Portal venous gas may result from septic mesenteric or portal vein thrombophlebitis (rather than ischemia)
TOP DIFFERENTIAL DIAGNOSES
• Crohn disease
• Intestinal scleroderma
• Abdominal foreign bodies
• Meckel diverticulum
PATHOLOGY
• Diverticulitis: Result of perforation of diverticulum
• Small bowel obstruction
Large diverticula may cause adhesions, intussusception, or volvulus
• Bleeding
Thin-walled vessels in wall of diverticulum may bleed
• Malabsorption or anemia
Stasis within large or numerous diverticula with bacterial overgrowth
Bacteria consume vitamins (including B12) and nutrients
CLINICAL ISSUES
• Most common signs/symptoms: Usually asymptomatic unless perforated
• Other signs/symptoms: Malabsorption, steatorrhea, megaloblastic anemia secondary to B12 deficiency
(Left) Small bowel follow-through shows multiple large duodenal and small bowel diverticula in a patient with no relevant symptoms.
(Right) Axial CECT in the same patient shows one of the large diverticula as a thin-walled cystic structure with a gas-fluid level . One of the duodenal diverticula is fluid-filled and might be mistaken for a cystic lesion in the head of the pancreas.
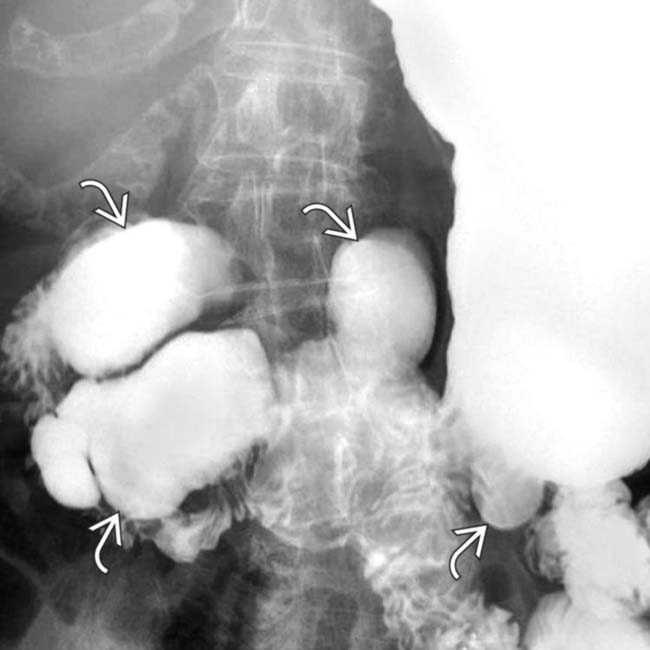
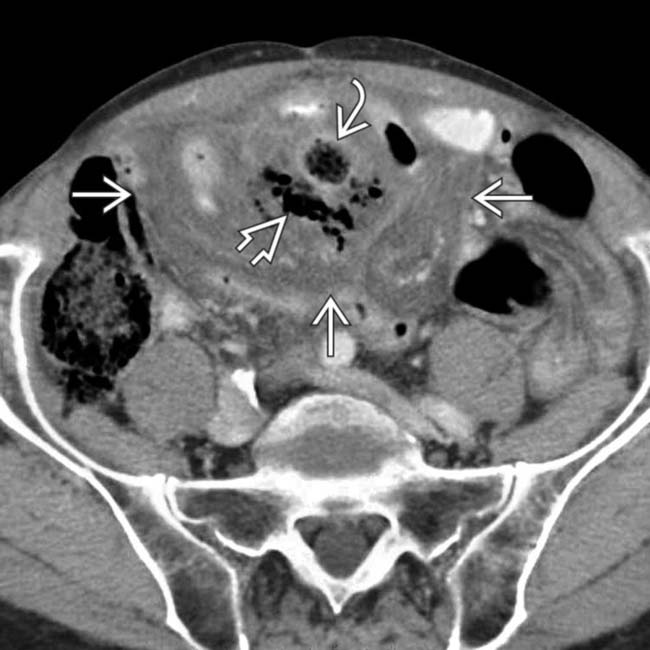
(Left) Small bowel follow-through performed at a time when the patient was asymptomatic shows several small bowel diverticula .
(Right) Axial CECT at a time of acute symptoms in the same patient shows extraluminal gas and fluid with a large inflammatory process centered in the small bowel mesentery. A diverticulum filled with gas and particulate debris is seen . A perforated diverticulum and mesenteric abscess were confirmed at surgery.









 in a patient with no relevant symptoms.
in a patient with no relevant symptoms.
 . One of the duodenal diverticula
. One of the duodenal diverticula  is fluid-filled and might be mistaken for a cystic lesion in the head of the pancreas.
is fluid-filled and might be mistaken for a cystic lesion in the head of the pancreas.
 .
.
 with a large inflammatory process
with a large inflammatory process  centered in the small bowel mesentery. A diverticulum filled with gas and particulate debris is seen
centered in the small bowel mesentery. A diverticulum filled with gas and particulate debris is seen  . A perforated diverticulum and mesenteric abscess were confirmed at surgery.
. A perforated diverticulum and mesenteric abscess were confirmed at surgery.


