Chapter 62 Rare Coagulation Factor Deficiencies
Table 62-2 Treatment Considerations for Rare Coagulation Factor Deficiencies
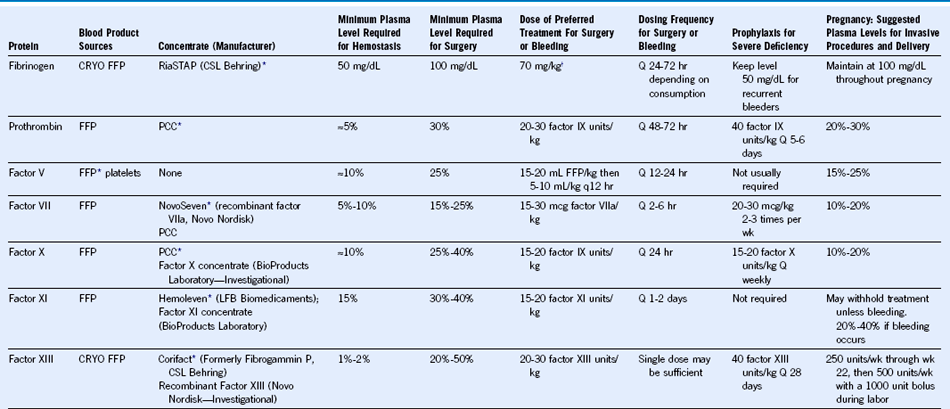
FFP, Fresh frozen plasma; CRYO, cryoprecipitate; PCC, prothrombin complex concentrate.
Published on 04/03/2015 by admin
Filed under Hematology, Oncology and Palliative Medicine
Last modified 22/04/2025
Print this pageChapter 62 Rare Coagulation Factor Deficiencies
Table 62-2 Treatment Considerations for Rare Coagulation Factor Deficiencies
FFP, Fresh frozen plasma; CRYO, cryoprecipitate; PCC, prothrombin complex concentrate.