[level-membership-for-hematology-oncology-and-palliative-medicine-category]
Chapter 62 Rare Coagulation Factor Deficiencies
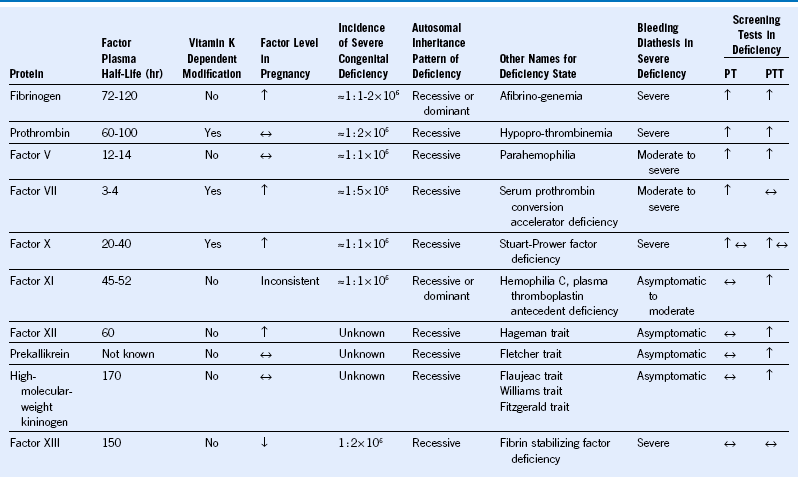
Table 62-2 Treatment Considerations for Rare Coagulation Factor Deficiencies
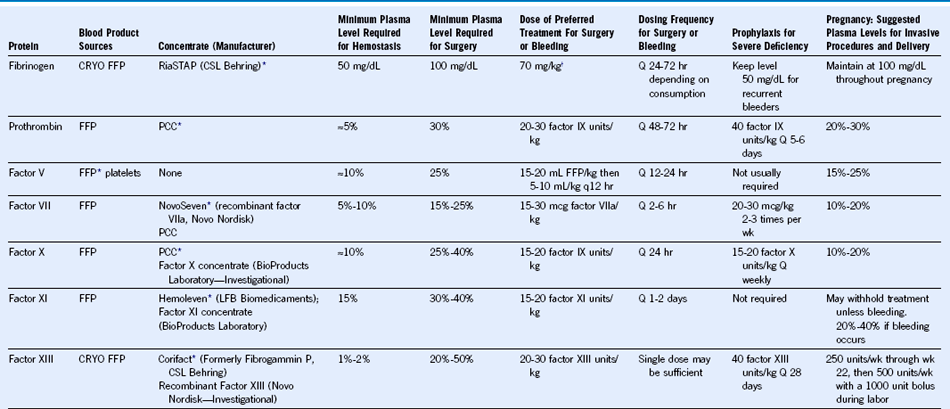
FFP, Fresh frozen plasma; CRYO, cryoprecipitate; PCC, prothrombin complex concentrate.
[/level-membership-for-hematology-oncology-and-palliative-medicine-category][not-level-membership-for-hematology-oncology-and-palliative-medicine-category]
Chapter 62 Rare Coagulation Factor Deficiencies
Table 62-2 Treatment Considerations for Rare Coagulation Factor Deficiencies
FFP, Fresh frozen plasma; CRYO, cryoprecipitate; PCC, prothrombin complex concentrate.
