Pulmonary Edema
After reading this chapter, you will be able to:
• List the anatomic alterations of the lungs associated with pulmonary edema.
• Describe the causes of pulmonary edema.
• List the cardiopulmonary clinical manifestations associated with pulmonary edema.
• Describe the general management of pulmonary edema.
• Describe the clinical strategies and rationales of the SOAPs presented in the case study.
• Define key terms and complete self-assessment questions at the end of the chapter and on Evolve.
Anatomic Alterations of the Lungs
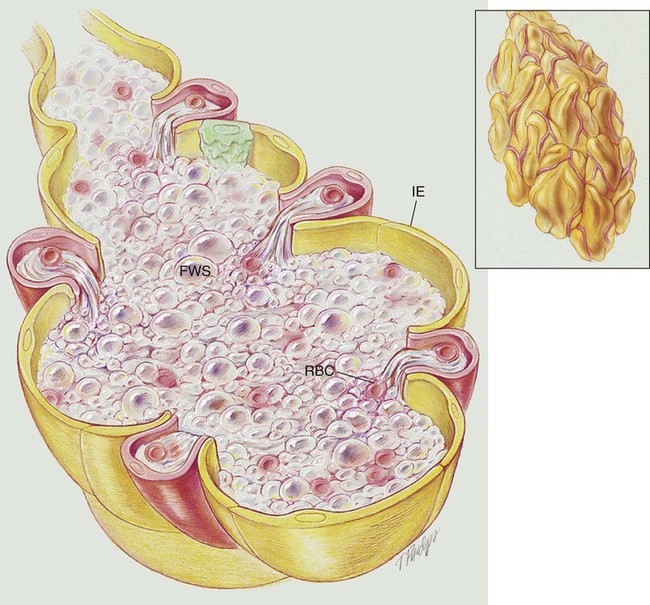
Pulmonary edema results from excessive movement of fluid from the pulmonary vascular system to the extravascular system and air spaces of the lungs. Fluid first seeps into the perivascular and peribronchial interstitial spaces; depending on the degree of severity, fluid may progressively move into the alveoli, bronchioles, and bronchi (see Figure 19-1).
Etiology and Epidemiology
Cardiogenic Pulmonary Edema
Movement of fluid in and out of the capillaries is expressed by Starling’s equation:
< ?xml:namespace prefix = "mml" />

where J is the net fluid movement out of the capillary, K is the capillary permeability factor, Pc and Pi are the hydrostatic pressures in the capillary and interstitial space, and πc and πi are the oncotic pressures in the capillary and interstitial space.
When the hydrostatic pressure within the pulmonary vascular system rises to more than 25 to 30 mm Hg, the oncotic pressure loses its holding force over the fluid within the pulmonary capillaries. Consequently fluid starts to spill into the interstitial and air spaces of the lungs (see Figure 19-1).
Clinically, the patient with left ventricular failure often has anxiety, delirium, dyspnea, orthopnea, paroxysmal nocturnal dyspnea, cough, fatigue, and adventitious breath sounds. Because of poor peripheral circulation, such patients often have cool skin, diaphoresis, cyanosis of the digits, and peripheral pallor. Increased pulmonary capillary hydrostatic pressure is the most common cause of pulmonary edema. Box 19-1 provides common causes of cardiogenic pulmonary edema. Box 19-2 provides common risk factors for coronary heart disease (CHD).
Noncardiogenic Pulmonary Edema
Increased Capillary Permeability
Decreased Oncotic Pressure
• Overtransfusion and/or rapid transfusion of intravenous fluids
Although the exact mechanisms are not known, Box 19-3 provides other causes of conditions associated with noncardiogenic pulmonary edema.
 OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Pulmonary Edema
OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Pulmonary Edema
The following clinical manifestations result from the pathologic mechanisms caused (or activated) by Atelectasis (see Figure 9-8), Increased Alveolar-Capillary Membrane Thickness (see Figure 9-10), and, in severe cases, Excessive Bronchial Secretions (see Figure 9-12)—the major anatomic alterations of the lungs associated with pulmonary edema (see Figure 19-1).
CLINICAL DATA OBTAINED AT THE PATIENT’S BEDSIDE
Increased Heart Rate (Pulse) and Blood Pressure
Cheyne-Stokes respiration may be seen in patients with severe left-sided heart failure and pulmonary edema. Some authorities have suggested that the cause of Cheyne-Stokes respiration in these patients may be related to the prolonged circulation time between the lungs and the central chemoreceptors. Cheyne-Stokes respiration is a classic clinical manifestation in central sleep apnea (see Chapter 30).
Paroxysmal Nocturnal Dyspnea (PND) and Orthopnea
Patients with pulmonary edema often awaken with severe dyspnea after several hours of sleep. This condition is called paroxysmal nocturnal dyspnea. This condition is particularly prevalent in patients with cardiogenic pulmonary edema. While the patient is awake, more time is spent in the erect position and, as a result, excess fluids tend to accumulate in the dependent portions of the body. When the patient lies down, however, the excess fluids from the dependent parts of the body move into the bloodstream and cause an increase in venous return to the lungs. This action raises the pulmonary hydrostatic pressure and promotes pulmonary edema. The pulmonary edema in turn produces pulmonary shunting, venous admixture, and hypoxemia. When the hypoxemia becomes severe, the peripheral chemoreceptors are stimulated and initiate an increased ventilatory rate (see Figure 4-4). The decreased lung compliance, J receptor stimulation, and anxiety also may contribute to the paroxysmal nocturnal dyspnea commonly seen in this disorder at night. A patient is said to have orthopnea when dyspnea increases while the patient is in a recumbent position.
CLINICAL DATA OBTAINED FROM LABORATORY TESTS AND SPECIAL PROCEDURES
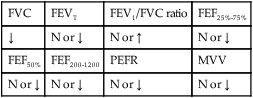
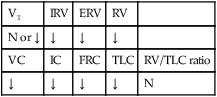
Pulmonary Function Test Findings (Moderate to Severe) (Restrictive Lung Pathology)
FORCED EXPIRATORY FLOW RATE FINDINGS
| FVC | FEVT | FEV1/FVC ratio | FEF25%-75% |
| ↓ | N or ↓ | N or ↑ | N or ↓ |
| FEF50% | FEF200-1200 | PEFR | MVV |
| N or ↓ | N or ↓ | N or ↓ | N or ↓ |
Arterial Blood Gases

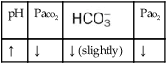

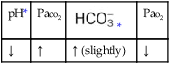
 values will be lower than expected for a particular Pa
values will be lower than expected for a particular PaOxygenation Indices*
 |
Do2† |  |
C(a- )o2 )o2 |
O2ER |  |
| ↑ | ↓ | N | N | ↑ | ↓ |
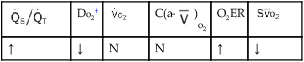
†The Do2 may be normal in patients who have compensated to the decreased oxygenation status with (1) an increased cardiac output, (2) an increased hemoglobin level, or (3) a combination of both. When the Do2 is normal, the O2ER is usually normal.
*C(a- )O2, Arterial-venous oxygen difference; DO2, total oxygen delivery; O2ER, oxygen extraction ratio;
)O2, Arterial-venous oxygen difference; DO2, total oxygen delivery; O2ER, oxygen extraction ratio;  , pulmonary shunt fraction;
, pulmonary shunt fraction;  , mixed venous oxygen saturation;
, mixed venous oxygen saturation;  , oxygen consumption.
, oxygen consumption.
Hemodynamic Indices‡
Cardiogenic Pulmonary Edema Moderate to Severe Stages
| CVP | RAP |  |
PCWP | CO | SV |
| ↑ | ↑ | ↑ | ↑ | ↓ | ↓ |
| SVI | CI | RVSWI | LVSWI | PVR | SVR |
| ↓ | ↓ | ↑ | ↓ | ↑ | ↑ |
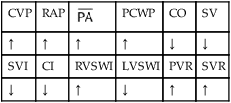
‡CO, Cardiac output; CVP, central venous pressure; LVSWI, left ventricular stroke work index;  , mean pulmonary artery pressure; PCWP, pulmonary capillary wedge pressure; PVR, pulmonary vascular resistance; RAP, right atrial pressure; RVSWI, right ventricular stroke work index; SV, stroke volume; SVI, stroke volume index; SVR, systemic vascular resistance.
, mean pulmonary artery pressure; PCWP, pulmonary capillary wedge pressure; PVR, pulmonary vascular resistance; RAP, right atrial pressure; RVSWI, right ventricular stroke work index; SV, stroke volume; SVI, stroke volume index; SVR, systemic vascular resistance.
The radiographic findings associated with left heart failure are commonly described as follows:
• Mild left-sided heart failure: Pulmonary venous congestion with dilated pulmonary arteries is present.
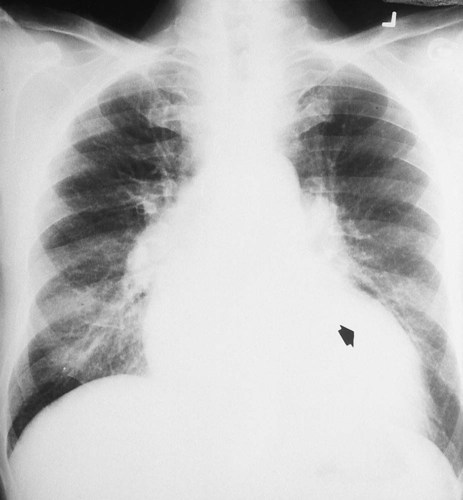
• Moderate left-sided heart failure: Cardiomegaly, engorgement of the pulmonary arteries, and Kerley A and Kerley B lines are present. When cardiomegaly is present, the heart is greater than half the diameter of the thorax in a posterior-anterior chest radiograph (Figure 19-2). Because radiographic densities primarily reflect alveolar filling and not early interstitial edema, by the time abnormal findings are encountered, the pathologic changes associated with pulmonary edema are advanced. Chest x-ray films typically reveal dense, fluffy opacities that spread outward from the hilar areas to the peripheral borders of the lungs (Figure 19-2).
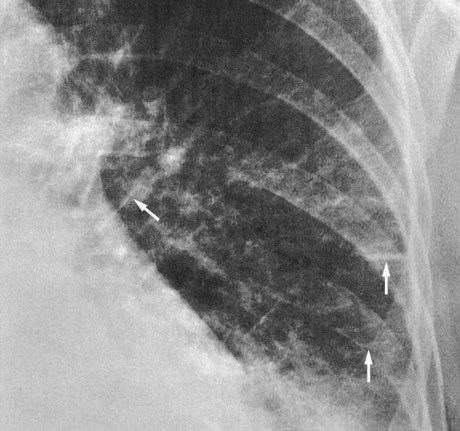
Kerley A lines, which represent deep interstitial edema, radiate out from the hilum into the central portions of the lungs. Kerley A lines do not reach the pleura and are most prevalent in the middle and upper lung regions. Kerley B lines are short, thin, horizontal lines of interstitial edema, usually less than 1 cm in length, that extend inward from the pleural surface. They appear peripherally in contact with the pleura and are parallel to one another at right angles to the pleura. Although they may be seen in any lung region, they are most commonly seen in the lung bases (Figure 19-3).
• Severe left-sided heart failure: During this stage, the patient’s chest radiograph shows cardiomegaly; pulmonary artery engorgement; interstitial pulmonary edema; fluffy, patchy areas of alveolar edema; and often the appearance of the bat’s wing pattern (also called the butterfly pattern)—the peripheral portion of the lungs often remains clear, and this produces what is described as a “butterfly” or “bat’s wing” distribution (Figure 19-4). Pleural effusion may also be seen.

General Management of Pulmonary Edema
Medications and Procedures Commonly Prescribed by the Physician
Positive Inotropic Agents (Improve Cardiac Output)
When left-sided heart failure is present, positive inotropic agents (e.g., digitalis, dopamine, dobutamine, and amiodarone) are commonly administered to increase cardiac output. Digitalis is the most frequently prescribed inotropic agent for heart failure and is the drug of choice (see Appendix II, Positive Inotropic Agents).
Respiratory Care Treatment Protocols
Oxygen Therapy Protocol
Oxygen therapy is used to treat hypoxemia, decrease the work of breathing, and decrease myocardial work. The hypoxemia that develops in pulmonary edema is most commonly caused by the interstitial and alveolar fluid, atelectasis, and capillary shunting associated with the disorder. Hypoxemia caused by capillary shunting is at least partially refractory to oxygen therapy (see Oxygen Therapy Protocol, Protocol 9-1).
Lung Expansion Therapy Protocol
Lung expansion therapy is commonly prescribed to offset the fluid accumulation and alveolar shrinkage associated with pulmonary edema. For example, high-flow mask continuous positive airway pressure (CPAP) has been shown to produce a significant and rapid improvement in oxygenation and ventilatory status in patients with pulmonary edema. Mask CPAP improves decreased lung compliance, decreases the work of breathing, enhances gas exchange, and decreases vascular congestion in patients with pulmonary edema. In fact, mask CPAP is prescribed (at least for a trial period) for patients with pulmonary edema who have arterial blood gas values that reveal impending or acute ventilatory failure—the hallmark clinical manifestation for mechanical ventilation. Often, mask CPAP dramatically improves oxygenation and ventilatory status in these patients and eliminates the need for mechanical ventilation (see Lung Expansion Therapy Protocol, Protocol 9-3).
 27, and Pa
27, and PaRespiratory Assessment and Plan
S Patient states “a feeling of suffocation.”
O Cyanosis, disorientation. Distended neck veins and mottled extremities. BP 105/50, HR 124, RR 28. ECG: sinus tach and occasional PVCs. Distended neck veins, mottled extremities, coarse rhonchi and crackles bilaterally. Frothy pink sputum. CXR: Bilateral fluffy infiltrates and an enlarged heart. ABG: pH 7.11, Paco2 72,  25, and Pao2 56 (Fio2 0.30). Spo2 87%.
25, and Pao2 56 (Fio2 0.30). Spo2 87%.
P Oxygen Therapy Protocol: Increase Fio2 to 0.60 via continuous CPAP mask at 25 cm H2O per Lung Expansion Therapy Protocol. Remain on standby for emergency endotracheal intubation and ventilator support. Continue ECG and oximetry monitoring, and repeat ABG in 30 minutes.
 24, and Pa
24, and PaRespiratory Assessment and Plan
S Patient states, “I’m less short of breath. No pain.”
O Not cyanotic. BP 126/70, HR 96, RR 18. ECG: Mild sinus tachycardia without ectopic beats. Fewer crackles; no sputum production; CXR: Improved. ABG: pH 7.35, Paco2 46,  24, Pao2 120 (Fio2 0.50).
24, Pao2 120 (Fio2 0.50).
• Decreased pulmonary edema (overall impression from the data)
• No longer in ventilatory failure (ABG)
• Acceptable acid-base status with excessively corrected hypoxemia (ABG)
P Reduce O2 per Oxygen Therapy Protocol to 2 L/min by nasal cannula. Discontinue CPAP per Lung Expansion Therapy Protocol. Continue ECG and oximetric monitoring. Repeat ABG in 60 minutes.
Discussion
Acute pulmonary edema is a classic finding in CHF. Several clinical manifestations associated with Increased Alveolar-Capillary Membrane Thickness (see Figure 9-10) were present in this case. For example, the patient’s decreased lung compliance was manifested in his tachycardia and tachypnea, whereas his hypoxemia reflected diffusion blockade associated with classic pulmonary edema. His lung compliance was so reduced that he had progressed to acute ventilatory failure—the severe stage of pulmonary edema. Some Atelectasis (see Figure 9-8) was doubtless also present and was the rationale for CPAP therapy. In addition, the clinical scenario associated with Excessive Bronchial Secretions (see Figure 9-12) also was evident initially with frothy blood-tinged sputum and coarse rhonchi and crackles in both lower lung fields. The patient was too ill to allow valid pulmonary function testing, but the suspicion is that a combined obstructive and restrictive pattern may have been present at the time of the first assessment.
