[level-membership-for-orthopaedics-category]CHAPTER 4
SHOULDER
SELECTED MOVEMENTS

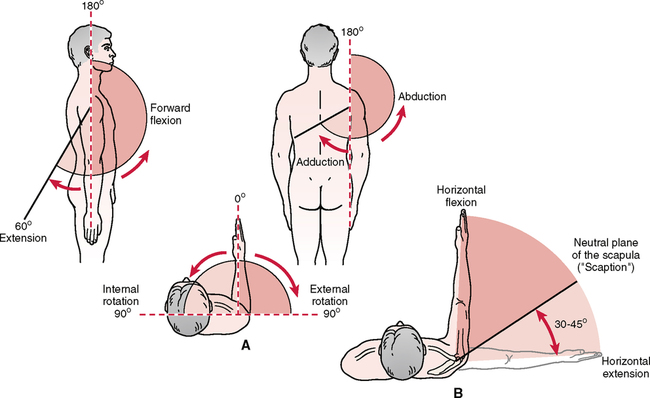
• Elevation in this position is sometimes called neutral elevation.
• Patients with weakness spontaneously choose this plane when elevating the arm.
• During elevation through scaption, scapulohumeral rhythm is similar to that of abduction, although there is greater individual variability.
• Often, movement into elevation is less painful in this position than elevation through abduction, when the glenohumeral joint is actually in extension, or elevation in forward flexion.
• Movement in the plane of the scapula puts less stress on the capsule and surrounding musculature and is the position in which most of the functions of daily activity are commonly performed.
INDICATIONS OF A POSITIVE TEST
When examining the movement of elevation through abduction, the examiner must take time to observe the scapulohumeral rhythm of the shoulder complex both anteriorly and posteriorly. During 180° of abduction, there is roughly a 2:1 ratio of movement of the humerus to the scapula, with 120° of movement occurring at the glenohumeral joint and 60° at the scapulothoracic joint. However, the examiner must keep in mind that a great deal of variability exists among individuals and may depend on the speed of movement; also, authors do not completely agree on the exact amounts of each movement.18–20
In the unstable shoulder, the scapulohumeral rhythm commonly is altered because of incorrect dynamic functioning of the scapular or humeral stabilizers or both. This may be related to incorrect arthrokinematics at the glenohumeral joint. Kibler21 pointed out that watching the movement of the scapula in both the ascending and descending phases of abduction is especially important. Commonly, weakness of the scapular control muscles is more evident during descent as many of the muscles are required to work eccentrically. An instability jog, hitch, or jump may occur when the patient loses control of the scapula.
• In the first phase of 30° of elevation through abduction, the scapula is said to be “setting.” This means that the scapula moves minimally during this stage—rotating slightly in, rotating slightly out, or not moving at all. Therefore, there is no 2:1 ratio of movement during this phase. The angle between the scapular spine and the clavicle also may increase up to 5° at the sternoclavicular and acromioclavicular joints when elevating the arm; however, this depends on whether the scapula moves during this phase.
• During the next 60° of upper extremity elevation (second phase), the scapula rotates about 20°, and the humerus elevates 40° with minimal protraction or elevation of the scapula. Therefore, there is a 2:1 ratio of scapulohumeral movement. During phase 2, the clavicle elevates because of the scapular rotation, but the clavicle still does not rotate or does so minimally.
• During the final 90° of motion (third phase), the 2:1 ratio of scapulohumeral movement continues and the angle between the scapular spine and the clavicle increases an additional 10°. Therefore, the scapula continues to rotate and now begins to elevate. The amount of protraction continues to be minimal when the abduction movement is performed. During this stage, the clavicle rotates posteriorly 30° to 50° on a long axis and elevates up to a further 15°. Also during this final stage, the humerus laterally rotates 90° so that the greater tuberosity of the humerus avoids the acromion process.
• During the second and third phases, rotation of the scapula (total, 60°) is possible because of the 20° of motion at the acromioclavicular joint and 40° at the sternoclavicular joint.
• When the test is done in this fashion, the examiner must be aware that the range measured is not actually that of the glenohumeral joint alone. In fact, much of the range is gained by winging the scapula, or protraction of the scapula so when the patient does the movement, the examiner should watch for movement in the scapula. As soon as the scapula begins to move, it is usually the end of glenohumeral rotation.
• With tight medial glenohumeral motion, greater winging and protraction of the scapula occur.
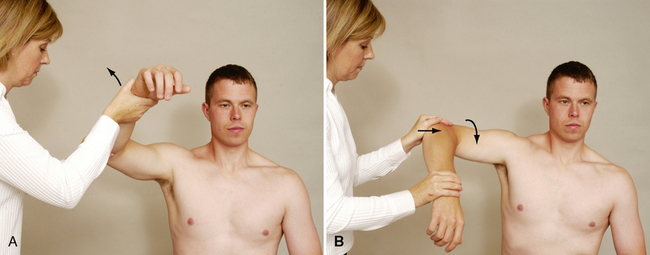
• If the patient can abduct to 90°, it is often easier to measure medial rotation from this positon.
• Measurement may also be taken by measuring the height of the patient’s radial styloid process as it reaches up the back. This eliminates variability in thumb position.
• Care must be taken when applying overpressure with this movement, because it could lead to anterior subluxation/dislocation of the glenohumeral joint, especially in individuals with recurrent dislocation problems.
• It is important to compare medial and lateral rotation, especially in active people who use their dominant arm at extremes of motion and under high load situations. The examiner should note any glenohumeral internal (medial) rotation deficit (GIRD), which is the difference in medial rotation between the patient’s two shoulders. Normally, the difference should be within 20°. This may also be compared with the glenohumeral external (lateral) rotation gain (GERG). If the GIRD/GERG ratio is greater than 1, the patient will often develop shoulder problems.
Horizontal Adduction/Cross Flexion
• To assess glenohumeral horizontal adduction instead of total shoulder horizontal adduction, the patient’s scapula can be stabilized into scapular retraction and the patient’s shoulder horizontally adducted. Alternatively, the clinician can assess when the scapula begins to move during the horizontal adduction motion. Movement of the scapula in either case indicates the end of glenohumeral motion and the beginning of scapulothoracic motion.
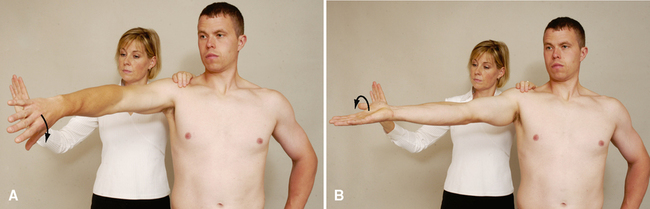
Scapular Retraction and Protraction
INDICATIONS OF A POSITIVE TEST
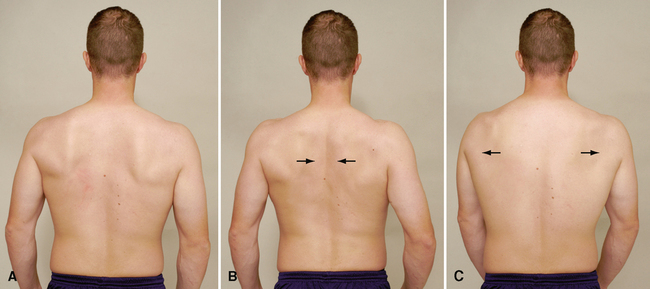
Scapular retraction. Normally, the medial borders of the scapulae remain parallel to the spine but move toward the spine with the soft tissue bunching up between them. Ideally, the patient is able to do this movement without excessive contraction of the upper trapezius muscles.
Scapular protraction. Normally, the scapulae move away from the midline; the inferior angle of the scapula commonly moves laterally more than the superior angle, resulting in some lateral rotation of the inferior angle. Commonly the two scapulae are tested simultaneously so that the examiner can visualize the difference between the two shoulders. A difference between the two sides indicates a positive test result.
• If the serratus anterior muscle is weak or paralyzed, the scapula “wings” away from the thorax on its medial border. The serratus anterior also assists upward rotation of the scapula during abduction. Therefore, injury to the muscle (serratus anterior) or its nerve (long thoracic nerve) may limit abduction.
• Similarly, weakness of the trapezius muscle, especially the lower part, can alter scapular mechanics, resulting in anterior secondary impingement.
• The protraction/retraction cycle may cause a clicking or snapping near the inferior angle or supramedial corner, a condition sometimes called a “snapping scapula,” which is caused by the scapula rubbing over the underlying ribs.

• Often the dominant shoulder shows greater restriction than the nondominant shoulder, even in the absence of a pathological condition. An exception would be individuals who continually use their arms at the extremes of motion (e.g., baseball pitchers). Because of the extra ROM developed over time doing the activity, the dominant arm may show greater ROM. However, the examiner must always be aware that shoulder movements include movements of the scapula and clavicle, as well as the glenohumeral joint. Many glenohumeral joint problems actually are scapular muscle control problems, which may secondarily lead to glenohumeral joint problems, especially in people under 40 years of age.
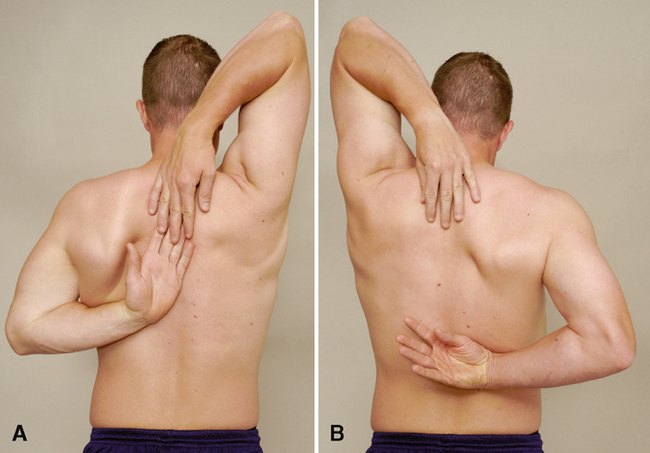
• The scapular reach test (neck and back) is a similar test in which the patient does medial rotation and adduction (back reach) of both arms at the same time, then lateral rotation and adduction (neck reach) of both arms at the same time. By having the patient do the combined movements, the examiner gets some idea of the individual’s functional capacity and can easily see differences between the two sides. (See Figure 5-29 in Magee DJ: Orthopedic Physical Assessment, ed. 5.)

• Passive movements may reveal the presence of a capsular pattern. The end feel of capsular tightness is different from the tissue stretch end feel or muscle tightness. Capsular tightness has a more hard and elastic feel to it, and it usually occurs earlier in the ROM.
• If unsure of the end feel, the examiner can have the patient contract the muscles acting in the opposite direction 10% to 20% of the maximum voluntary contraction (MVC) and then relax. The examiner then attempts to move the limb farther into range. If the range increases, the problem was muscular, not capsular.
POSTERIOR CAPSULAR TIGHTNESS TEST 


Flexion. The examiner places the palm of one hand on the anterior distal humerus to provide resistance near the elbow and uses the other hand to support the patient’s hand at the wrist.
Extension. The examiner places the palm of one hand on the posterior distal humerus to provide resistance near the elbow and uses the other hand to support the patient’s hand at the wrist.
Abduction. The examiner places the palm of one hand on the lateral distal humerus to provide resistance near the elbow and uses the other hand to support the patient’s hand at the wrist.
Adduction. The examiner places the palm of one hand on the medial distal humerus to provide resistance near the elbow and uses the other hand to support the patient’s hand at the wrist.
Medial rotation. The examiner places the palm of one hand on the distal forearm at the palmar aspect of the wrist to provide resistance, and the other hand just above the elbow.
Lateral rotation. The examiner places the palm of one hand on the distal forearm at the posterior aspect of the wrist to provide resistance and the other hand just above the elbow.
Elbow flexion. The examiner places the palm of one hand near the anterior wrist to provide resistance and uses the other hand to support the elbow.
Elbow extension. The examiner places the palm of one hand near the posterior wrist to provide resistance and uses the other hand to support the elbow.
• The disadvantage of testing shoulder isometrics with the patient in the supine position is that the examiner cannot observe the stabilization of the scapula during the testing. Normally, the scapula should not move during isometric testing. Scapular protraction, winging, or tilting during isometric testing indicates weakness of the scapular control muscles.
• Although all the muscles around the shoulder can be tested with the patient in the supine lying position, some recommend testing the muscles in more than one position (e.g., different amounts of abduction or forward flexion) to determine the mechanical effect of the contraction in different situations.
• If the patient history includes a complaint of pain in one or more positions, these positions also should be tested. If the initial position causes pain, other positions (e.g., position of injury, position of mechanical advantage) may be tried to further differentiate the specific contractile tissue that has been injured.
• The relative percentages for isometric testing will be altered if tests are performed at faster speeds and in different planes.
• If the patient history includes a complaint that concentric, eccentric, or econcentric (biceps and triceps) movements are painful or cause symptoms, these movements should be tested with loading or no loading as required.
• When testing isometric elbow flexion, the examiner should watch for the possibility of a third-degree strain (rupture) of the long head of the biceps tendon (“Popeye muscle”).
SPECIAL TESTS FOR ANTERIOR GLENOHUMERAL INSTABILITY27–37
General Information
Suspected Injury
• Unidirectional anterior instability.
• If the instability is the result of anterior dislocation or subluxation, injuries that may be present include a Hill-Sachs lesion, fracture of the anterior glenoid rim, or a Bankart lesion.
• Incorrect forward head posture, with rounded shoulders and protracted scapulae.
• Any of the peripheral nerves arising from the brachial plexus could be compromised. Damage can range from minor numbness or tingling to complete palsy of the nerve. The axillary nerve is especially susceptible.
• Anterior laxity often is accompanied by damage to the labrum, glenoid, anterior capsule, and/or brachial plexus.
• Vascular damage can occur with a shoulder dislocation. The brachial artery may be injured as it runs through the anterior shoulder complex.
Epidemiology and Demographics
Athletes who play overhead sports (e.g., tennis, volleyball, baseball) and patients with a history of dislocations or subluxations are more likely to have anterior shoulder instability. Several factors make the younger athlete more susceptible to anterior shoulder instability, such as poor technique and inadequate strength. Some researchers speculate that, in addition, adolescents’ immature collagen makeup makes them more susceptible to anterior shoulder instability and laxity.37
A wide array of incidences has been proposed in studies on anterior shoulder instability. Most patients initially dislocate the shoulder in their 20s or 30s, and 85% to 95% of dislocations in the shoulder are anterior. One fourth of all patients with dislocations have a family history of the same problem. The patient’s age at the time of dislocation has a significant impact on the recurrence rate. Reported recurrence rates in patients younger than age 20 vary from 70% to 100%.37
Relevant Signs and Symptoms
Translational Instability
• The patient may complain of generalized or anterior shoulder pain that can radiate down into the deltoid region of the shoulder, especially when the arm is above shoulder height.
• The patient may also complain of weakness in the shoulder that may be accompanied by clicking or grinding with shoulder motion.
• The patient often has a subjective feeling of instability, dislocation, or apprehension.
• The patient may complain that the shoulder does not “feel right,” especially when it is loaded above shoulder height.
• The results of unloaded active and passive movement and/or resisted isometric testing in neutral may be normal.
• Sensory loss, numbness or tingling, weakness, or complete palsy within a peripheral nerve distribution may be present in some cases.
• Coldness or weakness may be present if the vascular structures are compromised through the brachial region.
End-Range Instability
• Severe pain and restricted ROM are noted with dislocation.
• Severe muscle spasm may be present.
• The arm is held in 20º of abduction.
• Loss of shoulder roundness is seen.
• The humeral head may be palpated in the axilla.
• Once the dislocation has been reduced or if it has previously subluxed, apprehension predominates over pain.
• In individuals under age 35, anterior shoulder instability is commonly associated with scapular instability and a tight posterior capsule, both of which must be addressed for successful treatment.
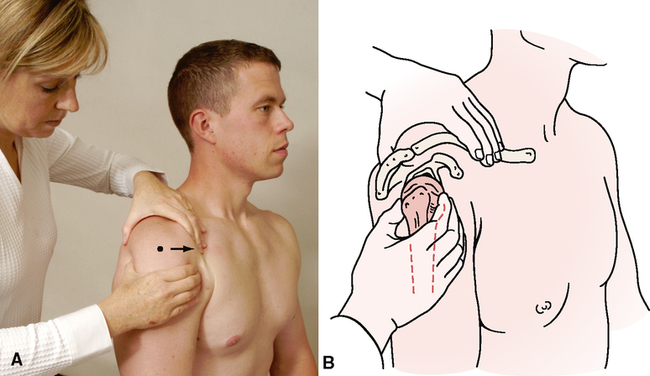
LOAD AND SHIFT TEST—ANTERIOR22,38–49 
• Generalized shoulder pain may be present that can radiate down into the deltoid region of the shoulder on testing.
• The patient commonly complains of weakness in the shoulder and may complain of clicking or grinding with shoulder motion.
• Neural irritation may occur in conjunction with shoulder instability. Sensory loss, numbness or tingling, weakness, or complete palsy within a peripheral nerve distribution may be seen.

INDICATIONS OF A POSITIVE TEST
Translation of 25% of the humeral head diameter or less anteriorly from the neutral position is considered normal. Hawkins and Mohtadi39 proposed a three-grade system of anterior translation. Normally, the head translates 0 to 25% of the diameter of the humeral head. Up to 50% of humeral head translation, with the head riding up to the glenoid rim and spontaneous reduction, is considered a grade I anterior translation. In a grade II anterior translation, the humeral head has more than 50% translation, and the head feels as though it is riding over the glenoid rim, but it spontaneously reduces. Grade III is a dislocation with no spontaneous reduction.
• Normally, the head of the humerus should translate anteriorly 0% to 25% of the diameter of the humeral head. The head of the humerus should translate posteriorly equal if not more than the anterior translation (25% to 50% of the diameter of the humerus). (Authors vary with regard to the amount of movement possible.)
• The load and shift test is designed to test for clinical symptoms more than any particular pathological condition. Many types of pathological conditions can result in instability of the shoulder. The load and shift test can be used as an assessment tool for both multidirectional and unidirectional instability. Multidirectional instability usually is the result of a genetic predisposition to laxity in the joints. Unidirectional instability is the result of trauma or repetitive use. Shoulder dislocations/subluxations/labral tears (type II instability) and general joint laxity (type I instability) are examples of pathological conditions that can be detected with this test.
• It is important to note that a positive test result is not specific for any one pathological condition; rather, it helps to guide the clinician in the reasoning process. Instability may be a contributing factor in the development of the ultimate pathological condition. Other factors that may contribute to instability include muscle weakness of the rotator cuff and/or weakness of the scapular control muscles.
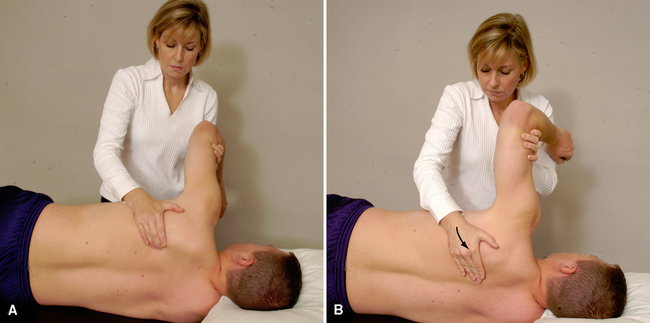
CRANK APPREHENSION TEST (RELOCATION TEST)27–30,36,41,50–61 
• If the shoulder has not been reduced, the patient will be in pain, will be supporting the arm, and will be hesitant to move it.
• If the shoulder has been reduced, the patient may have a generalized ache or pain that may radiate down into the deltoid region of the shoulder.
• Weakness in the shoulder may be noted, and the patient may complain of clicking or grinding with shoulder motion.
• Neural irritation is not uncommon in conjunction with shoulder instability. Sensory loss, numbness or tingling, weakness, or complete palsy within a peripheral nerve distribution (usually the axillary nerve) may be seen.
• If brachial vessels have been compromised, the patient may complain of weakness, coldness, or heaviness in the hand and arm.
• The patient often has a subjective feeling of instability, dislocation, or apprehension in the shoulder (especially with lateral rotation).
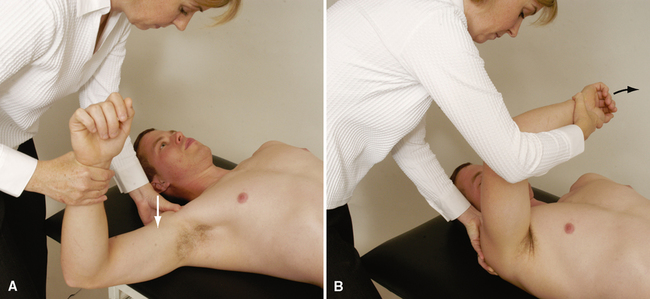
Step 1—the crank test. The examiner places one hand beneath the elbow to support the upper extremity. The other hand grasps the wrist and is responsible for movement of the shoulder into lateral rotation. The examiner flexes the elbow to 90°, abducts the arm to 90°, and laterally rotates the shoulder slowly, watching for apprehension. The shoulder is laterally rotated as far as possible. The hand supporting the elbow then is moved to the anterior aspect of the humeral head. The examiner should maintain the amount of lateral rotation without releasing pressure.
Step 2—the relocation test. The examiner applies a posterior stress to the humeral head and assesses whether the patient loses the apprehension, the pain decreases, and further lateral rotation is possible before the apprehension returns. This relocation sometimes is referred to as the Fowler sign or Fowler test or the Jobe relocation test.39,56 The hand pressure on the humeral head is removed, and symptoms are reassessed. For most patients, lateral rotation should be released before the posterior stress is released.

INDICATIONS OF A POSITIVE TEST
Apprehension test. A positive test result is indicated if the patient becomes apprehensive as the arm is laterally rotated and begins to contract the muscles to stop the lateral rotation (apprehension predominates). The patient may say that the feeling resembles what it felt like when the shoulder was dislocated.
Relocation test. The patient’s apprehension in the laterally rotated position disappears with the posterior translation. The examiner may find that lateral rotation will increase and apprehension will return as the lateral rotation increases. The test result is considered positive if pain decreases during the relocation maneuver, even if the patient felt no apprehension. If the arm is released (“surprise” test) in the new acquired range (step 3), pain and forward translation of the head are noted as positive test results.40,56,57
• If pain rather than apprehension increases on lateral rotation, the problem is more likely to be impingement, and impingement tests should be performed.
• Hawkins and Bokor58 state that the examiner should note the amount of lateral rotation present when the patient becomes apprehensive.
• With the relocation test, lateral rotation should be released before the posterior stress is released.
• If the patient’s symptoms decrease or are eliminated during the relocation test, the diagnosis is glenohumeral instability, subluxation, dislocation, or impingement.
• If apprehension predominates during the crank test and disappears with the relocation test, the diagnosis is glenohumeral instability, subluxation, or dislocation.
• If pain predominates during the crank test and disappears with the relocation test, the diagnosis is pseudolaxity or anterior instability at either the glenohumeral joint or the scapulothoracic joint, with secondary impingement, or a posterior labral lesion.
• Kvitne and Jobe59 advocate applying a mild, anteriorly directed force to the posterior humeral head when it is in the test position to see whether apprehension or pain increases. An increase in posterior pain may indicate a posterior internal impingement.
• Hamner et al60 have suggested that if a posterior internal impingement is suspected, the relocation test should be done in 100° to 120° of abduction.
• In patients with a primary impingement, the relocation test does not alter the pain. A decrease in posterior pain when the relocation test is done posteriorly is a positive test result for posterior internal impingement.
• If the joint is normal, translation of the humeral head in the glenoid is less than with other tests, because the crank test takes the joint into the close packed position.
• If the arm is released (anterior release, or “surprise,” test) in the newly acquired range of the relocation test, a positive test result is indicated by pain and forward translation of the head.
• The release maneuver (surprise test) should be done with care, because it often causes apprehension and distrust in the patient, and it could cause a dislocation.40,56,57
• The pain that results from the release maneuver (surprise test) may be caused by anterior shoulder instability, a labral lesion (Bankart or SLAP lesion), or bicipital peritenonitis or tendinosus.40,56,57 Most often this pain is related to anterior instability, because it is temporarily produced by the anterior translation. The surprise test also has been reported to cause pain in older patients with a pathological condition of the rotator cuff and no instability.61
ROCKWOOD TEST (MODIFICATION OF THE CRANK TEST)62 

• It is imperative that this test be done slowly. If it is done too quickly, the humerus may dislocate, especially in patients who have had recurrent dislocations.
• The different positions of the arm are tested because different passive stabilizers of the shoulder come into play with changes in the angle of abduction.


SPECIAL TESTS FOR POSTERIOR GLENOHUMERAL INSTABILITY
Relevant Special Tests
Epidemiology and Demographics
Recurrent posterior instability of the glenohumeral joint is less common than anterior instability. The frequency of occurrence is less than 5% of shoulder dislocations in most series.63 Other studies report that the rate of incidence is 2% to 12% of all cases of shoulder instability.64
Relevant Signs and Symptoms
• The patient may complain of generalized or posterior shoulder pain that may radiate down into the deltoid region of the shoulder.
• The patient may complain of weakness in the shoulder that may be accompanied by clicking or grinding with shoulder motion.
• Neural irritation is not common with posterior shoulder instability.
• The patient often has subjective feelings of instability, dislocation, or apprehension.
• The patient may complain that the shoulder “doesn’t feel right,” especially when it is loaded above shoulder height.
• The results of unloaded active and passive movement and resisted isometric testing may be normal.
Clinical Note/Caution
• Posterior dislocations of the glenohumeral joint can be easily missed, even on x-ray films. Therefore, it is important to test all active and passive movements and compare the two sides before doing the instability test. Limited rotation may indicate that the dislocation has not been reduced.
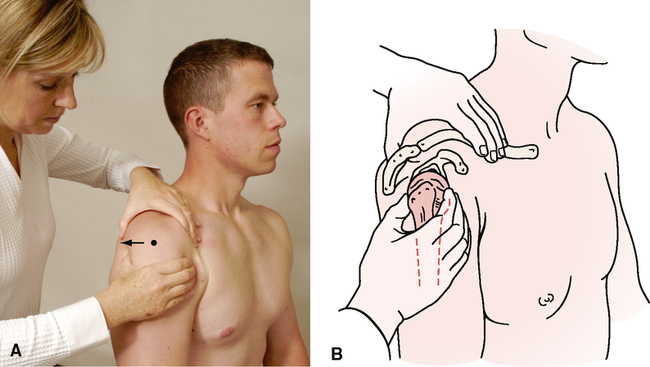
LOAD AND SHIFT TEST—POSTERIOR38–44,47–49,65 
INDICATIONS OF A POSITIVE TEST

• If the load is not applied to put the head in neutral position, the amount of movement found will not indicate the true amount of translation posteriorly, and the end feel will be altered.
• Normally, the head of the humerus should translate 25% to 50% of the diameter of the humeral head.
• Posterior translation of the humeral head is generally greater than anterior translation. (Authors vary on the amount of movement possible, but normally, posterior movement is never less than anterior movement.)
• The test also may be done with the patient in the supine-lying position. It is important to note that a positive test result is not specific for any one pathological condition; rather, it helps guide the clinician in the reasoning process.

• Cofield and Irving67 recommend medially rotating the forearm approximately 20º after the forward flexion and then pushing the elbow posteriorly to enhance the effect of the test.
• Care must be taken with this test, because it does not cause apprehension in the patient, but it may cause subluxation or dislocation.
POSTERIOR APPREHENSION OR STRESS TEST41,49,63,68,69 

• The test may also be performed with the arm in 90º of abduction.
• The test also may be done with the patient in the sitting position, but the scapula must be stabilized.
• It is important to note that a positive test result is not specific for any one pathological condition; rather, it helps guide the clinician in the reasoning process. Instability may be a contributing factor in the development of the ultimate pathological condition.
• Pagnani and Warren69 reported that a positive test result is more likely to be marked by pain than by apprehension. They reported that with atraumatic multidirectional (inferior) instability, the test result is negative.
SPECIAL TESTS FOR INFERIOR GLENOHUMERAL INSTABILITY
Relevant Special Tests
Epidemiology and Demographics
Athletes who play overhead sports (e.g., tennis, volleyball, baseball) and patients with a history of dislocations or subluxations are more likely to have multidirectional instability of the shoulder. Several factors make the younger athlete more susceptible to multidirectional shoulder instability. Younger athletes have a tendency to have poor shoulder mechanics (incorrect techniques) and inadequate strength. In addition, some researchers speculate that adolescents’ immature collagen makeup leaves them more susceptible to shoulder instability and laxity.37,70–77
Relevant Signs and Symptoms
• The patient may have subjective feelings of instability, dislocation, or apprehension.
• The patient may complain that the shoulder “doesn’t feel right,” especially when it is loaded above shoulder height.
• Test results with unloaded active and passive movement and resisted isometric testing may be normal.
Mechanism of Injury

INDICATIONS OF A POSITIVE TEST
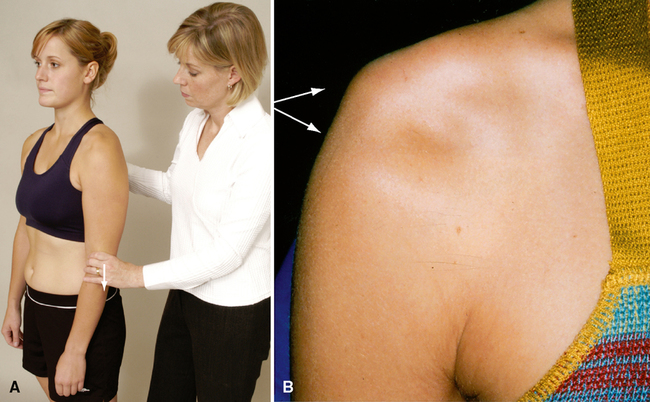
The presence of a sulcus under the acromion indicates inferior instability or glenohumeral laxity. The sulcus sign may be graded by measuring from the inferior margin of the acromion to the humeral heads (Table 4-1).
• Some researchers have reported that the best position for testing for inferior instability is at 20º to 50º of abduction with neutral rotation.48 Therefore, the examiner should consider testing more than one position. Depending on the history, the examiner should test the patient in the position in which the sensation of instability is reported


• The Feagin test is a modification of the sulcus test with the arm abducted to 90º instead of being at the patient’s side. Some authors consider the Feagin test the second part of the sulcus test.80
• This test position also puts more stress on the inferior glenohumeral ligament.
• Positive results on both the sulcus sign and the Feagin test point more decisively to multidirectional instability, rather than just laxity.
SPECIAL TESTS FOR IMPINGEMENT
Relevant Special Tests
Epidemiology and Demographics83
Neer has described three stages of impingement (Table 4-2).
Table 4-2
Neer’s Grades of Shoulder Impingement83
| Grade | Pathology | Symptoms | Range of Motion and Strength |
| Grade I | Subacromial bursitis/tendonitis |

Mechanism of Injury84–88
Anterior shoulder impingement. Regardless of its cause (e.g., pathological condition of the rotator cuff, bicipital paratenonitis/tendinosis, scapular or humeral instability, labral pathology), anterior shoulder impingement most commonly results when structures are compressed in the anterior aspect of the humerus between the head of the humerus and the coracoid process, under the acromion process and under the coracoacromial ligament. These injuries may be acute or degenerative. An acute injury produces a sudden onset of shoulder pain after a specific activity. The aggravating activity commonly is an overhead maneuver, such as throwing or painting. Trauma, such as a fall onto an outstretched hand (FOOSH injury), also can result in shoulder impingement. Because of the progressive nature of subacromial impingement, patients with degenerative-type impingement often complain of several bouts of shoulder pain over a number of years. Each subsequent episode generally is worse than the previous one. The patient often reports that the latest episode did not resolve and has increasing loss of ROM.
Posterior shoulder impingement. Posterior impingement occurs when the rotator cuff impinges against the posterosuperior edge of the glenoid when the arm is abducted, extended, and laterally rotated. The result is a “kissing” labral lesion posteriorly. The resulting impingement occurs between the rotator cuff and greater tuberosity on one side and the posterior glenoid and labrum on the other side. This type of impingement often accompanies anterior instability or pseudolaxity, and deltoid activity increases to compensate for weakened rotator cuff muscles.
RELIABILITY/SPECIFICITY/SENSITIVITY/COMPARISON89
| Validity | Interrater Reliability | Intrarater Reliability | Specificity | Sensitivity | |
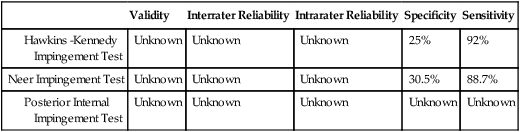
HAWKINS-KENNEDY IMPINGEMENT TEST87,89–99 

• The test also may be performed in different degrees of forward flexion (vertically “circling the shoulder”) or horizontal adduction (horizontally circling the shoulder).
• McFarland et al.96 described the coracoid impingement sign, which is the same as the Hawkins-Kennedy test but involves horizontally adducting the arm across the body 10° to 20° before doing the medial rotation. This is more likely to approximate the lesser tuberosity of the humerus and the coracoid process.
• The Yocum test is a modification of the Hawkins-Kennedy test in which the patient’s hand is placed on the opposite shoulder and the examiner elevates the elbow.97,98
• Park et al.99 found that combining tests gave better results. They found that the Hawkins-Kennedy test, the painful arc sign, and a positive result on the infraspinatus test gave the best probability of detecting impingement, whereas the painful arc sign, drop arm test, and infraspinatus test were best for detecting full-thickness rotator cuff tears.
NEER IMPINGEMENT TEST89,90,95,99–102 

INDICATIONS OF A POSITIVE TEST
A positive test result is indicated by an expression of pain on the patient’s face.
• A positive test result may indicate an overuse injury to the supraspinatus muscle and sometimes to the biceps tendon; these injuries often are associated with scapular control problems.
• If the test result is positive when the test is done with the arm laterally rotated, the examiner should check the acromioclavicular joint (acromioclavicular differentiation test).


SPECIAL TESTS FOR LABRAL TEARS OF THE GLENOHUMERAL JOINT
Relevant Special Tests
Note: Parentis et al.107 concluded that no one test can provide a definitive diagnosis of a labral lesion.
Epidemiology and Demographics
The most common cause of a labral tear is trauma from a dislocation. In addition, younger individuals are prone to labral injury with repetitive overhead motions, such as swimming, tennis, or throwing. Older people are more prone to degenerative lesions, which often are associated with poor vascular supply to the labral tissue.54,74,108,109
Relevant Signs and Symptoms
• Aching of the shoulder region
• A feeling of instability may be noted by the patient
• Clicking or popping with motion
• Catching in the shoulder with movement
• Weakness or pain (or both) with overhead motions
• Diffuse upper trapezius or thoracic pain (or both)
Clinical Note/Caution
• Diagnosis of a SLAP lesion is based primarily on the history. The special tests are used to verify the suspected involvement of the labrum. The tests themselves should not be the sole source of diagnosis; they must correlate with the patient’s subjective complaints.
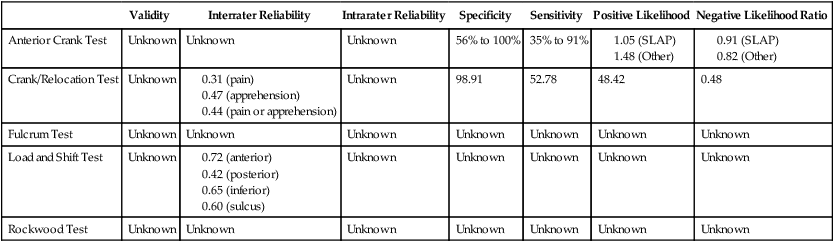
RELIABILITY/SPECIFICITY/SENSITIVITY COMPARISON27–29,110–112
| Active Compression Test of O’Brien | Anterior Slide Test | Biceps Load Test | Biceps Tension Test | Clunk Test | Labral Crank Test | SLAP Prehension Test | |
| Specificity | 31% to 55% | 84% to 91.5% | 96.6% | Unknown | Unknown | 56% to 100% | Unknown |
| Sensitivity | 47% to 54% | 8% to 78.4% | 89.7% | Unknown | Unknown | 46% to 91% | Unknown |

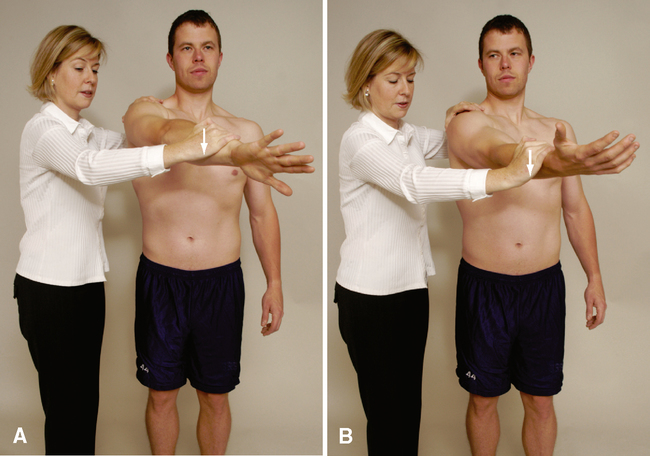
ACTIVE COMPRESSION TEST OF O’BRIEN29,30,32,53,102,103,110,111,113,114 




• Speed’s test should be done to rule out a biceps pathological condition.
• Because SLAP lesions may involve the long head of the biceps tendon, any test stressing the long head of the biceps could stress the superior labrum. Several similar tests are designed to stress both structures, such as the biceps load test, biceps tension test, SLAP prehension test, and labral crank test.


• The examiner may position the arm in different amounts of abduction (vertically circling the shoulder) and perform the test in each position. This stresses different parts of the labrum.
• Walsh117 reported that if the examiner follows the abduction maneuvers with horizontal adduction that relocates the humerus, a clunk or click may be heard, indicating a labral tear.




[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]CHAPTER 4
SHOULDER
SELECTED MOVEMENTS
• Elevation in this position is sometimes called neutral elevation.
• Patients with weakness spontaneously choose this plane when elevating the arm.
• During elevation through scaption, scapulohumeral rhythm is similar to that of abduction, although there is greater individual variability.
• Often, movement into elevation is less painful in this position than elevation through abduction, when the glenohumeral joint is actually in extension, or elevation in forward flexion.
• Movement in the plane of the scapula puts less stress on the capsule and surrounding musculature and is the position in which most of the functions of daily activity are commonly performed.
INDICATIONS OF A POSITIVE TEST
When examining the movement of elevation through abduction, the examiner must take time to observe the scapulohumeral rhythm of the shoulder complex both anteriorly and posteriorly. During 180° of abduction, there is roughly a 2:1 ratio of movement of the humerus to the scapula, with 120° of movement occurring at the glenohumeral joint and 60° at the scapulothoracic joint. However, the examiner must keep in mind that a great deal of variability exists among individuals and may depend on the speed of movement; also, authors do not completely agree on the exact amounts of each movement.18–20
In the unstable shoulder, the scapulohumeral rhythm commonly is altered because of incorrect dynamic functioning of the scapular or humeral stabilizers or both. This may be related to incorrect arthrokinematics at the glenohumeral joint. Kibler21 pointed out that watching the movement of the scapula in both the ascending and descending phases of abduction is especially important. Commonly, weakness of the scapular control muscles is more evident during descent as many of the muscles are required to work eccentrically. An instability jog, hitch, or jump may occur when the patient loses control of the scapula.
• In the first phase of 30° of elevation through abduction, the scapula is said to be “setting.” This means that the scapula moves minimally during this stage—rotating slightly in, rotating slightly out, or not moving at all. Therefore, there is no 2:1 ratio of movement during this phase. The angle between the scapular spine and the clavicle also may increase up to 5° at the sternoclavicular and acromioclavicular joints when elevating the arm; however, this depends on whether the scapula moves during this phase.
• During the next 60° of upper extremity elevation (second phase), the scapula rotates about 20°, and the humerus elevates 40° with minimal protraction or elevation of the scapula. Therefore, there is a 2:1 ratio of scapulohumeral movement. During phase 2, the clavicle elevates because of the scapular rotation, but the clavicle still does not rotate or does so minimally.
• During the final 90° of motion (third phase), the 2:1 ratio of scapulohumeral movement continues and the angle between the scapular spine and the clavicle increases an additional 10°. Therefore, the scapula continues to rotate and now begins to elevate. The amount of protraction continues to be minimal when the abduction movement is performed. During this stage, the clavicle rotates posteriorly 30° to 50° on a long axis and elevates up to a further 15°. Also during this final stage, the humerus laterally rotates 90° so that the greater tuberosity of the humerus avoids the acromion process.
• During the second and third phases, rotation of the scapula (total, 60°) is possible because of the 20° of motion at the acromioclavicular joint and 40° at the sternoclavicular joint.
• When the test is done in this fashion, the examiner must be aware that the range measured is not actually that of the glenohumeral joint alone. In fact, much of the range is gained by winging the scapula, or protraction of the scapula so when the patient does the movement, the examiner should watch for movement in the scapula. As soon as the scapula begins to move, it is usually the end of glenohumeral rotation.
• With tight medial glenohumeral motion, greater winging and protraction of the scapula occur.
• If the patient can abduct to 90°, it is often easier to measure medial rotation from this positon.
• Measurement may also be taken by measuring the height of the patient’s radial styloid process as it reaches up the back. This eliminates variability in thumb position.
• Care must be taken when applying overpressure with this movement, because it could lead to anterior subluxation/dislocation of the glenohumeral joint, especially in individuals with recurrent dislocation problems.
• It is important to compare medial and lateral rotation, especially in active people who use their dominant arm at extremes of motion and under high load situations. The examiner should note any glenohumeral internal (medial) rotation deficit (GIRD), which is the difference in medial rotation between the patient’s two shoulders. Normally, the difference should be within 20°. This may also be compared with the glenohumeral external (lateral) rotation gain (GERG). If the GIRD/GERG ratio is greater than 1, the patient will often develop shoulder problems.
Horizontal Adduction/Cross Flexion
• To assess glenohumeral horizontal adduction instead of total shoulder horizontal adduction, the patient’s scapula can be stabilized into scapular retraction and the patient’s shoulder horizontally adducted. Alternatively, the clinician can assess when the scapula begins to move during the horizontal adduction motion. Movement of the scapula in either case indicates the end of glenohumeral motion and the beginning of scapulothoracic motion.
Scapular Retraction and Protraction
INDICATIONS OF A POSITIVE TEST
Scapular retraction. Normally, the medial borders of the scapulae remain parallel to the spine but move toward the spine with the soft tissue bunching up between them. Ideally, the patient is able to do this movement without excessive contraction of the upper trapezius muscles.
Scapular protraction. Normally, the scapulae move away from the midline; the inferior angle of the scapula commonly moves laterally more than the superior angle, resulting in some lateral rotation of the inferior angle. Commonly the two scapulae are tested simultaneously so that the examiner can visualize the difference between the two shoulders. A difference between the two sides indicates a positive test result.
• If the serratus anterior muscle is weak or paralyzed, the scapula “wings” away from the thorax on its medial border. The serratus anterior also assists upward rotation of the scapula during abduction. Therefore, injury to the muscle (serratus anterior) or its nerve (long thoracic nerve) may limit abduction.
• Similarly, weakness of the trapezius muscle, especially the lower part, can alter scapular mechanics, resulting in anterior secondary impingement.
• The protraction/retraction cycle may cause a clicking or snapping near the inferior angle or supramedial corner, a condition sometimes called a “snapping scapula,” which is caused by the scapula rubbing over the underlying ribs.
• Often the dominant shoulder shows greater restriction than the nondominant shoulder, even in the absence of a pathological condition. An exception would be individuals who continually use their arms at the extremes of motion (e.g., baseball pitchers). Because of the extra ROM developed over time doing the activity, the dominant arm may show greater ROM. However, the examiner must always be aware that shoulder movements include movements of the scapula and clavicle, as well as the glenohumeral joint. Many glenohumeral joint problems actually are scapular muscle control problems, which may secondarily lead to glenohumeral joint problems, especially in people under 40 years of age.
• The scapular reach test (neck and back) is a similar test in which the patient does medial rotation and adduction (back reach) of both arms at the same time, then lateral rotation and adduction (neck reach) of both arms at the same time. By having the patient do the combined movements, the examiner gets some idea of the individual’s functional capacity and can easily see differences between the two sides. (See Figure 5-29 in Magee DJ: Orthopedic Physical Assessment, ed. 5.)
• Passive movements may reveal the presence of a capsular pattern. The end feel of capsular tightness is different from the tissue stretch end feel or muscle tightness. Capsular tightness has a more hard and elastic feel to it, and it usually occurs earlier in the ROM.
• If unsure of the end feel, the examiner can have the patient contract the muscles acting in the opposite direction 10% to 20% of the maximum voluntary contraction (MVC) and then relax. The examiner then attempts to move the limb farther into range. If the range increases, the problem was muscular, not capsular.
POSTERIOR CAPSULAR TIGHTNESS TEST
Flexion. The examiner places the palm of one hand on the anterior distal humerus to provide resistance near the elbow and uses the other hand to support the patient’s hand at the wrist.
Extension. The examiner places the palm of one hand on the posterior distal humerus to provide resistance near the elbow and uses the other hand to support the patient’s hand at the wrist.
Abduction. The examiner places the palm of one hand on the lateral distal humerus to provide resistance near the elbow and uses the other hand to support the patient’s hand at the wrist.
Adduction. The examiner places the palm of one hand on the medial distal humerus to provide resistance near the elbow and uses the other hand to support the patient’s hand at the wrist.
Medial rotation. The examiner places the palm of one hand on the distal forearm at the palmar aspect of the wrist to provide resistance, and the other hand just above the elbow.
Lateral rotation. The examiner places the palm of one hand on the distal forearm at the posterior aspect of the wrist to provide resistance and the other hand just above the elbow.
Elbow flexion. The examiner places the palm of one hand near the anterior wrist to provide resistance and uses the other hand to support the elbow.
Elbow extension. The examiner places the palm of one hand near the posterior wrist to provide resistance and uses the other hand to support the elbow.
• The disadvantage of testing shoulder isometrics with the patient in the supine position is that the examiner cannot observe the stabilization of the scapula during the testing. Normally, the scapula should not move during isometric testing. Scapular protraction, winging, or tilting during isometric testing indicates weakness of the scapular control muscles.
• Although all the muscles around the shoulder can be tested with the patient in the supine lying position, some recommend testing the muscles in more than one position (e.g., different amounts of abduction or forward flexion) to determine the mechanical effect of the contraction in different situations.
• If the patient history includes a complaint of pain in one or more positions, these positions also should be tested. If the initial position causes pain, other positions (e.g., position of injury, position of mechanical advantage) may be tried to further differentiate the specific contractile tissue that has been injured.
• The relative percentages for isometric testing will be altered if tests are performed at faster speeds and in different planes.
• If the patient history includes a complaint that concentric, eccentric, or econcentric (biceps and triceps) movements are painful or cause symptoms, these movements should be tested with loading or no loading as required.
• When testing isometric elbow flexion, the examiner should watch for the possibility of a third-degree strain (rupture) of the long head of the biceps tendon (“Popeye muscle”).
SPECIAL TESTS FOR ANTERIOR GLENOHUMERAL INSTABILITY27–37
General Information
[/not-level-membership-for-orthopaedics-category]
