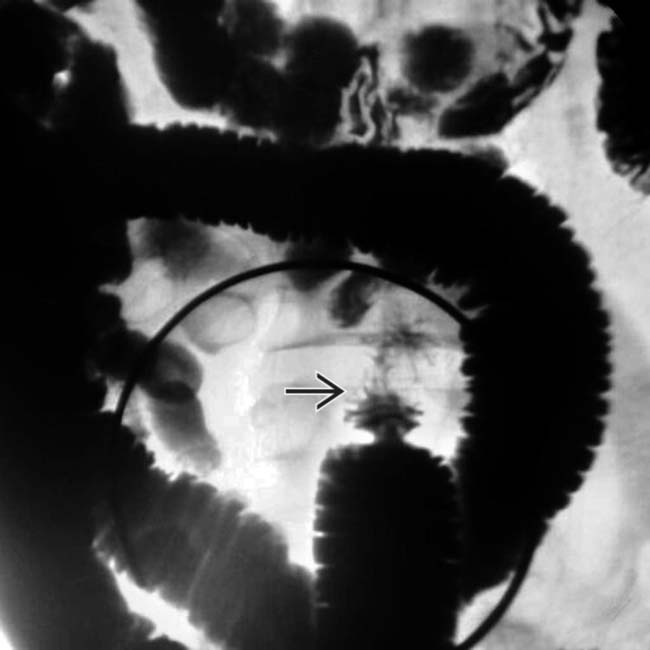
 in the ileum. At surgery, the stricture was confirmed, resected, and determined to be due to injury from chronic use of NSAIDs.
in the ileum. At surgery, the stricture was confirmed, resected, and determined to be due to injury from chronic use of NSAIDs.


















