Shoulder and Arm
Stephen Thompson, Luke Choi, Stephen Brockmeier, Mark D. Miller
Regional Anatomy and Surgical Intervals
Regional Anatomy
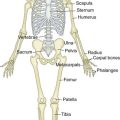
Osteology
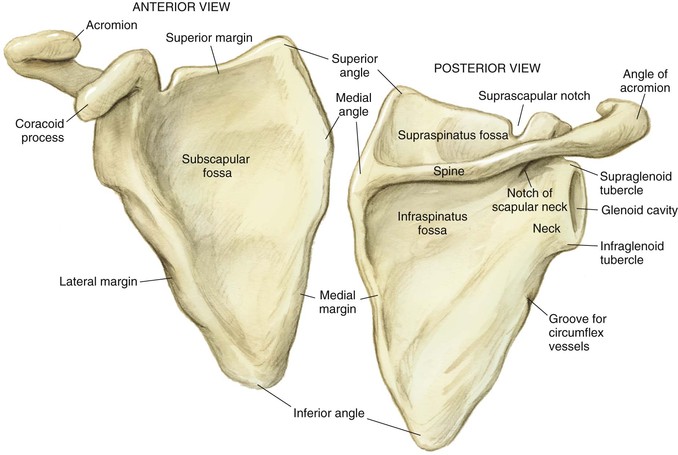
Scapula (Fig. 2-1)
A broad flat bone that serves as an attachment for 17 muscles and 4 ligaments
The scapular spine is the superior aspect of the scapula
The coracoid is the anterior projection that serves as the origin for several muscles and ligaments
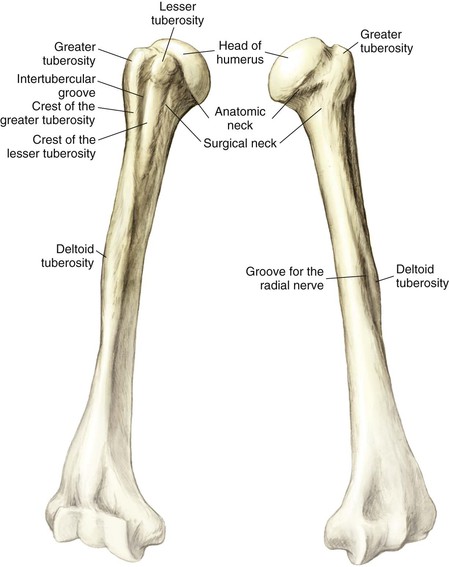
Humerus (Fig. 2-3)
The largest diaphyseal bone in the upper extremity
The hemispherical head is retroverted approximately 30 degrees
The anatomic neck is directly below the head
The surgical neck is approximately 2 cm distal to the anatomic neck
The greater tuberosity is the attachment for the supraspinatus, infraspinatus, and teres minor
The lesser tuberosity is the attachment for the subscapularis
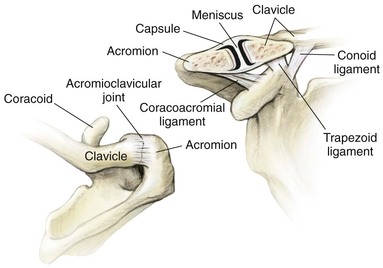
Arthrology
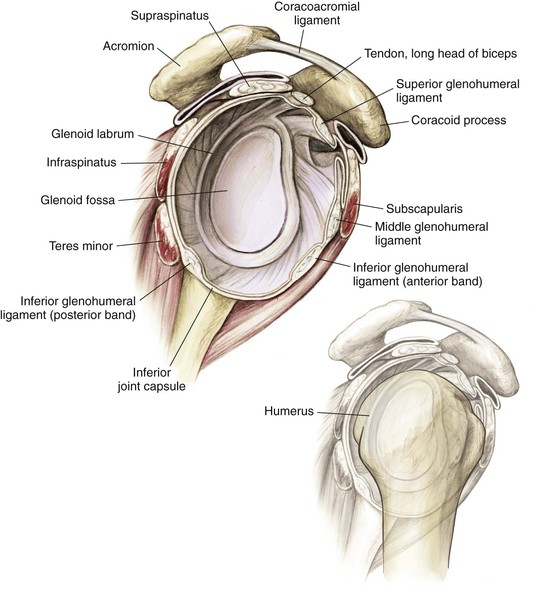
Glenohumeral Joint (Fig. 2-4)
This spheroidal (ball and socket) joint is designed for motion over stability
• Labrum—deepens the socket by 50% and provides a barrier against excessive translation
• Negative intraarticular pressure
• Capsule
• Glenohumeral ligaments (superior, middle, and inferior)
• The anterior band of the inferior glenohumeral ligament is the most important
• Resists inferior translation
Muscles
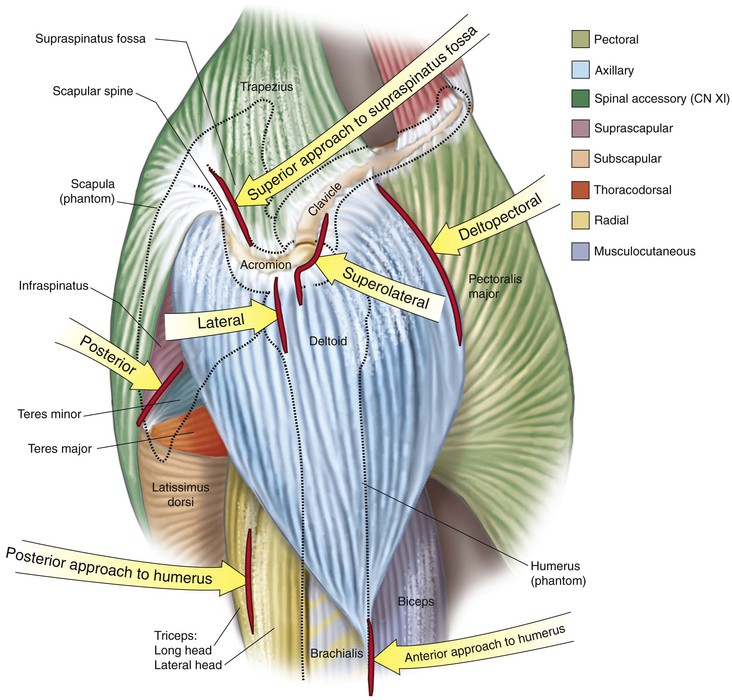
Shoulder Muscle Groups (Fig. 2-6 and Table 2-1)
Connect the upper limb to the axial skeleton
• Trapezius, latissimus, rhomboid major and minor, and levator scapulae
Connect the upper limb to the thoracic wall
• Pectoralis major and minor, subclavius, and serratus anterior
• Deltoid, teres major and minor, supraspinatus, infraspinatus, and subscapularis
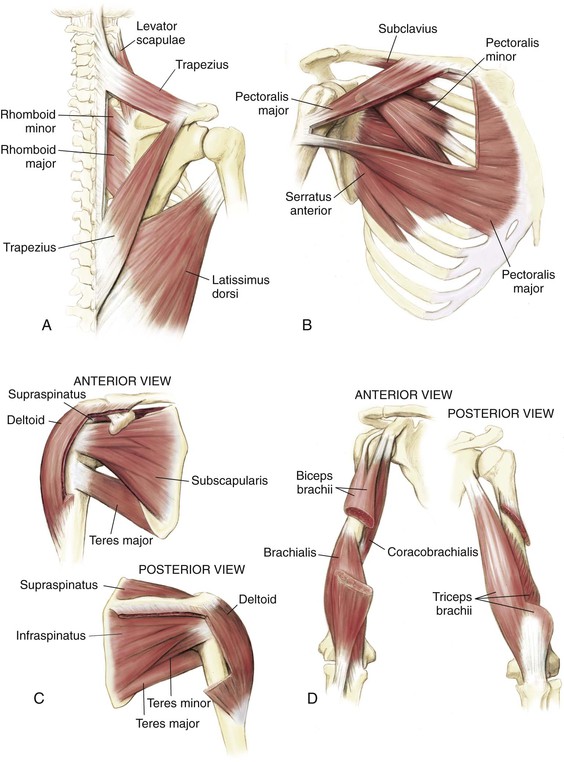
Table 2-1
Muscles of the Shoulder
| MUSCLE | ORIGIN | INSERTION | ACTION | INNERVATION |
| Trapezius | Spinous process C7-T12 | Clavicle, scapula (acromion, spinous process) | Rotate scapula | Cranial nerve XI |
| Lateral dorsi | Spinous process T6-S5, ilium | Humerus (ITG) | Extend, adduct, IR humerus | Thoracodorsal |
| Rhomboideus major | Spinous process T2-T5 | Scapula (medial border) | Adduct scapula | Dorsal scapular |
| Rhomboideus minor | Spinous process C7-T1 | Scapula (medial spine) | Adduct scapula | Dorsal scapular |
| Levator scapulae | Transverse process C1-C4 | Scapula (superior medial) | Elevate, rotate scapula | C3, C4 |
| Pectoralis major | Sternum, ribs, clavicle | Humerus (lateral ITG) | Adduct, IR arm | Mid and lower PN |
| Pectoralis minor | Ribs 3-5 | Scapula (coracoid) | Protract scapula | MPN |
| Subclavius | Rib 1 | Inferior clavicle | Depress clavicle | Upper trunk |
| Serratus anterior | Ribs 1-9 | Scapula (ventral medial) | Prevent winging | Long thoracic |
| Deltoid | Lateral clavicle, scapula | Humerus (deltoid tuberosity) | Abduct arm (2) | Axillary |
| Teres major | Inferior scapula | Humerus (medial ITG) | Adduct, IR, extend | Lower subscapular |
| Subscapularis | Ventral scapula | Humerus (lesser tuberosity) | IR arm, anterior stability | Upper and lower subscapular |
| Supraspinatus | Superior scapula | Humerus (GT) | Abduct (1), ER arm stability | Suprascapular |
| Infraspinatus | Dorsal scapula | Humerus (GT) | Stability, ER arm | Suprascapular |
| Teres minor | Scapula (dorsolateral) | Humerus (GT) | Stability, ER arm | Axillary |
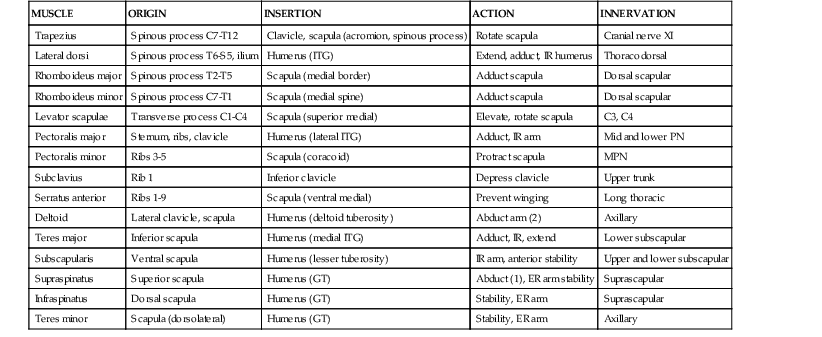
ER, External rotation; GT, greater tuberosity; IR, internal rotation; ITG, intertubercular groove; MPN, medial pectoral nerve; PN, pectoral nerve.
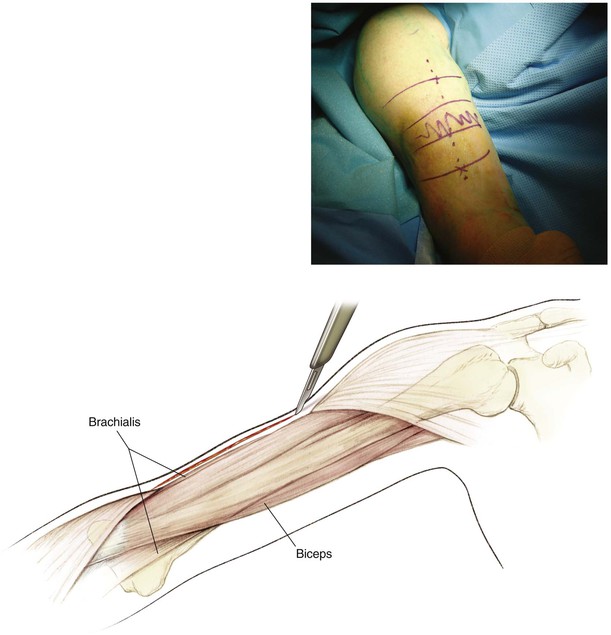
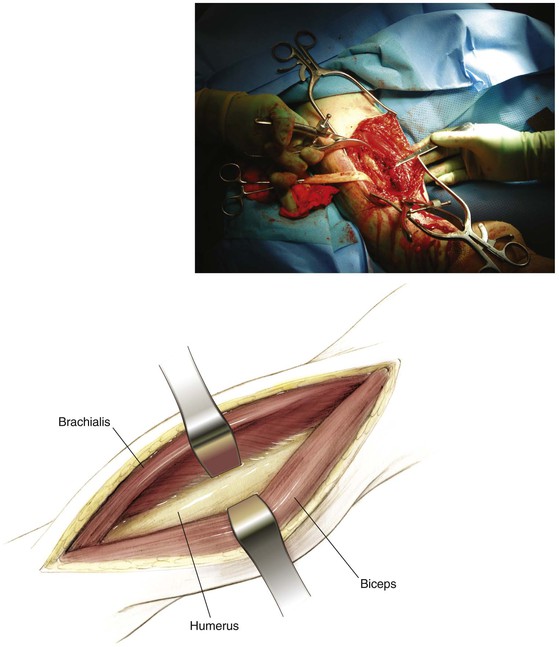
Arm Muscles (Fig. 2-6, D, and Table 2-2)
Table 2-2
Muscles of the Arm
| MUSCLE | ORIGIN | INSERTION | ACTION | INNERVATION |
| Coracobrachialis | Coracoid | Mid humerus medial | Flexion, adduction | Musculocutaneous |
| Biceps | Coracoid (SH) | Radial tuberosity | Supination, flexion | Musculocutaneous |
| Supraglenoid (LH) | ||||
| Brachialis | Anterior humerus | Ulnar tuberosity (anterior) | Flexes forearm | Musculocutaneous, radial |
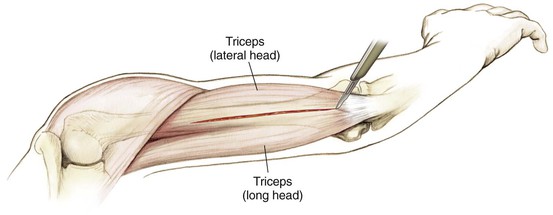
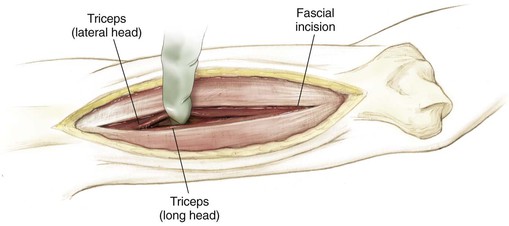
| Triceps | Infraglenoid (LH) | Olecranon | Extends forearm | Radial |
| Posterior humerus (LH) | ||||
| Posterior humerus (MH) |
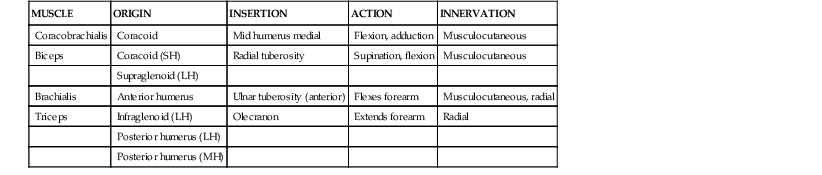
LH, Long head; MH, middle head; SH, short head.
Nerves
Brachial Plexus (Fig. 2-7)
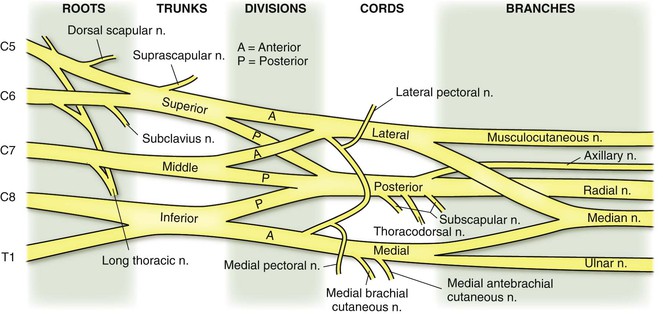
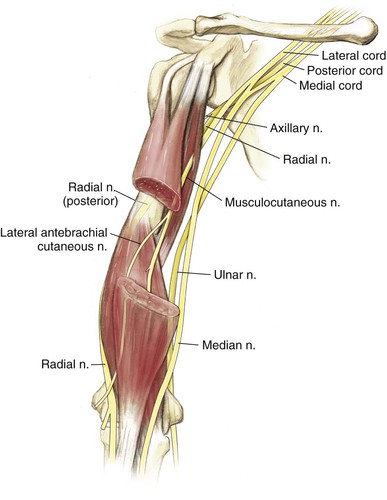
Major Arm Branches (Fig. 2-8)
Musculocutaneous nerve (lateral cord)
• Runs from medial to central anteriorly
• Supplies the biceps (short head), coracobrachialis, and part of the brachialis
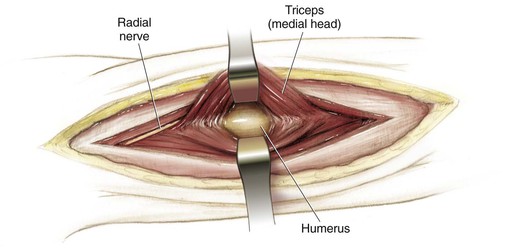
• Spirals behind the humerus from medial to lateral
• Supplies the triceps (all three heads) in the arm
Median nerve (medial and lateral cords)
• Runs just medial to the brachial artery in the medial arm
• No major branches in the arm
• Runs just lateral to the brachial artery in the medial arm
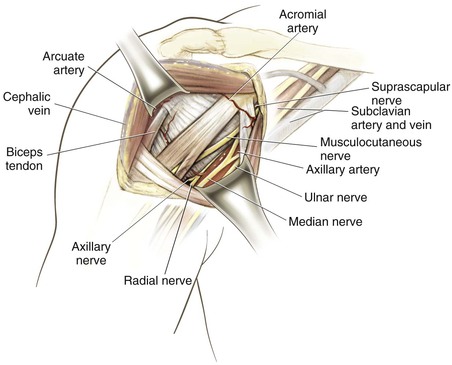
Vascularity (Fig. 2-9)
Subclavian Artery
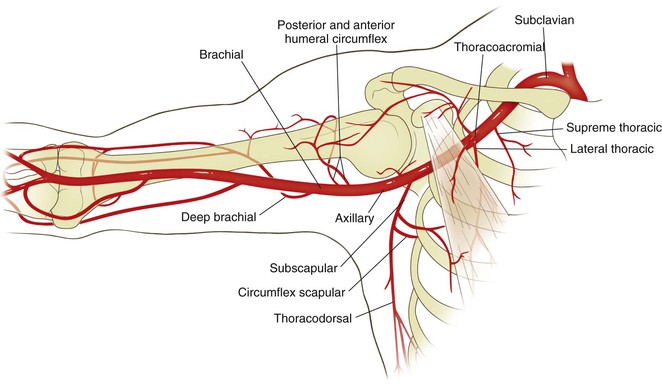
Axillary Artery (Table 2-3)
Three divisions based on the relationship to the pectoralis minor (1, proximal; 2, deep; 3, distal; Table 2-3)
(1) Proximal: supreme thoracic
(2) Deep: thoracoacromial and lateral thoracic (deltoid, acromial, pectoralis, and clavicular)
(3) Distal: subscapular, anterior, and posterior humeral circumflex
Table 2-3
Axillary Artery Branches
| PART | BRANCH | COURSE |
| 1 | Supreme thoracic | Medial to the serratus anterior and pectorals |
| 2 | Thoracoacromial | Four branches (deltoid, acromial, pectoralis, and clavicular) |
| Lateral thoracic | Descends to the serratus anterior | |
| 3 | Subscapular | Two branches (thoracodorsal and circumflex scapular [triangular space]) |
| Anterior humeral circumflex | Blood supply to the humeral head–arcuate artery lateral to the bicipital groove | |
| Posterior humeral circumflex | Branch in the quadrangular space accompanying the axillary nerve |
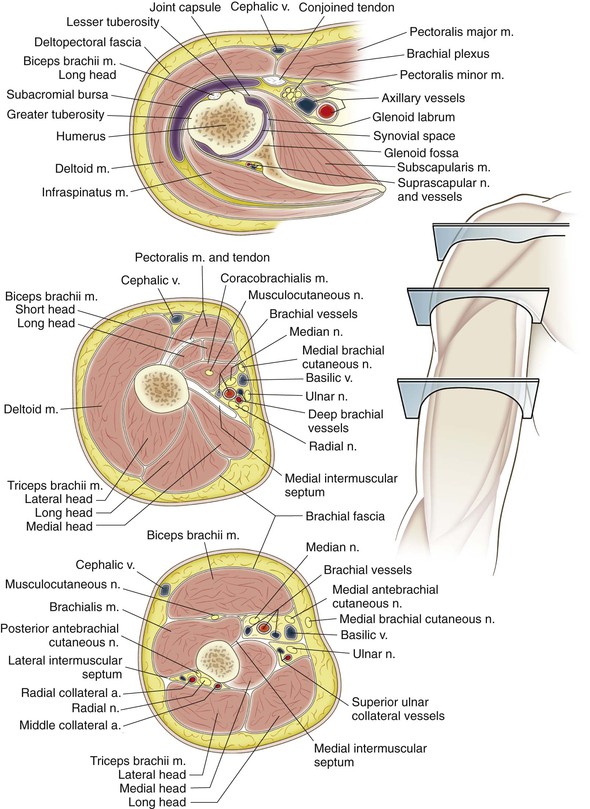
Cross-Sectional Anatomy
Surgical Intervals

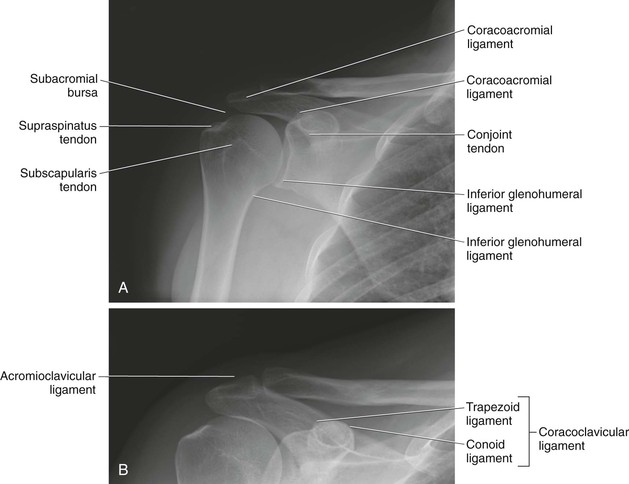
Radiologic Landmarks (Fig. 2-13, A and B)
Hazards
Shoulder (Fig. 2-14)
Nerves
Axillary Nerve
A branch of the posterior cord that supplies the deltoid and teres minor muscles
• Inferiorly as it transverses just below the glenohumeral joint
• Adduct and externally rotate the arm and stay directly on the neck of the glenoid with dissection
• Avoid retractor placement below the subscapularis and capsule
• Palpate the nerve with blunt dissection and use electrocautery without muscle relaxation
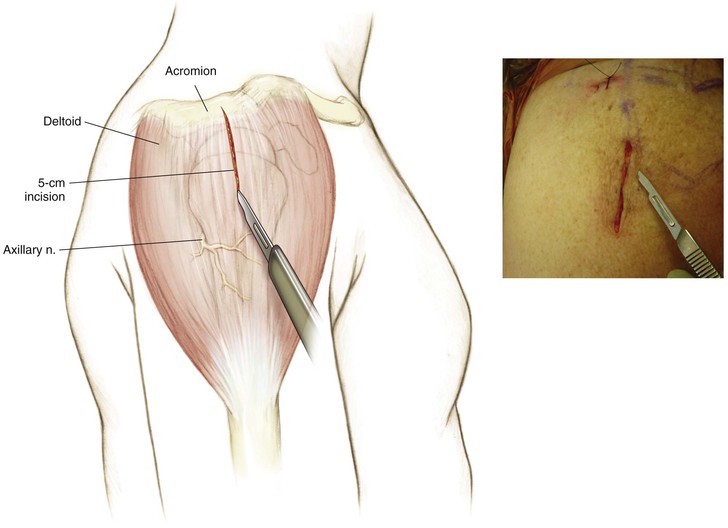
• Laterally with any incision or dissection 5 cm or more distal to the lateral acromion
• Place a marking suture at that location, and do not dissect below it
Musculocutaneous Nerve
Acromial Branch of the Thoracoacromial Artery
Surgical Approaches to the Shoulder and Arm
Anterior (Deltopectoral) Approach to the Shoulder (Video 2-1)
Indications
Positioning
Beach Chair Position (Fig. 2-15)
The head is secured in a Mayfield headrest or a commercially available beach chair attachment
The upper torso is elevated 30 to 60 degrees depending on the procedure performed
• Can cause transient hypotension
The opposite arm, legs, and other prominences are padded and secured
The operative shoulder and arm are positioned off the side of the operating table for full access
• A bump placed under the ipsilateral scapula may improve access
Rotating and tilting the bed away from the operative side can be helpful
Commercially available arm holders or positioners may be helpful

Incision
Extended Deltopectoral Incision (Fig. 2-16)
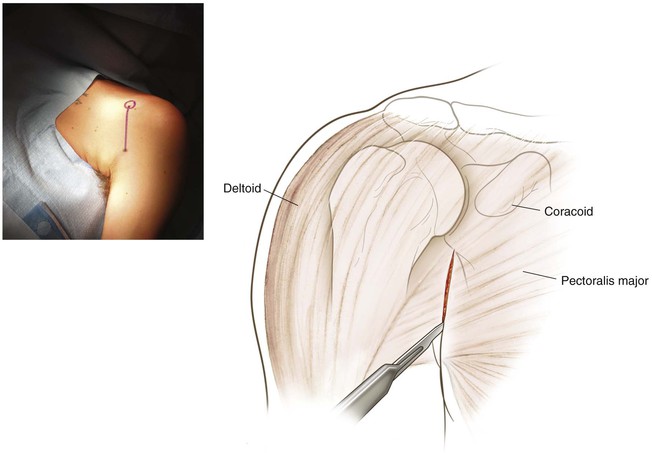
Superficial Dissection
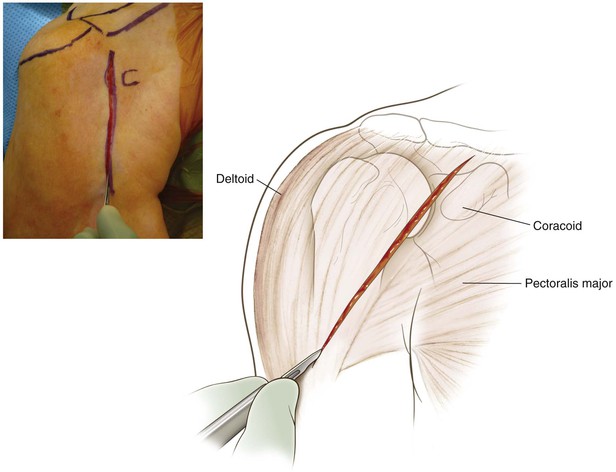
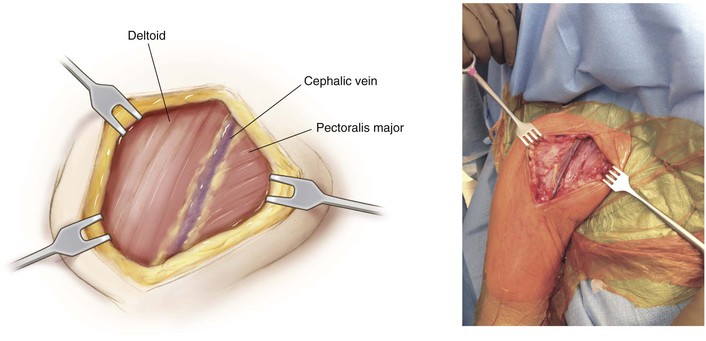
Identify and dissect the deltopectoral interval (Fig. 2-18)
• The cephalic vein is the key landmark
• Identification may be easier distally
• Small tributaries should be coagulated
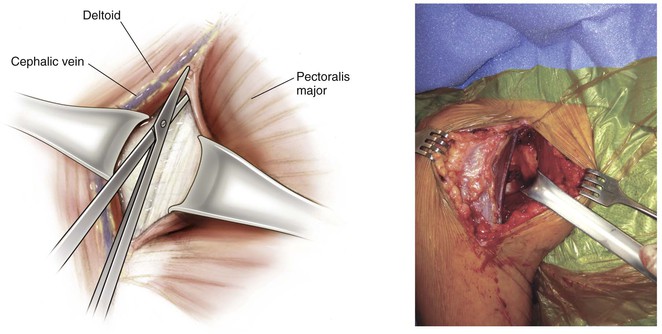
Retract the deltoid laterally and the pectoralis major medially (Fig. 2-19)
• Commercially available self-retaining retractors are useful
• A superiorly placed retractor above the coracoid can also be useful
• Make an incision in the clavipectoral fascia lateral to the conjoined tendon
Deep Dissection
Identify the subscapularis muscle and conjoint tendon (Fig. 2-20)
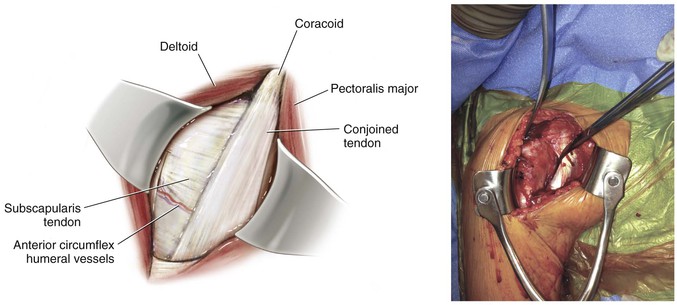
• Exposure of the glenohumeral joint is dependent on the procedure and the surgeon’s preference
• For most procedures, release of the subscapularis tendon is necessary and may be performed via two different techniques
• Soft tissue subscapularis release either directly from bone or through the tendon substance
• Superficial osteotomy of the lesser tuberosity
• The subscapularis and capsule can be taken down together by making a vertical incision approximately 1 cm medial to the bicipital groove, placing traction sutures in the capsule and tendon, and dissecting along the neck of the humerus (Fig. 2-21)
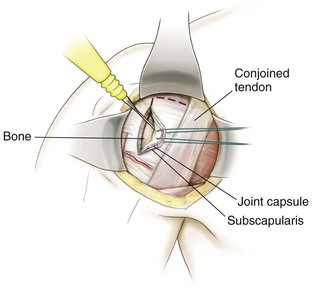
• Most often used for arthroplasty
• The capsule can be dissected further inferiorly, directly off the neck of the humerus
• The axillary nerve should be identified and protected with inferior dissection
• The subscapularis and capsule can be taken down separately by making a vertical incision approximately 1 cm medial to the bicipital groove and carefully “teasing” the subscapularis off the underlying capsule (Fig. 2-22)
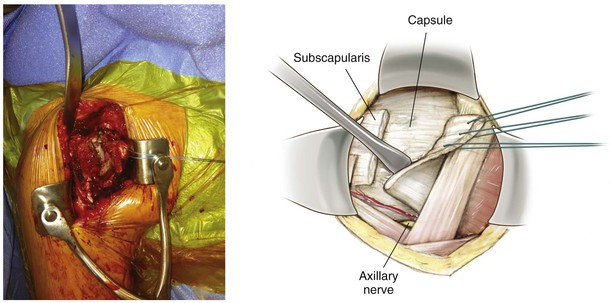
• Traction sutures are placed in the subscapularis, and a small elevator is used to assist in the dissection
• The subscapularis can be split in a horizontal direction (Fig. 2-23)
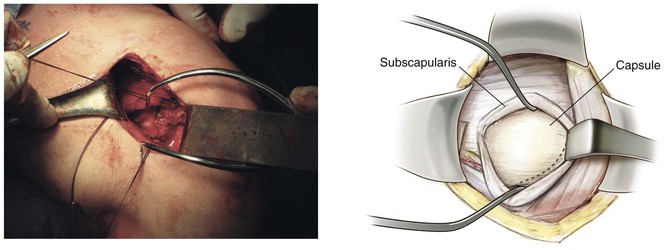
• Identify the bicipital groove
• Use a 2-mm drill to create four holes in the medial aspect of the groove
• Special forked and ring retractors can be used to expose the glenoid
Posterior Approach to the Shoulder (Video 2-2)
Indications
Positioning
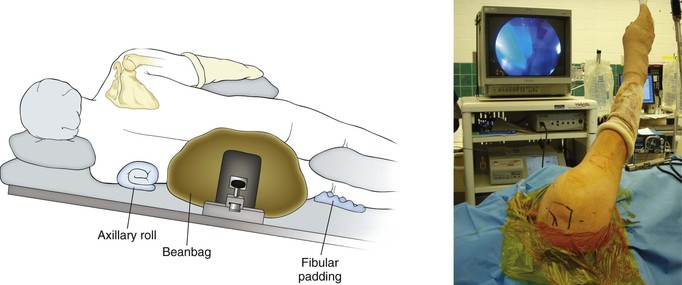
Lateral Decubitus Position (Fig. 2-24)
Can follow arthroscopy in this position
A beanbag is typically used with the operative side up
The nonoperative side must be well protected
• Pad the elbow, fibular head, and ankles
Position and drape the operative arm so it is free
• Alternatively, a commercially available arm positioner may be used
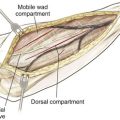
Deep Dissection
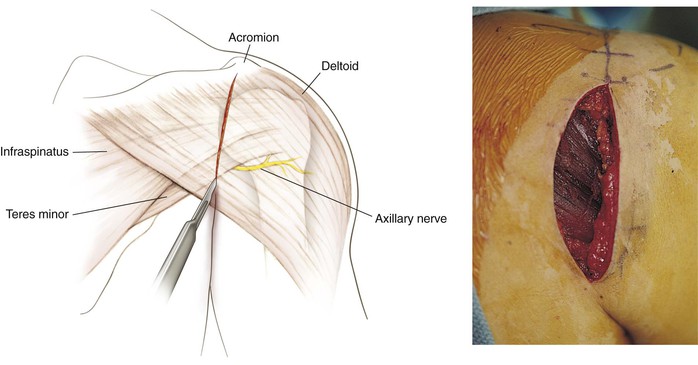
The interval between the infraspinatus and teres minor is identified
The infraspinatus is identified by three anatomic features
• Horizontal direction of muscle fibers
• Fatty raphe that divides the muscle belly
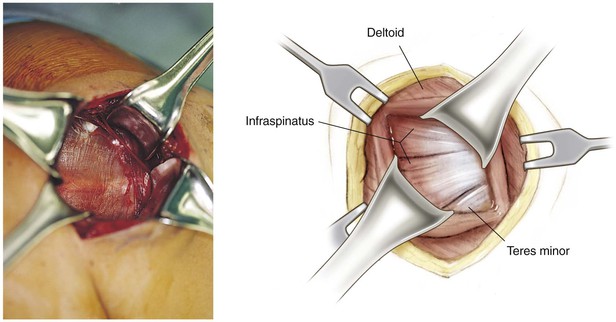
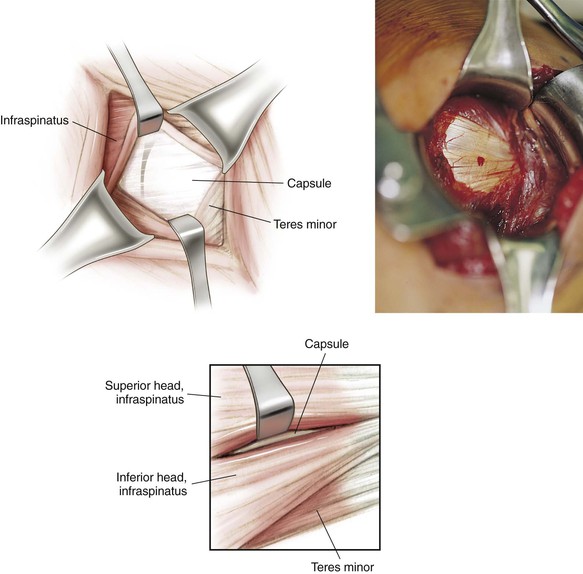
Typically the interval between the infraspinatus and teres minor is developed by blunt dissection and the posterior capsule is exposed by retraction of these muscles (Fig. 2-27)
Do not dissect below the teres minor muscle because of risk to the axillary nerve and posterior humeral circumflex artery
Superolateral Approach to the Shoulder (Video 2-3)
Indications
Superficial Dissection
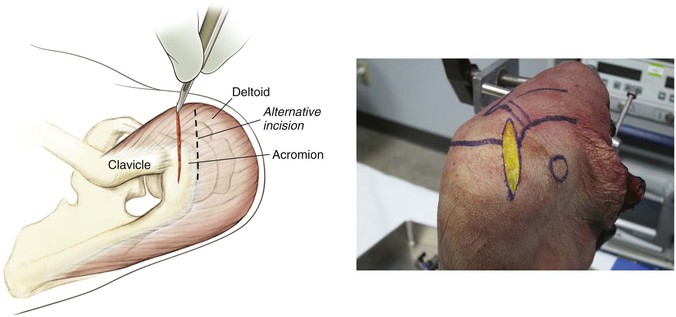
The deep deltoid fascia is identified along with the anterolateral corner of the acromion (Fig. 2-29)
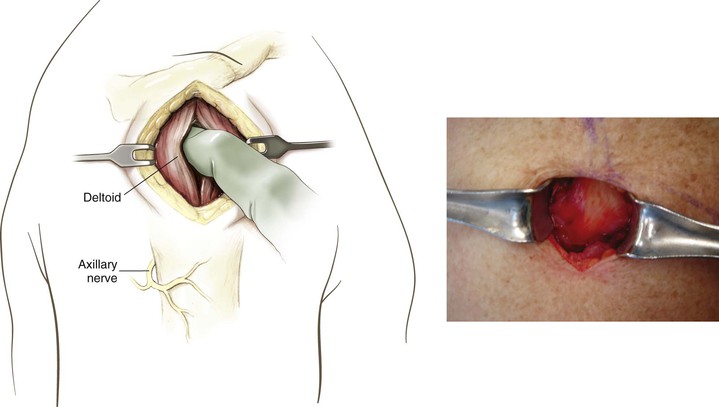
• The deltoid is detached and split
• Subperiosteally elevate the deltoid from the anterolateral acromion and acromioclavicular joint
• High-strength sutures are placed in the deltoid to aid in retraction and for later repair (Fig. 2-30)
• The deltoid can be split at the anterolateral border of the acromion (raphe) and extended 2 to 3 cm distally for exposure for rotator cuff repair


Deep Dissection
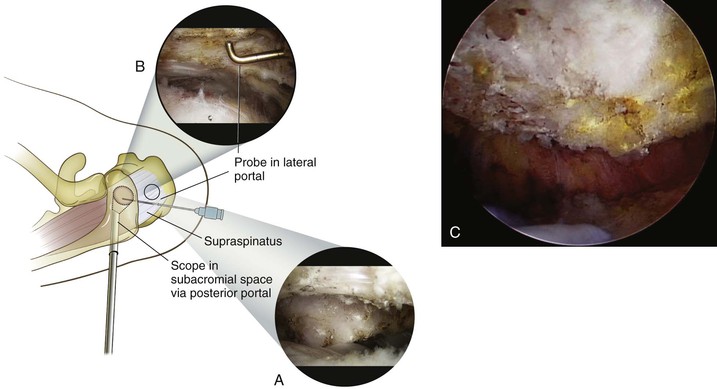
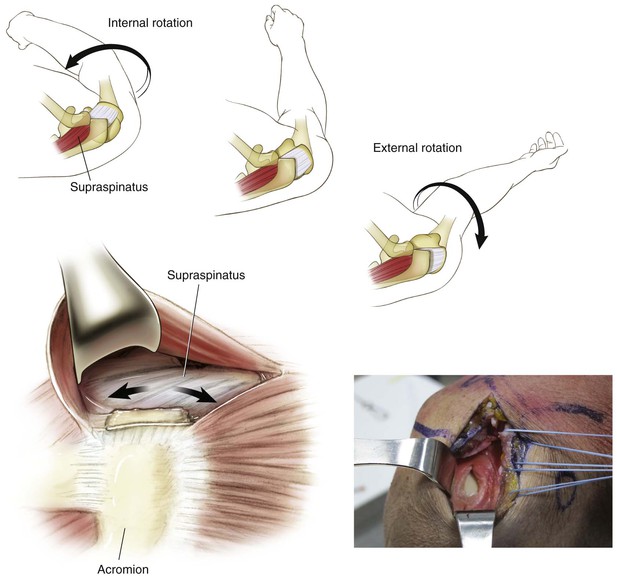
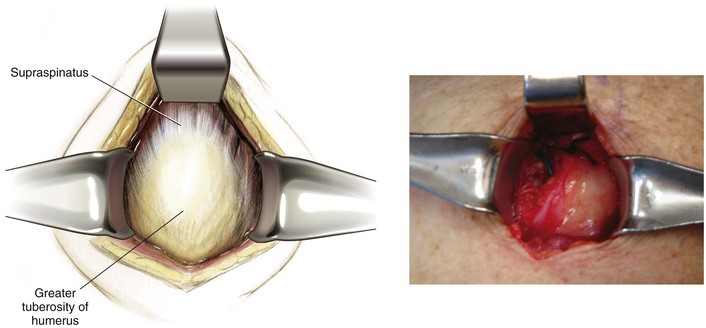
The coracoacromial ligament, subacromial bursa, and supraspinatus tendon are now identified (Fig. 2-31)
• The coracoacromial ligament can be incised, protected, or tagged, depending on the surgical plan
• The supraspinatus tendon and overlying bursa are exposed and explored by rotating the arm
• The humeral head may be seen if a rotator cuff tear is present (Fig. 2-32)

Closure
Reattachment of the Deltoid
It is crucial that the deltoid be reattached through drill holes into the acromion
• Using a 2-mm drill, create three holes into the acromion, taking care not to cause injury to the underlying structures (Fig. 2-33)
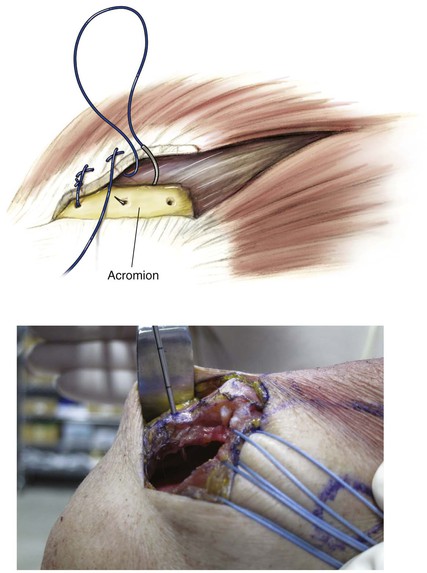
• Pass the previously placed sutures through the holes and tie them securely
The skin and subcutaneous tissues are closed in the standard fashion
Lateral (Deltoid-Splitting [Mini Open]) Approach to the Shoulder (Video 2-4)
Indications
Approach to the Acromioclavicular Joint
Indications
Incision
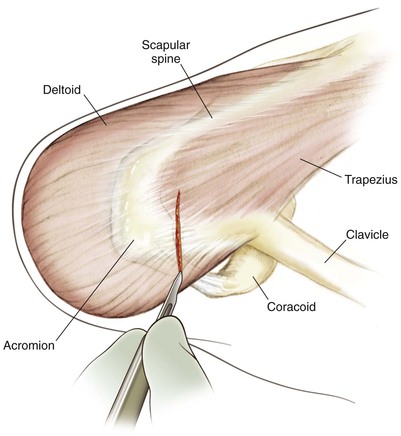
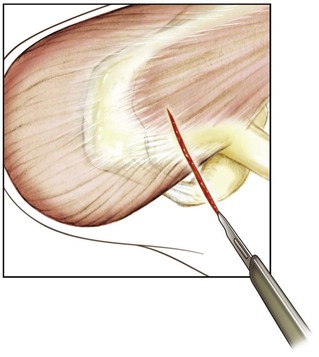
A 2- to 3-cm saber-type incision is made in Langer’s lines directly over the AC joint (Fig. 2-37)
• If an anterior portal is used, it often can be extended superiorly for this approach
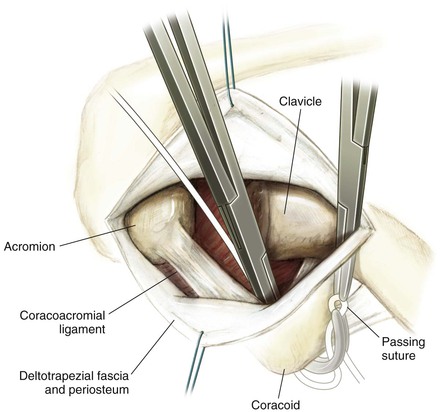
• For AC reconstruction procedures, the incision is placed more medially and can be extended more distally to allow access to the coracoid (Fig. 2-38)
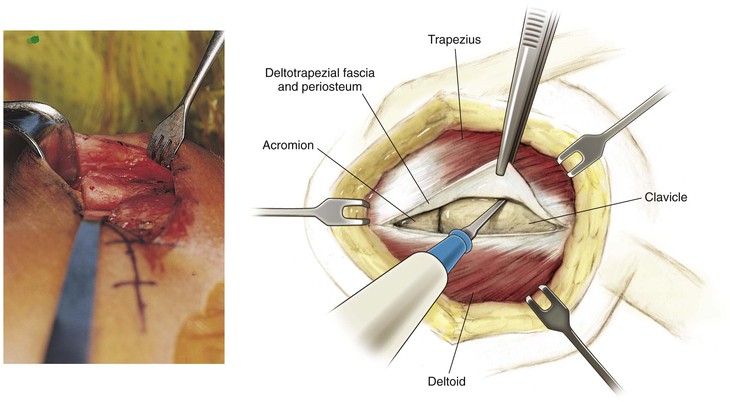
Superficial Dissection
Superior Approach to the Supraspinatus Fossa (Video 2-5)
Indications
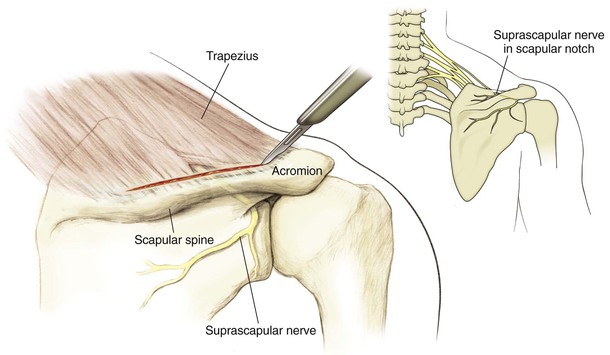
Superficial Dissection
Deep Dissection
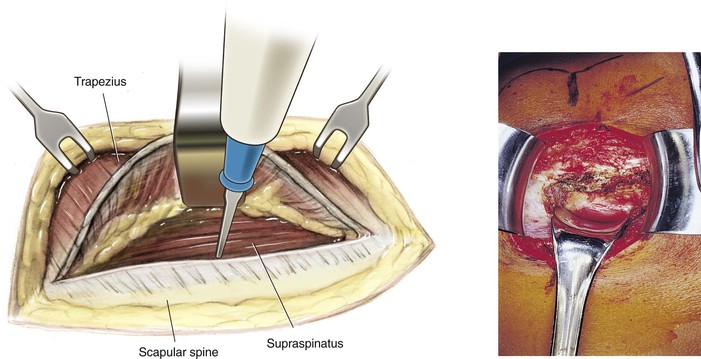
Expose the supraspinatus muscle deep to the trapezius
• A layer of fat is usually present below the trapezius, and the fiber orientation is different (trapezius fibers are oblique, and supraspinatus fibers go directly from medial to lateral)
• Retract the supraspinatus anteriorly
• Expose the suprascapular notch (Fig. 2-43)
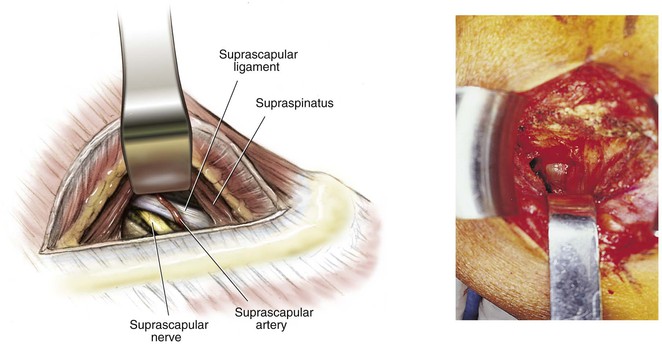
• Palpate the coracoid base and then palpate approximately 1 cm medially to locate the notch
• The suprascapular ligament is dissected
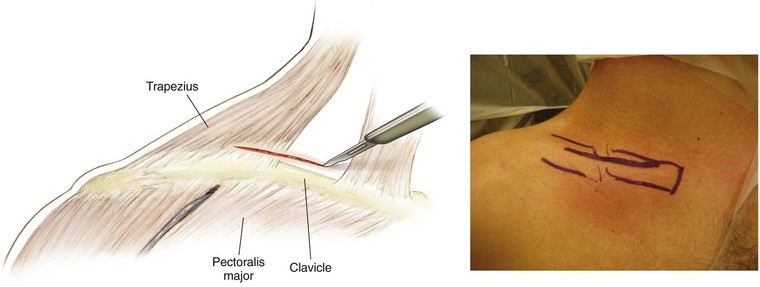
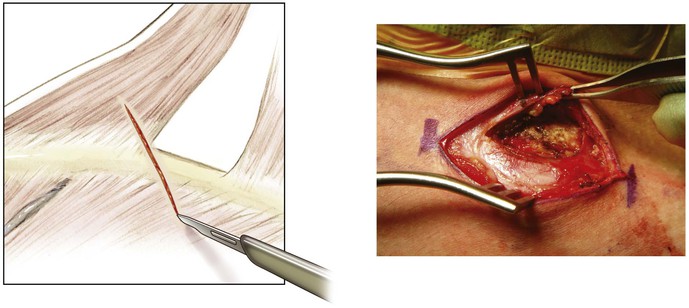
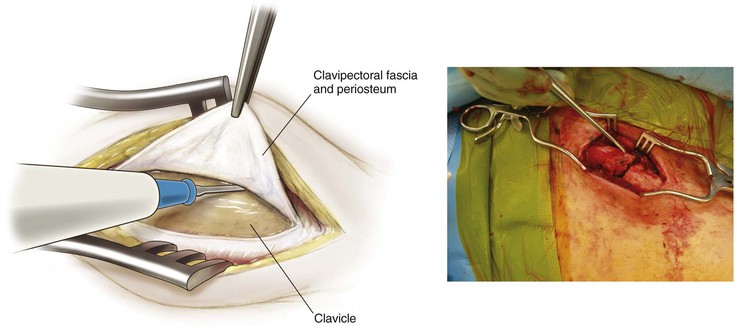
Approach to the Clavicle (Video 2-6)
Indications

Shoulder Arthroscopy
Indications
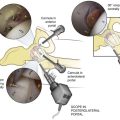
Portals (Fig. 2-52)
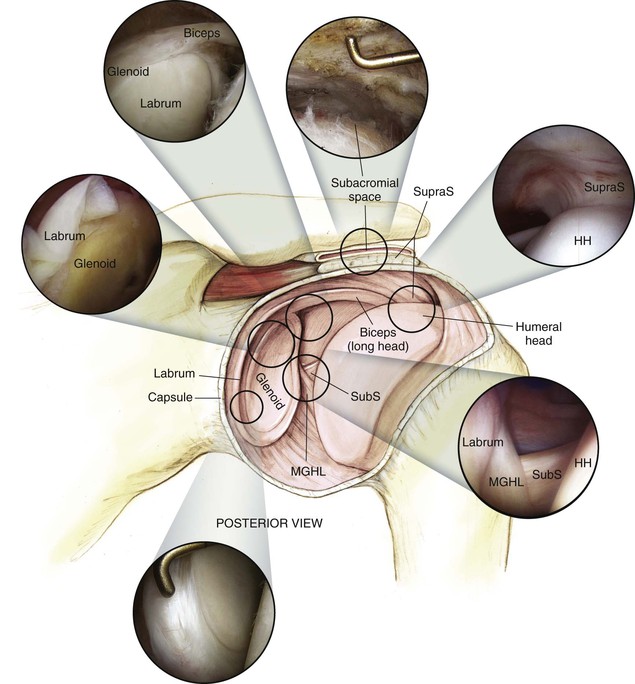
Posterior
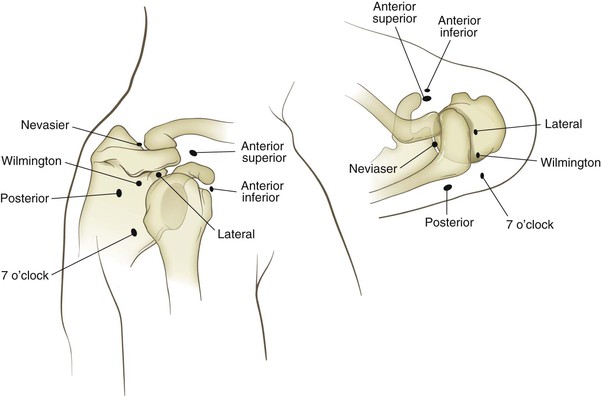
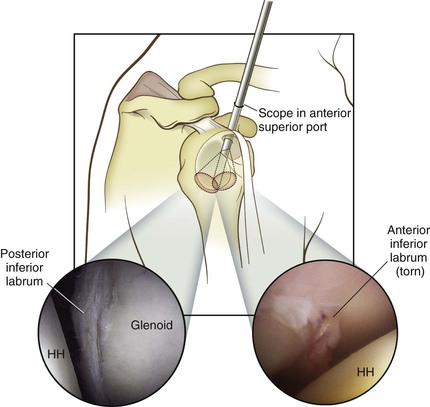
Anterior Superior
Location: superior and lateral to the coracoid
• Typically localized with a spinal needle from outside-in just anterior to the biceps adjacent to the superior glenoid (Fig. 2-53)
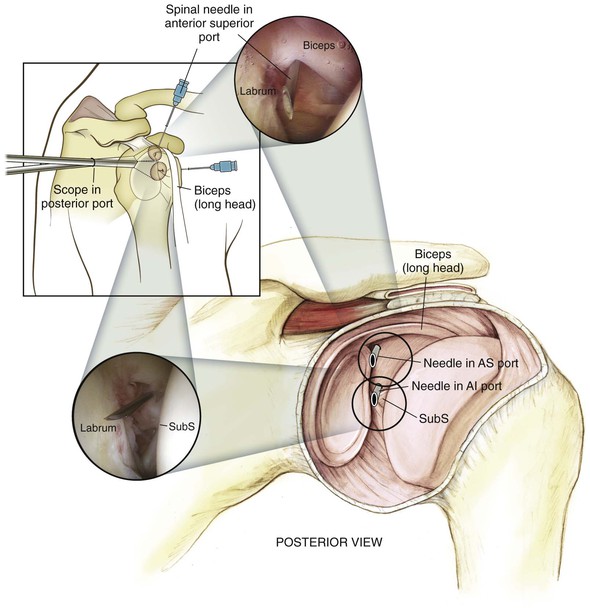
• Can be moved more medially for cases requiring distal clavicle resection
Use: It is the primary instrument portal
• This portal also can be used for visualization, especially to view the anterior glenoid and labrum (Fig. 2-54)