1. Maddah, G, et al. Management of sigmoid volvulus: options and prognosis. J Coll Physicians Surg Pak. 2014; 24(1):13–17.
2. Selçuk Atamanalp, S. Treatment for ileosigmoid knotting: a single-center experience of 74 patients. Tech Coloproctol. 2014; 18(3):233–237.
3. Meyer, F, et al. Unusual “twister”-like appearance of a sigmoid volvulus on computed tomography. Endoscopy. 2007; 39(Suppl 1):E295.
4. Tiah, L, et al. Sigmoid volvulus: diagnostic twists and turns. Eur J Emerg Med. 2006; 13(2):84–87.
5. Agaoglu, N, et al. Surgical treatment of the sigmoid volvulus. Acta Chir Belg. 2005; 105(4):365–368.
6. Chandrasekaran, TV, et al. Minimally invasive stapled surgical approach to the management of sigmoid volvulus. Ann R Coll Surg Engl. 2005; 87(5):381–382.
7. Matsumoto, S, et al. Computed tomographic imaging of abdominal volvulus: pictorial essay. Can Assoc Radiol J. 2004; 55(5):297–303.
8. Chiu, HH, et al. Recurrent sigmoid volvulus. Gastrointest Endosc. 2002; 56(3):419–420.
9. Kuzu, MA, et al. Emergent resection for acute sigmoid volvulus: results of 106 consecutive cases. Dis Colon Rectum. 2002; 45(8):1085–1090.
10. Chirdan, LB, et al. Sigmoid volvulus and ileosigmoid knotting in children. Pediatr Surg Int. 2001; 17(8):636–637.
11. Moore, CJ, et al. CT of cecal volvulus: unraveling the image. AJR Am J Roentgenol. 2001; 177(1):95–98.
12. Daniels, IR, et al. Recurrent sigmoid volvulus treated by percutaneous endoscopic colostomy. Br J Surg. 2000; 87(10):1419.
13. Dulger, M, et al. Management of sigmoid colon volvulus. Hepatogastroenterology. 2000; 47(35):1280–1283.
14. Lee, SH, et al. The ileosigmoid knot: CT findings. AJR Am J Roentgenol. 2000; 174(3):685–687.
15. Madiba, TE, et al. The management of sigmoid volvulus. J R Coll Surg Edinb. 2000; 45(2):74–80.
16. Chung, YF, et al. Minimizing recurrence after sigmoid volvulus. Br J Surg. 1999; 86(2):231–233.
17. Javors, BR, et al. The northern exposure sign: a newly described finding in sigmoid volvulus. AJR Am J Roentgenol. 1999; 173(3):571–574.
18. Choi, D, et al. Endoscopic sigmoidopexy: a safer way to treat sigmoid volvulus? J R Coll Surg Edinb. 1998; 43(1):64.
19. Catalano, O. Computed tomographic appearance of sigmoid volvulus. Abdom Imaging. 1996; 21(4):314–317.
20. Frizelle, FA, et al. Colonic volvulus. Adv Surg. 1996; 29:131–139.
21. Forde, KA. Therapeutic colonoscopy. World J Surg. 1992; 16(6):1048–1053.
22. Gibney, EJ. Volvulus of the sigmoid colon. Surg Gynecol Obstet. 1991; 173(3):243–255.







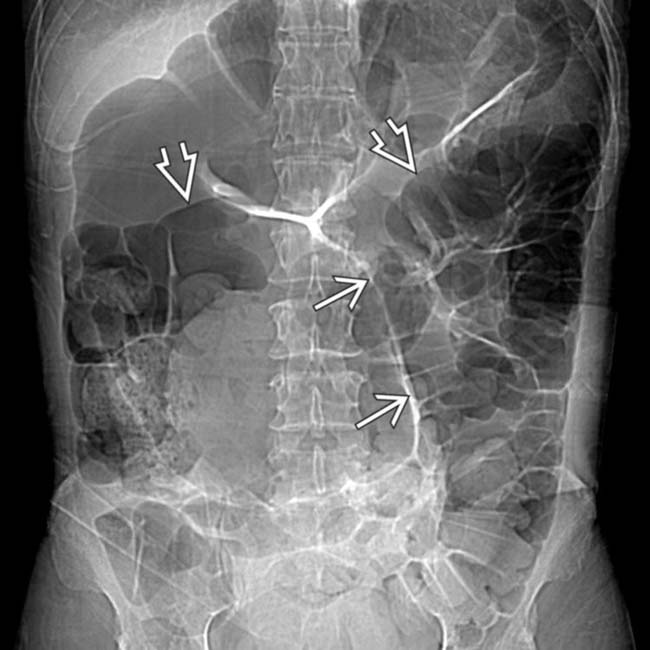
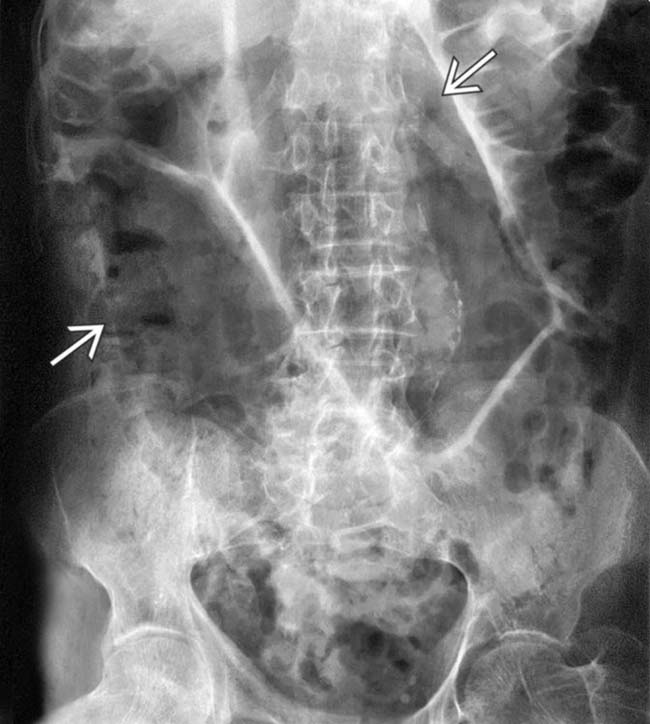
 form the “seam” of the football (or coffee bean) shape. The sigmoid extends into the upper abdomen above the transverse colon
form the “seam” of the football (or coffee bean) shape. The sigmoid extends into the upper abdomen above the transverse colon  .
.
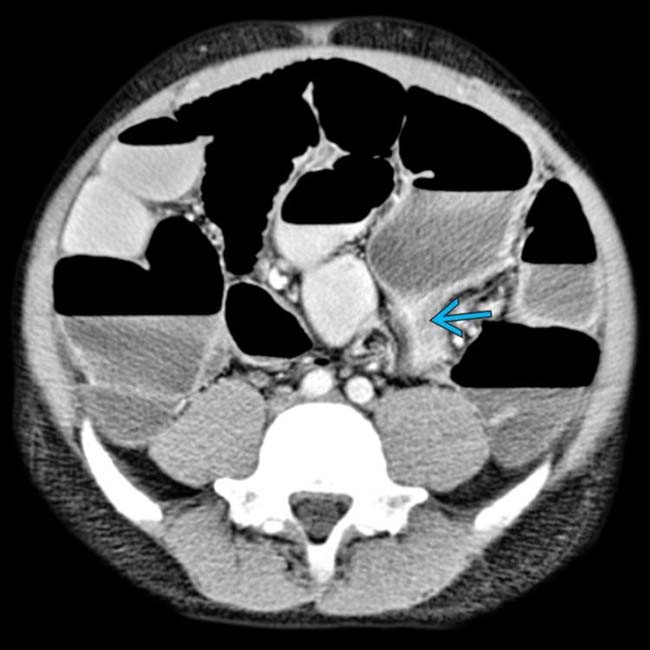
 with abrupt narrowing at its base
with abrupt narrowing at its base  .
.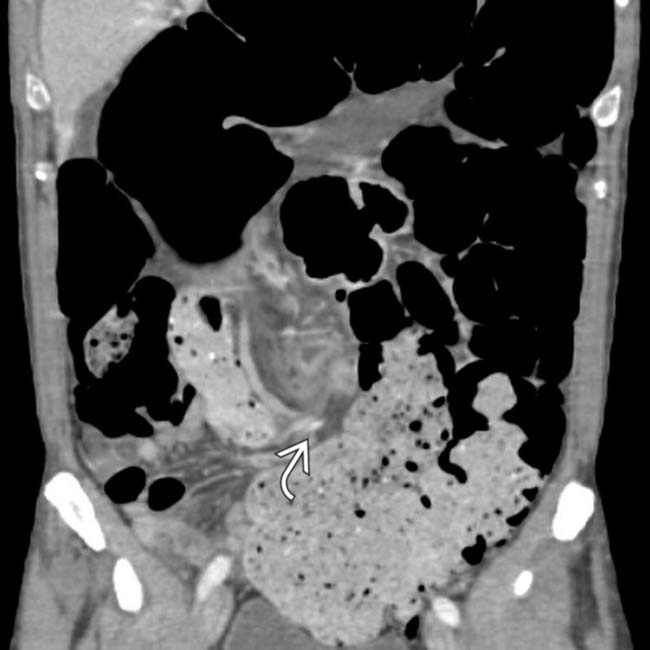
 . The dilated colonic segments upstream from the volvulus may be easier to distinguish on coronal sections.
. The dilated colonic segments upstream from the volvulus may be easier to distinguish on coronal sections.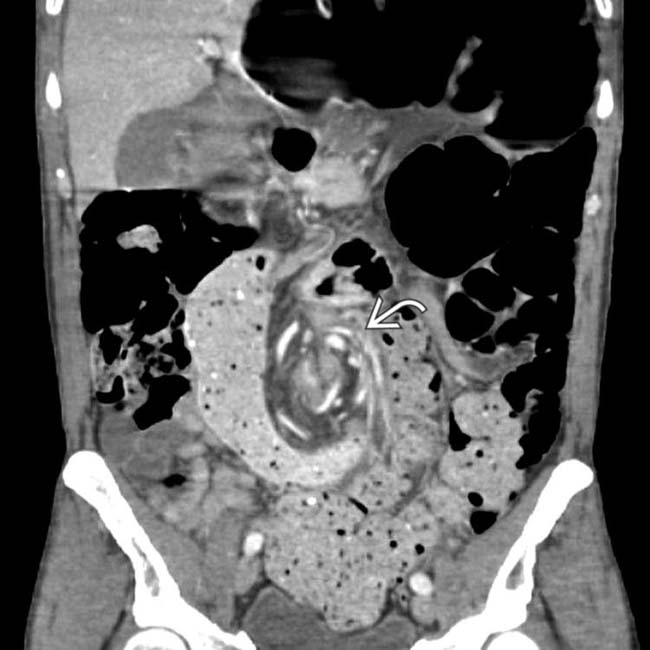
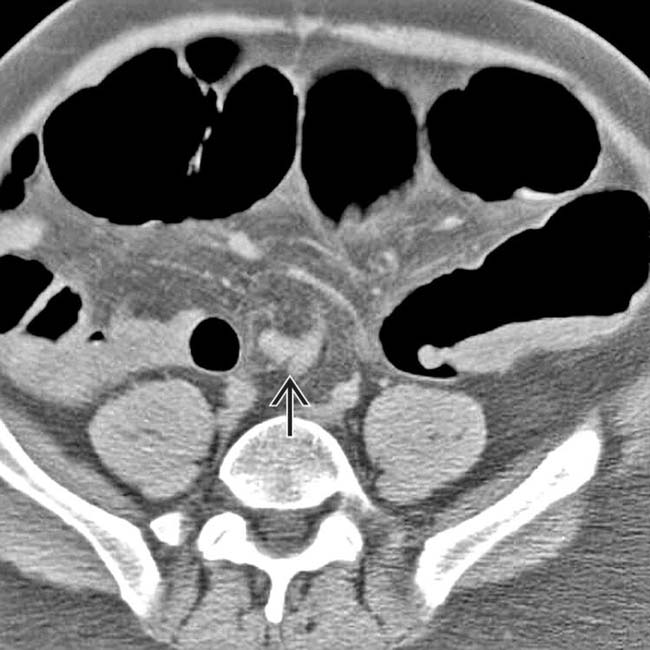
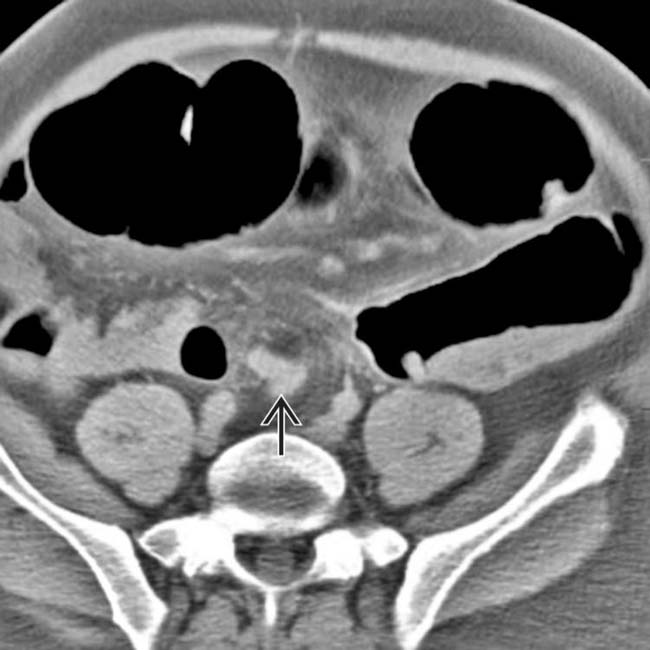
 of twisted colon and vessels at the base of the sigmoid mesentery.
of twisted colon and vessels at the base of the sigmoid mesentery.















































 of the twisted sigmoid colon.
of the twisted sigmoid colon.
 , characteristic findings in this setting.
, characteristic findings in this setting.
 in this typical presentation of a sigmoid volvulus.
in this typical presentation of a sigmoid volvulus.
 . This configuration is pathognomonic for sigmoid volvulus.
. This configuration is pathognomonic for sigmoid volvulus.
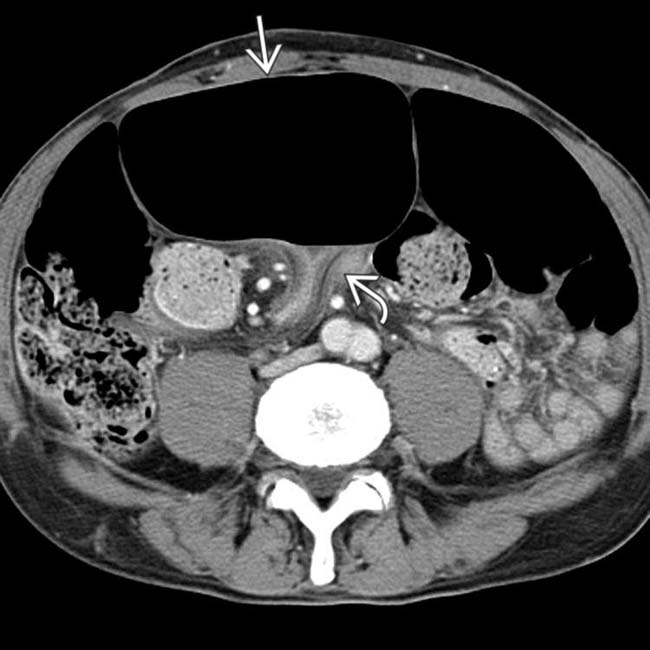
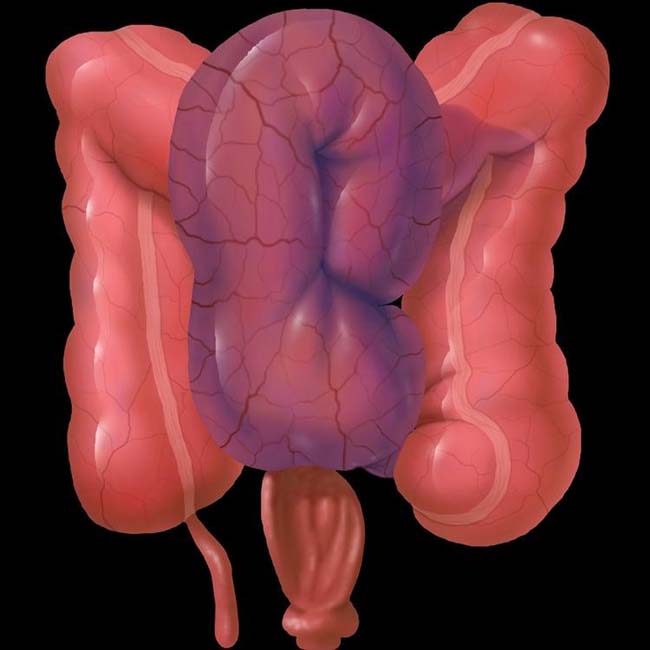
 as well as the ascending and descending colon
as well as the ascending and descending colon  . Note the apposed walls
. Note the apposed walls  of the sigmoid colon.
of the sigmoid colon.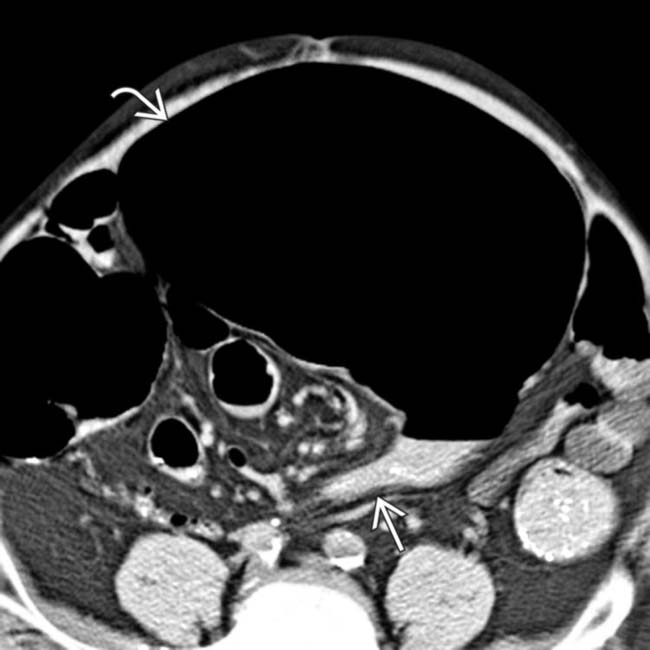
 from the volvulus obstructing the massively dilated sigmoid colon
from the volvulus obstructing the massively dilated sigmoid colon  .
.
 at the site of volvulus
at the site of volvulus  .
.
 .
.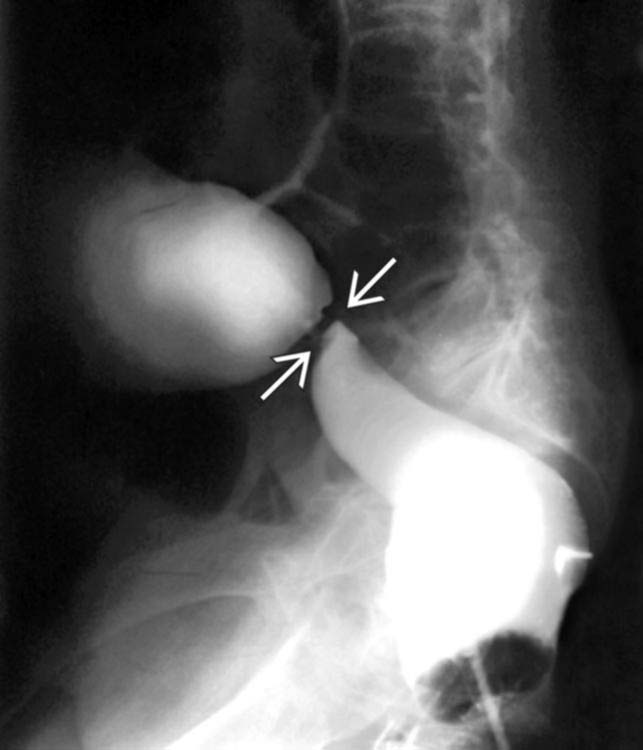
 corresponding to luminal narrowing at the site of sigmoid obstruction.
corresponding to luminal narrowing at the site of sigmoid obstruction.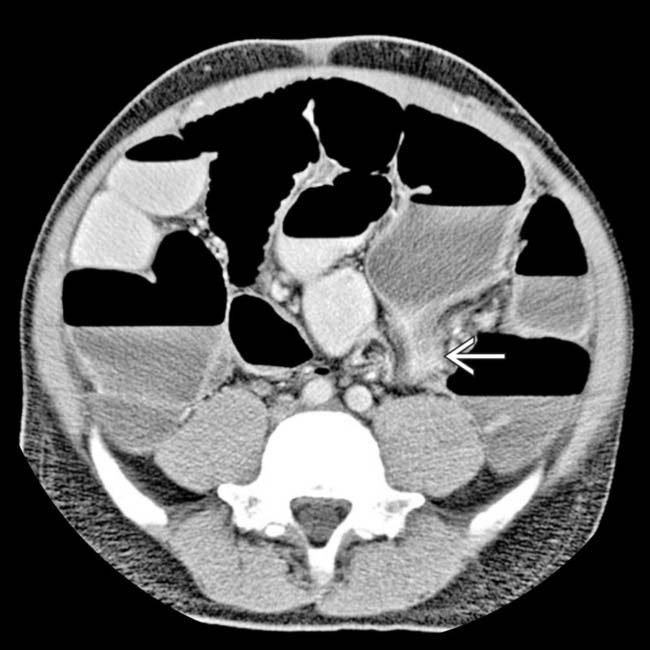
 of twisted sigmoid colon.
of twisted sigmoid colon.
 .
.
 .
.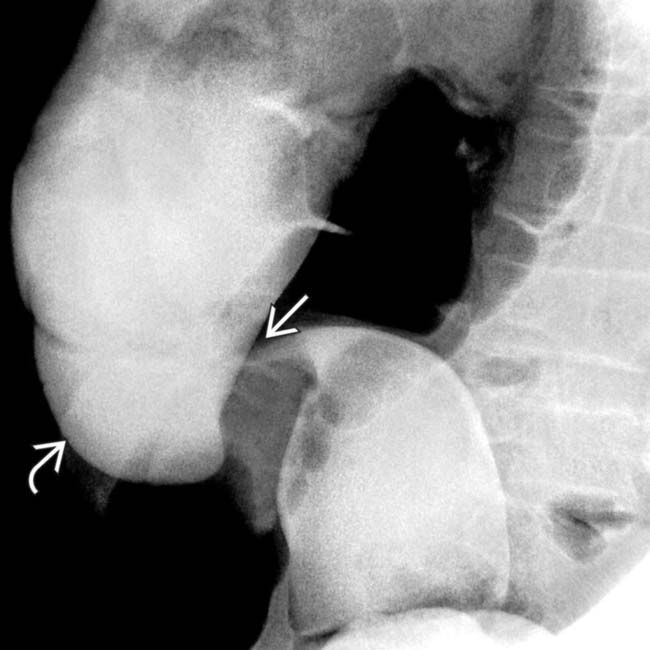
 and distal filling of the dilated colon
and distal filling of the dilated colon  due to partial obstruction.
due to partial obstruction.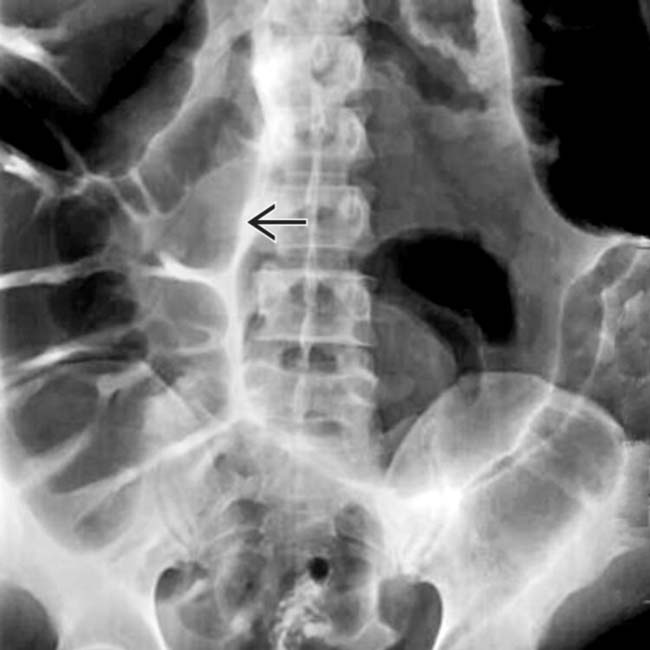
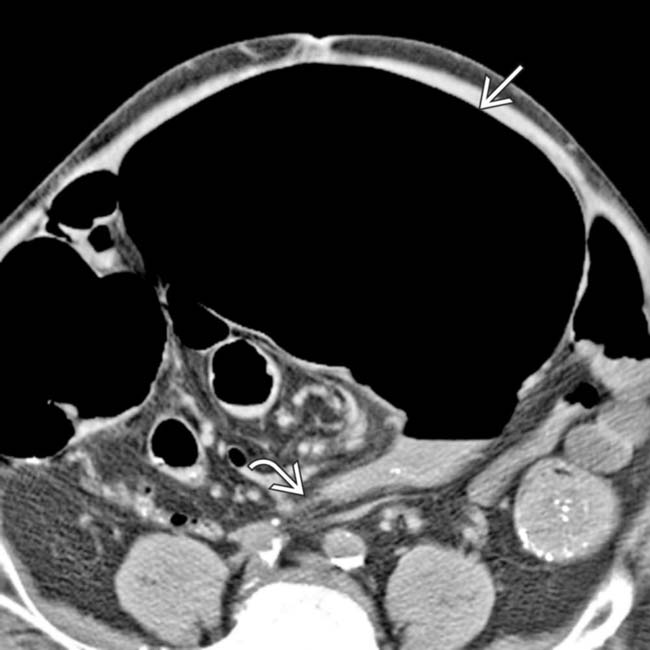
 represents the apposed walls of the dilated, inverted sigmoid colon and points toward the mesenteric volvulus.
represents the apposed walls of the dilated, inverted sigmoid colon and points toward the mesenteric volvulus.
 can be seen above the transverse colon, the “northern exposure” sign of sigmoid volvulus.
can be seen above the transverse colon, the “northern exposure” sign of sigmoid volvulus.
 .
.
 .
.




