[level-membership-for-opthalmology-category]22.1
Retinal Capillary Hemangioma
Clinical Features:
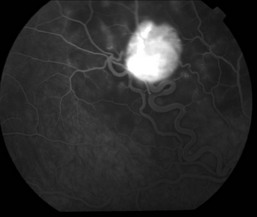
These lesions can affect both the retina and optic nerve. They start out small and can gradually enlarge with the possibility of intraretinal and subretinal exudation that can involve the macula and affect visual acuity. They have characteristic tortuous and dilated feeding and draining arteries and veins (Fig. 22.1.1 and Fig. 22.1.2), respectively. Multiple and bilateral lesions are common in the setting of Von Hippel–Lindau disease.
OCT Features:
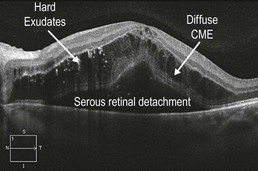
Smaller lesions are seen as a well-circumscribed bulbous deformity obscuring the layers of the retina (Fig. 22.1.3), whereas larger lesions have a hyper-reflective inner surface with deeper structures obscured by shadowing (Fig. 22.1.4). In larger lesions with surrounding exudation, there can be cystic cavities within the retina surrounding the retinal angioma (Fig. 22.1.5). There can be associated intraretinal fluid or even a serous retinal detachment within the macula (Fig. 22.1.6).
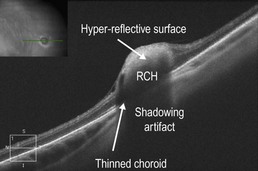
Figure 22.1.3 OCT of a smaller peripheral RCH shows a well-circumscribed area of hyper-reflectivity corresponding to the lesion that focally replaces the retina. The underlying choroid appears thin, though there is significant shadowing artifact.
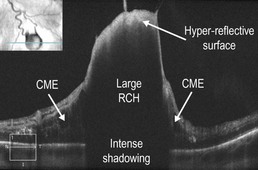
Figure 22.1.4 OCT of a large RCH shows hyper-reflectivity of the inner surface with a dense shadowing artifact of the central and outer portions. There is mild CME on the edges.
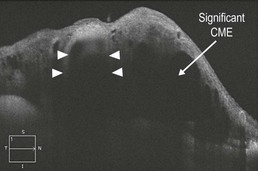
Figure 22.1.5 OCT of a large retinal capillary hemangioma (corresponding to Figure 22.1.1) shows significant hyper-reflectivity of the inner surface (between arrowheads). There is also significant surrounding intraretinal fluid or CME.
Ancillary Testing:
Serial color, red free photos and ultrasonography can be helpful in tracking changes in lesion size over time. Fluorescein angiography can also be useful in assisting with the diagnosis (Fig. 22.1.2), if it is in question.
[/level-membership-for-opthalmology-category][not-level-membership-for-opthalmology-category]22.1
Retinal Capillary Hemangioma
Clinical Features:
These lesions can affect both the retina and optic nerve. They start out small and can gradually enlarge with the possibility of intraretinal and subretinal exudation that can involve the macula and affect visual acuity. They have characteristic tortuous and dilated feeding and draining arteries and veins (Fig. 22.1.1 and Fig. 22.1.2), respectively. Multiple and bilateral lesions are common in the setting of Von Hippel–Lindau disease.
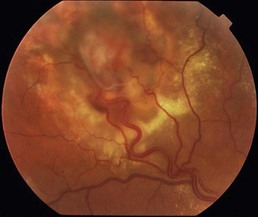
Figure 22.1.1 Color fundus photograph of a retinal capillary hemangioma shows a pink-colored lesion just superior to the macula with dilated and tortuous feeding vessels. There is surrounding subretinal fluid and exudation present.
[/not-level-membership-for-opthalmology-category]
