[level-membership-for-pediatrics-category]
Chapter 213 Relapsing Fever (Borrelia)
Epidemiology
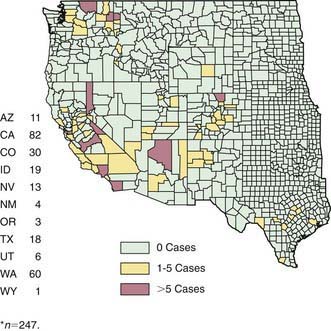
Ornithodoros ticks, which transmit endemic relapsing fever, are distributed worldwide, including the western USA, prefer warm, humid environments and high altitudes and are found in rodent burrows, caves, and other nesting sites (Fig. 213-1). Rodents (e.g., squirrels, chipmunks) are the principal reservoirs. Infected ticks gain access to human dwellings on the rodent host. Human contact is often unnoticed because these soft ticks have a painless bite and detach immediately after a short blood meal.
Butler TC. Relapsing fever: new lessons about antibiotic action. Ann Intern Med. 1985;102:397-399.
Centers for Disease Control and Prevention. Tickborne relapsing fever outbreak after a family gathering—New Mexico, August 2002. MMWR Morb Mortal Wkly Rep. 2003;52:809-812.
Dworkin MS, Schwan TG, Anderson DEJr, et al. Tick-borne relapsing fever. Infect Dis Clin North Am. 2008;22:449-468. viii
Fritz CL, Bronson LR, Smith CR, et al. Isolation and characterization of Borrelia hermsii associated with two foci of tick-borne relapsing fever in California. J Clin Microbiol. 2004;42:1123-1128.
Grosskinsky S, Schott M, Brenner C, et al. Borrelia recurrentis employs a novel multifunctional surface protein with anti–complement, anti opsonic and invasive potential to escape innate immunity. PloS One. 2009;4:e4858.
Hasin T, Davidovitch N, Cohen R, et al. Postexposure treatment with doxycycline for the prevention of tick-borne relapsing fever. N Engl J Med. 2006;355:148-154.
Larsson C, Bergstrom S. A novel and simple method for laboratory diagnosis of relapsing fever Borreliosis. Open Microbiol J. 2008;2:10-12.
Schwan TG, Policastro PF, Miller Z, et al. Tick-borne relapsing fever caused by Borrelia hermsii, Montana. Emerg Infect Dis. 2003;9:1151-1154.
Vial L, Diatta G, Tall A, et al. Incidence of tick-borne relapsing fever in west Africa: longitudinal study. Lancet. 2006;368:37-43.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
Chapter 213 Relapsing Fever (Borrelia)
Epidemiology
Ornithodoros ticks, which transmit endemic relapsing fever, are distributed worldwide, including the western USA, prefer warm, humid environments and high altitudes and are found in rodent burrows, caves, and other nesting sites (Fig. 213-1). Rodents (e.g., squirrels, chipmunks) are the principal reservoirs. Infected ticks gain access to human dwellings on the rodent host. Human contact is often unnoticed because these soft ticks have a painless bite and detach immediately after a short blood meal.
