[level-membership-for-radiology-category] Vessels within zone may appear normal (no mass effect)
Usually low density on NECT and CECT
May have mixed hypervascular and hypovascular foci
• Region of radiation damage that is hypodense on portal venous phase may become hyperdense with prolonged enhancement on delayed phase
Due to ↓ vascular perfusion, ↓ hepatic venous drainage, and subsequent stasis of contrast medium
• MR, especially T1WI with in- and opposed-phase GRE, is best means of distinguishing RILD from steatosis
TOP DIFFERENTIAL DIAGNOSES
• Focal steatosis
• Hepatic infarction
PATHOLOGY
• Patients receiving single 1,200-rad dose of external beam radiation or a 4,000 to 5,500-rad fractionated dose over 6 weeks can develop RILD
• Hepatic arterial administration of yttrium-90 glass microspheres
Emit radiation to perfused hepatic area persisting for 64-hour half-life
CLINICAL ISSUES
• Complete clinical recovery typically seen within 60 days, but there may be permanent hepatocyte loss, fat deposition, fibrosis, and obliteration of central veins
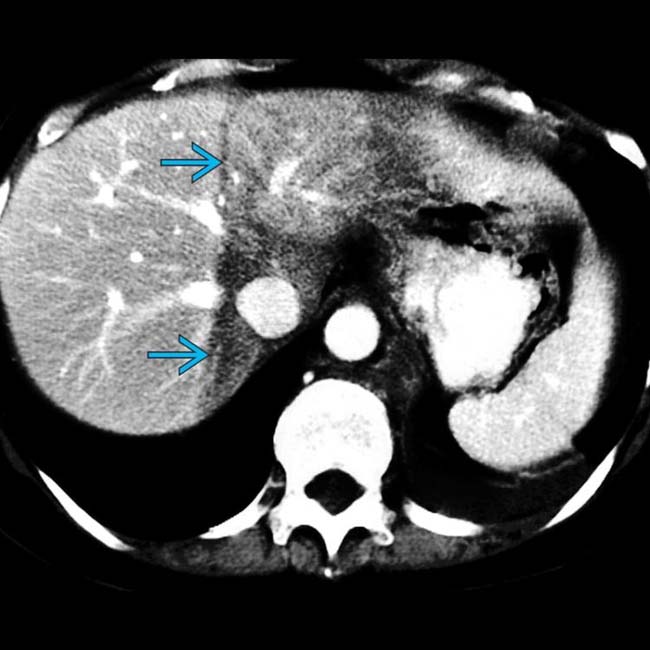
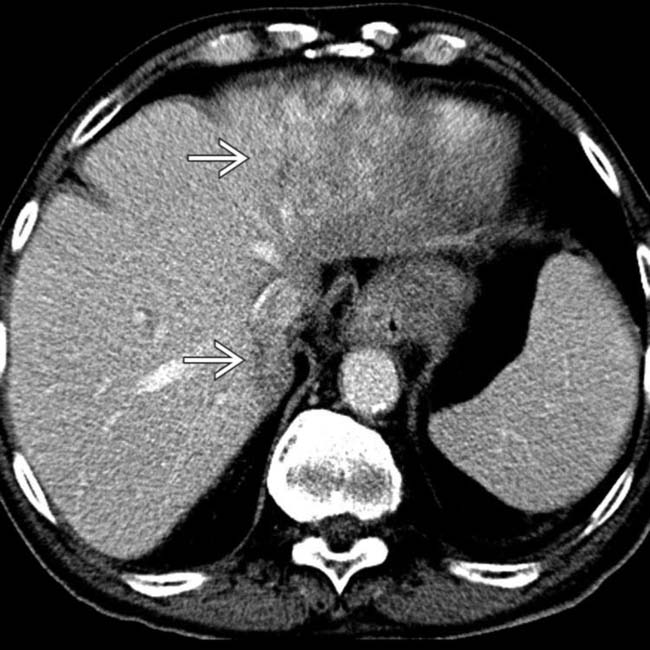
(Left) Axial CECT shows a vertically oriented zone of low attenuation extending from the cranial to caudal aspect of the liver in a straight line , following external radiation therapy for lymphoma.
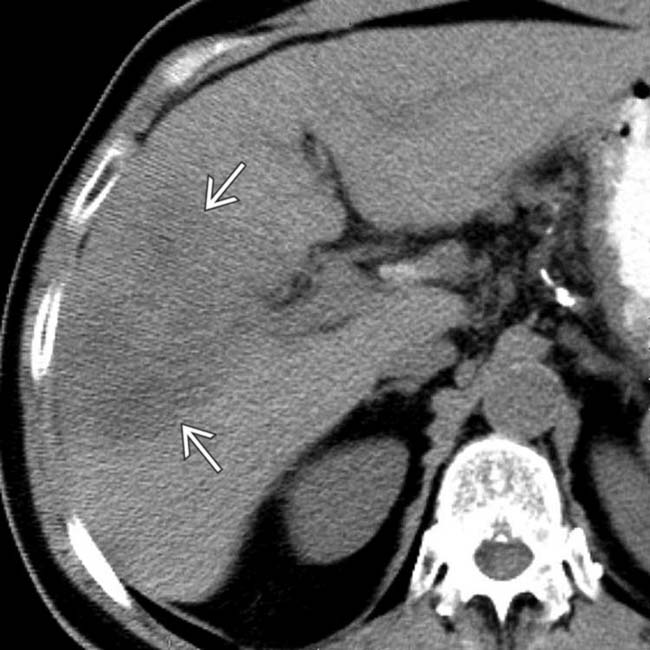
(Right) Axial CECT shows a straight line of demarcation of damaged liver in the left lobe due to external radiation therapy for esophageal carcinoma. Note the normal appearance of the left hepatic vein within the zone of radiation-induced liver disease (RILD).
(Left) Axial CECT shows decreased attenuation within the posterior segments of the liver, with a straight line of demarcation corresponding to the segments that had received yttrium-90 microsphere embolization for hepatocellular carcinoma (HCC). Note the normal appearance of the posterior right portal vein within the damaged liver.
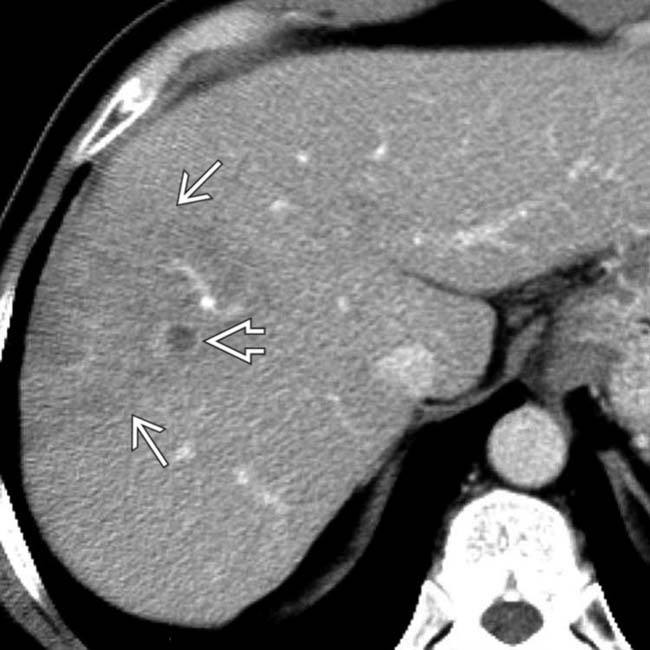
(Right) CECT section from the same case shows viable satellite foci of HCC within the untreated anterior segments of liver .
TERMINOLOGY
Abbreviations
• Radiation-induced liver disease (RILD)
Definitions
• Syndrome characterized by development of anicteric ascites ∼ 2 weeks to 4 months after hepatic irradiation
• Form of venoocclusive disease due to fibrous obliteration of terminal hepatic venules → postsinusoidal obstruction
IMAGING
General Features
• Best diagnostic clue
Sharp line of demarcation between normal and abnormal parenchyma corresponds to radiation port or vascular distribution of yttrium-90 microspheres
CT Findings
• NECT
Sharply defined band of low attenuation corresponding to treatment port
– Probably due to hepatocellular necrosis, edema, and steatosis
If hepatic congestion is severe, patchy congestion simulating tumor nodules may be seen
In patients with diffuse hepatic steatosis, irradiated area may appear as region of increased attenuation
– May be due to loss of fat in irradiated hepatocytes or regional edema
Over time, sharp borders of irradiated zone become more irregular and indistinct (peripheral parenchyma regenerates)
– Eventually, irradiated area may become atrophic
• CECT
Enhancement pattern of irradiated liver may vary depending on preexisting hepatic pathology
Intense enhancement of irradiated parenchyma may be seen in acute phase injury
– Due to ↑ arterial flow and reduced portal flow
Region of radiation damage that is hypodense on portal venous phase may become hyperdense with prolonged enhancement on delayed phase
– Due to ↓ vascular perfusion, ↓ hepatic venous drainage, and subsequent stasis of contrast medium
Narrowing and irregularity of hepatic vessels (sinusoidal congestion and perisinusoidal edema)
– Vessels within zone may appear normal (no mass effect)
MR Findings
• T1WI
Zone of ↓ intensity on T1WI, ↑ on T2WI
Imaging Recommendations
• Best imaging tool
NECT and CECT or MR T1WI GRE with in- and out-of-phase imaging
• Protocol advice
MR, especially T1WI with in- and opposed-phase GRE, is best means of distinguishing RILD from steatosis
DIFFERENTIAL DIAGNOSIS
Focal Steatosis
• May be geographic, band- or wedge-shaped
• Preservation of enhancing vessels within “lesion”
• Suppression of signal on opposed-phase GRE MR
Hepatic Infarction
• Segmental or geographic hypodense area with straight margins with absent or heterogeneous enhancement
PATHOLOGY
General Features
• Etiology
Patients receiving single 1,200-rad dose of external beam radiation or a 4,000 to 5,500-rad fractionated dose over 6 weeks can develop RILD
Hepatic arterial administration of yttrium-90 glass microspheres
– Emit radiation to perfused hepatic area persisting for 64-hour half-life
Microscopic Features
• Venoocclusive disease
• Massive panlobar congestion, hyperemia, hemorrhage, and mild proliferative change in sublobular central veins
Stasis secondary to injury of these veins
CLINICAL ISSUES
Presentation
• Hepatomegaly, ascites, fatigue
Demographics
• Epidemiology
Now more commonly seen with advent of 3D treatment planning and bone marrow transplantation with total body radiation
Natural History & Prognosis
• Complete clinical recovery typically within 60 days
Complete resolution or progression to atrophy of involved segments and, rarely, cirrhosis
DIAGNOSTIC CHECKLIST
Consider
• Factors that influence variability in liver damage
Irradiated liver volume, radiation fraction size, cytotoxic agents, and nutritional status
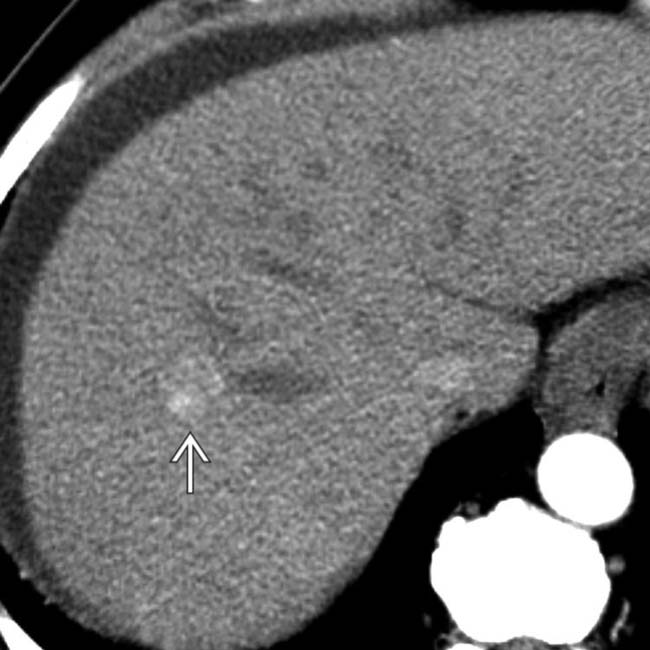
(Left) Arterial phase CECT shows a heterogeneous hypervascular lesion in a 66-year-old man with HCC, prior to the onset of therapy.
(Right) Portal venous phase imaging from the same case shows normal-appearing adjacent liver.
(Left) Repeat nonenhanced CT scan during therapy with hepatic arterial infusion of yttrium-90 microspheres shows a wedge-shaped zone of decreased attenuation in the distribution of the right anterior hepatic artery in which the radioactive microspheres had been placed.
(Right) An arterial phase CT image from the same study shows persistence of the wedge-shaped zone of radiation-induced liver injury. Note the straight line demarcation of the zone of injury .
(Left) A venous phase CT section from the same study shows that the HCC nodule is less vascular than on pretreatment images. Note persistence of the straight line of demarcation of the treated segment of liver.
(Right) Final venous phase CECT section from the same study shows intact blood vessels within the zone of radiation-induced injury. The patient remained clinically asymptomatic with only mild elevation of hepatic transaminase enzymes.
(Left) Axial CECT in a 65-year-old man who had radiation therapy for esophageal carcinoma and metastases to the left lobe shows mixed hypo- and hyperdense lesions in the left and caudate lobes, with a straight line of demarcation from normal liver corresponding to the radiation therapy port.
(Right) Venous phase CT in the same case shows mixed density lesions in the pattern of the radiation port , not corresponding to any anatomical divisions of the liver, all due to radiation hepatitis.
(Left) Axial CECT in a 26-year-old woman with hepatic metastases from nasopharyngeal carcinoma shows a peculiar low-attenuation band through the center of the liver . Note the lack of mass effect on the large hepatic and portal vein branches traversing this zone.
(Right) The same CECT section viewed on bone windows shows 1 of the vertebral metastases that had been treated with external beam radiation therapy.
(Left) Coronal reformatted CT section from the same study shows the band of hypodense liver that represents radiation-induced injury. Again, note the lack of mass effect on vessels within the injured liver, as well as hepatic metastases .
(Right) Representative axial CECT section from the same case 4 months later shows resolution of the radiation injury and decreased size of 1 of the hepatic metastases , the latter representing the effects of chemotherapy rather than the radiation therapy.
Axial NECT following a resection of primary sarcoma of IVC and prior to radiation therapy shows the synthetic graft .
Axial NECT several months after surgical resection and radiation therapy for sarcoma of IVC shows a band of low attenuation and volume loss in the left lobe corresponding to the radiation port.
Axial CECT shows a heterogeneous mass enhancing during the arterial phase, demonstrating hepatocellular carcinoma.
Axial CECT shows a patient with hepatocellular carcinoma (HCC) following hepatic arterial embolization of yttrium-90 microspheres. The wedge of hypodensity in segments 5 and 8 represents radiation hepatitis.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Vessels within zone may appear normal (no mass effect)
Usually low density on NECT and CECT
May have mixed hypervascular and hypovascular foci
• Region of radiation damage that is hypodense on portal venous phase may become hyperdense with prolonged enhancement on delayed phase
Due to ↓ vascular perfusion, ↓ hepatic venous drainage, and subsequent stasis of contrast medium
• MR, especially T1WI with in- and opposed-phase GRE, is best means of distinguishing RILD from steatosis
TOP DIFFERENTIAL DIAGNOSES
• Focal steatosis
• Hepatic infarction
PATHOLOGY
• Patients receiving single 1,200-rad dose of external beam radiation or a 4,000 to 5,500-rad fractionated dose over 6 weeks can develop RILD
• Hepatic arterial administration of yttrium-90 glass microspheres
Emit radiation to perfused hepatic area persisting for 64-hour half-life
CLINICAL ISSUES
• Complete clinical recovery typically seen within 60 days, but there may be permanent hepatocyte loss, fat deposition, fibrosis, and obliteration of central veins
(Left) Axial CECT shows a vertically oriented zone of low attenuation extending from the cranial to caudal aspect of the liver in a straight line , following external radiation therapy for lymphoma.
(Right) Axial CECT shows a straight line of demarcation of damaged liver in the left lobe due to external radiation therapy for esophageal carcinoma. Note the normal appearance of the left hepatic vein within the zone of radiation-induced liver disease (RILD).
(Left) Axial CECT shows decreased attenuation within the posterior segments of the liver, with a straight line of demarcation corresponding to the segments that had received yttrium-90 microsphere embolization for hepatocellular carcinoma (HCC). Note the normal appearance of the posterior right portal vein within the damaged liver.
(Right) CECT section from the same case shows viable satellite foci of HCC within the untreated anterior segments of liver .
TERMINOLOGY
Abbreviations
• Radiation-induced liver disease (RILD)
Definitions
• Syndrome characterized by development of anicteric ascites ∼ 2 weeks to 4 months after hepatic irradiation
• Form of venoocclusive disease due to fibrous obliteration of terminal hepatic venules → postsinusoidal obstruction
IMAGING
General Features
• Best diagnostic clue
Sharp line of demarcation between normal and abnormal parenchyma corresponds to radiation port or vascular distribution of yttrium-90 microspheres
CT Findings
• NECT
Sharply defined band of low attenuation corresponding to treatment port
– Probably due to hepatocellular necrosis, edema, and steatosis
If hepatic congestion is severe, patchy congestion simulating tumor nodules may be seen
In patients with diffuse hepatic steatosis, irradiated area may appear as region of increased attenuation
– May be due to loss of fat in irradiated hepatocytes or regional edema
Over time, sharp borders of irradiated zone become more irregular and indistinct (peripheral parenchyma regenerates)
– Eventually, irradiated area may become atrophic
• CECT
Enhancement pattern of irradiated liver may vary depending on preexisting hepatic pathology
Intense enhancement of irradiated parenchyma may be seen in acute phase injury
Buy Membership for Radiology Category to continue reading. Learn more here




 , following external radiation therapy for lymphoma.
, following external radiation therapy for lymphoma.
 in the left lobe due to external radiation therapy for esophageal carcinoma. Note the normal appearance of the left hepatic vein
in the left lobe due to external radiation therapy for esophageal carcinoma. Note the normal appearance of the left hepatic vein  within the zone of radiation-induced liver disease (RILD).
within the zone of radiation-induced liver disease (RILD).
 corresponding to the segments that had received yttrium-90 microsphere embolization for hepatocellular carcinoma (HCC). Note the normal appearance of the posterior right portal vein
corresponding to the segments that had received yttrium-90 microsphere embolization for hepatocellular carcinoma (HCC). Note the normal appearance of the posterior right portal vein  within the damaged liver.
within the damaged liver.
 .
.

















 in a 66-year-old man with HCC, prior to the onset of therapy.
in a 66-year-old man with HCC, prior to the onset of therapy.
 in the distribution of the right anterior hepatic artery in which the radioactive microspheres had been placed.
in the distribution of the right anterior hepatic artery in which the radioactive microspheres had been placed.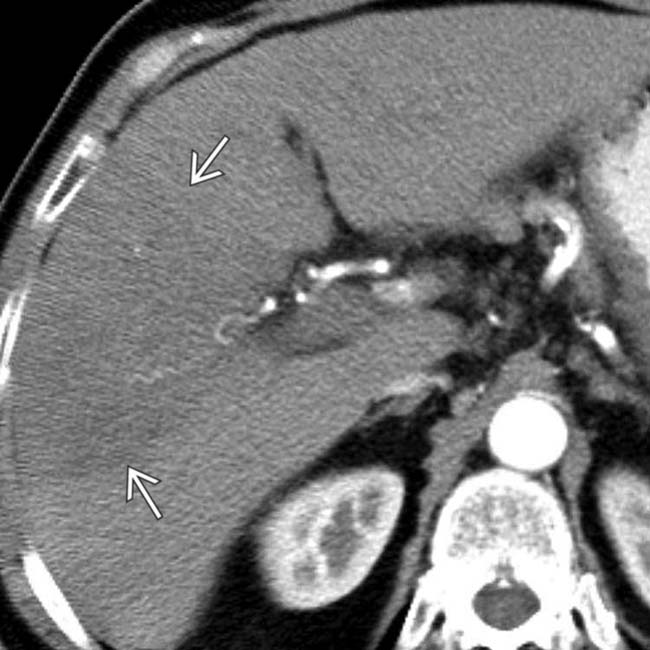
 .
.
 is less vascular than on pretreatment images. Note persistence of the straight line of demarcation
is less vascular than on pretreatment images. Note persistence of the straight line of demarcation  of the treated segment of liver.
of the treated segment of liver.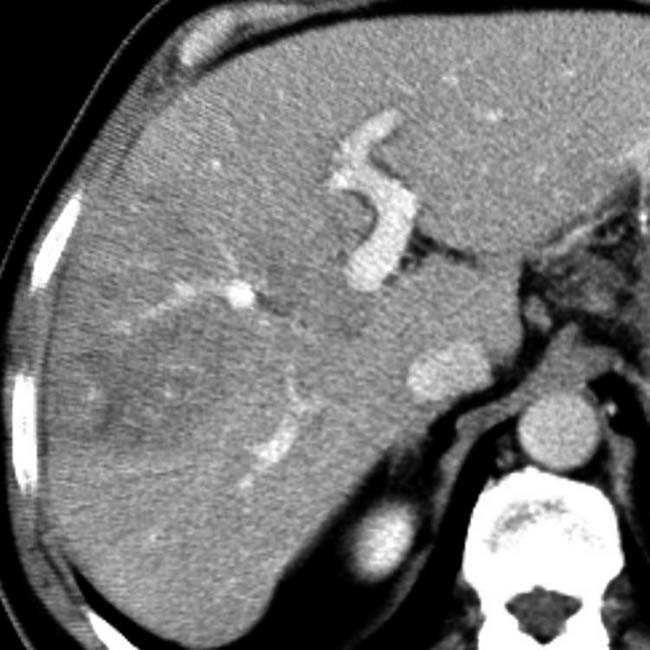
 corresponding to the radiation therapy port.
corresponding to the radiation therapy port.
 , not corresponding to any anatomical divisions of the liver, all due to radiation hepatitis.
, not corresponding to any anatomical divisions of the liver, all due to radiation hepatitis.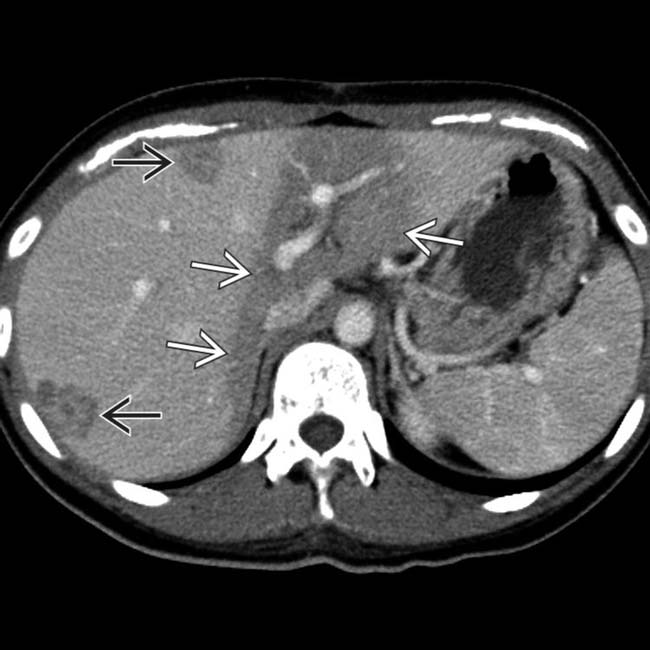
 from nasopharyngeal carcinoma shows a peculiar low-attenuation band through the center of the liver
from nasopharyngeal carcinoma shows a peculiar low-attenuation band through the center of the liver  . Note the lack of mass effect on the large hepatic and portal vein branches traversing this zone.
. Note the lack of mass effect on the large hepatic and portal vein branches traversing this zone.
 that had been treated with external beam radiation therapy.
that had been treated with external beam radiation therapy.
 that represents radiation-induced injury. Again, note the lack of mass effect on vessels within the injured liver, as well as hepatic metastases
that represents radiation-induced injury. Again, note the lack of mass effect on vessels within the injured liver, as well as hepatic metastases  .
.
 , the latter representing the effects of chemotherapy rather than the radiation therapy.
, the latter representing the effects of chemotherapy rather than the radiation therapy.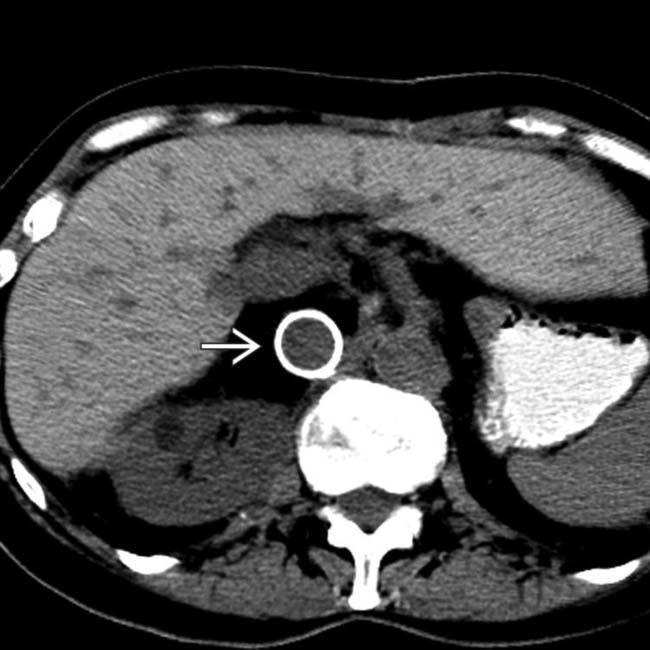
 .
.
 enhancing during the arterial phase, demonstrating hepatocellular carcinoma.
enhancing during the arterial phase, demonstrating hepatocellular carcinoma.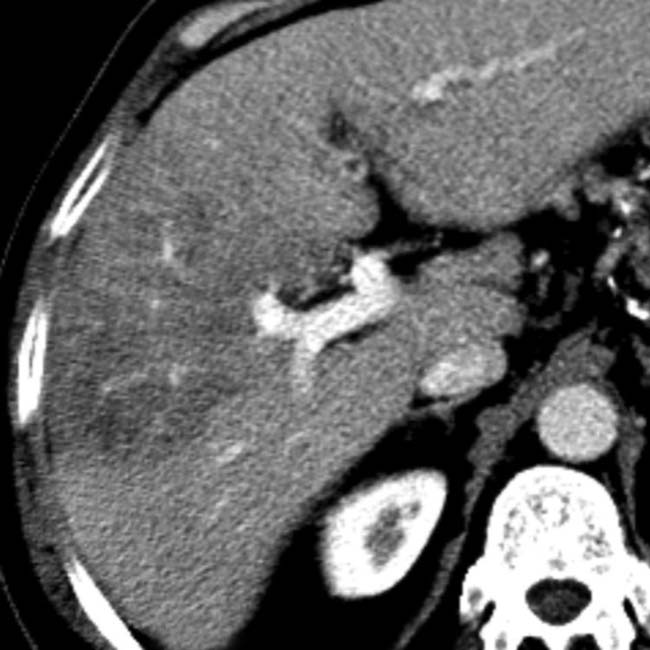
 Intense enhancement of irradiated parenchyma may be seen in acute phase injury
Intense enhancement of irradiated parenchyma may be seen in acute phase injury
