[level-membership-for-pulmolory-and-respiratory-category]
Pneumothorax
After reading this chapter, you will be able to:
• List the anatomic alterations of the lungs associated with a pneumothorax.
• Describe the causes of a pneumothorax.
• List the cardiopulmonary clinical manifestations associated with a pneumothorax.
• Describe the general management of a pneumothorax.
• Describe the clinical strategies and rationales of the SOAPs presented in the case study.
• Define key terms and complete self-assessment questions at the end of the chapter and on Evolve.
Anatomic Alterations of the Lungs
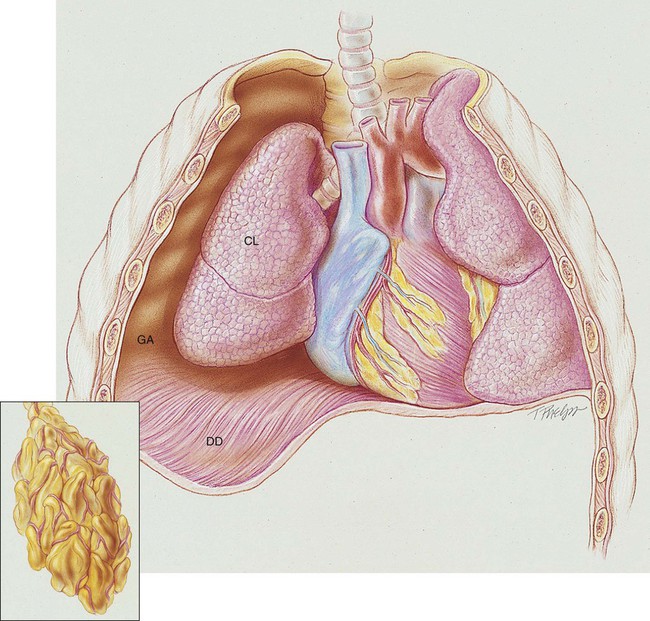
A pneumothorax exists when gas (sometimes called free air) accumulates in the pleural space (see Figure 22-1). When gas enters the pleural space, the visceral and parietal pleura separate. This enhances the natural tendency of the lungs to recoil, or collapse, and the natural tendency of the chest wall to move outward, or expand. As the lung collapses, the alveoli are compressed and atelectasis ensues. In severe cases, the great veins may be compressed and cause the venous return to the heart to diminish.
Etiology and Epidemiology
Gas can gain entrance to the pleural space in the following three ways:
1. From the lungs through a perforation of the visceral pleura
2. From the surrounding atmosphere through a perforation of the chest wall and parietal pleura or, rarely, through an esophageal fistula or a perforated abdominal viscus
3. From gas-forming microorganisms in an empyema in the pleural space (rare)
Traumatic Pneumothorax
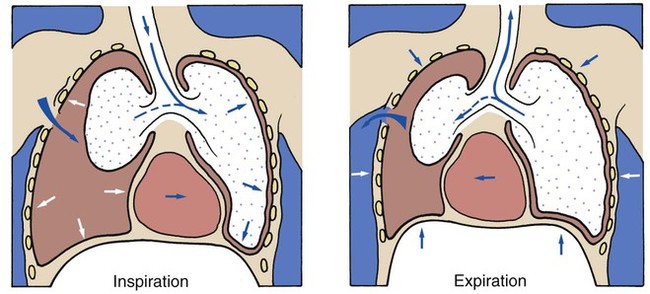
Penetrating wounds to the chest wall from a knife, a bullet, or an impaling object in an automobile or industrial accident are common causes of traumatic pneumothorax. When this type of trauma occurs, the pleural space is in direct contact with the atmosphere, and gas can move into and out of the pleural cavity. This condition is known as a sucking chest wound and is classified as an open pneumothorax (Figure 22-2).
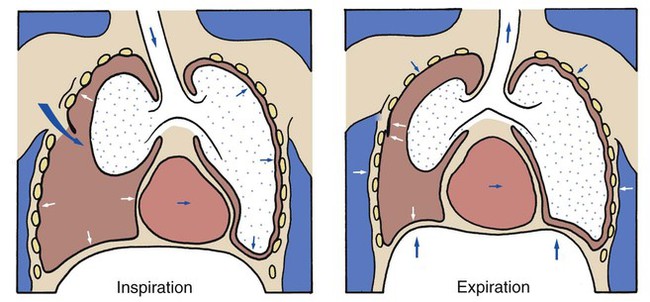
A piercing chest wound also may result in a closed (valvular) or tension pneumothorax through a one-way valvelike action of the ruptured parietal pleura. In this form of pneumothorax, gas enters the pleural space during inspiration but cannot leave during expiration because the parietal pleura (or, more infrequently, the chest wall itself) acts as a check valve. This condition may cause the intrapleural pressure to exceed the atmospheric pressure in the affected area. Technically this form of pneumothorax is classified as a tension pneumothorax (Figure 22-3). This form of pneumothorax is the most serious of all.
Spontaneous Pneumothorax
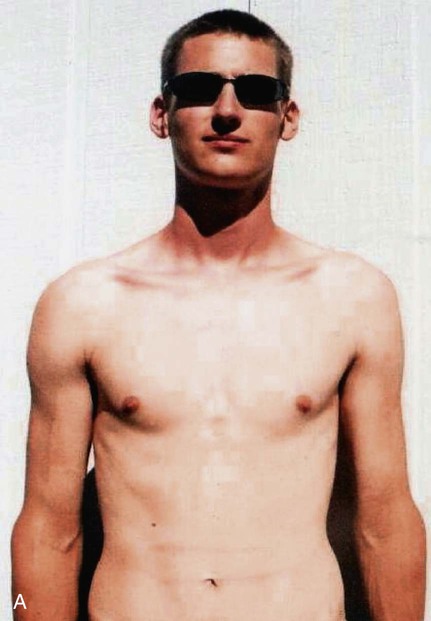
When a pneumothorax occurs suddenly and without any obvious underlying cause, it is referred to as a spontaneous pneumothorax. A spontaneous pneumothorax is secondary to certain underlying pathologic processes such as pneumonia, tuberculosis, and chronic obstructive pulmonary disease (COPD). A spontaneous pneumothorax is sometimes caused by the rupture of a small bleb or bulla on the surface of the lung. This type of pneumothorax often occurs in tall, thin persons aged 15 to 35 years. It may result from the high negative intrathoracic pressure and mechanical stresses that take place in the upper zone of the upright lung (Figure 22-4).
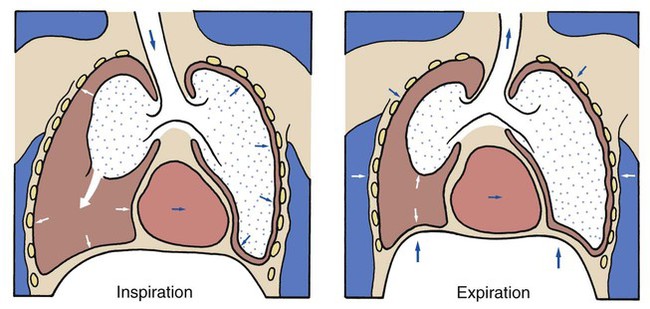
A spontaneous pneumothorax also may behave as a tension pneumothorax. Air from the lung parenchyma may enter the pleural space via a tear in the visceral pleura during inspiration but is unable to leave during expiration because the visceral tear functions as a check valve (see Figure 22-4). This condition may cause the intrapleural pressure to exceed the intraalveolar pressure. This form of pneumothorax is classified as both a closed pneumothorax and a tension pneumothorax.
Iatrogenic Pneumothorax
 OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Pneumothorax
OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Pneumothorax
The following clinical manifestations result from the pathologic mechanisms caused (or activated) by Atelectasis (see Figure 9-8)—the major anatomic alteration of the lungs associated with pneumothorax (see Figure 22-1).
CLINICAL DATA OBTAINED AT THE PATIENT’S BEDSIDE
Increased Respiratory Rate (Tachypnea)
Stimulation of Peripheral Chemoreceptors (Hypoxemia)
If the patient has a pneumothorax as a result of a sucking chest wound, an additional mechanism also may promote hypoventilation. In other words, when a patient with this type of pneumothorax inhales, the intrapleural pressure on the unaffected side decreases. As a result the mediastinum often moves to the unaffected side, where the pressure is lower, and compresses the normal lung. The intrapleural pressure on the affected side also may decrease, and some air may enter through the chest wound and further shift the mediastinum toward the normal lung. During expiration the intrapleural pressure on the affected side rises above atmospheric pressure, and gas escapes from the pleural space through the chest wound. As gas leaves the pleural space, the mediastinum moves back toward the affected side. Because of this back-and-forth movement of the mediastinum, some gas from the normal lung may enter the collapsed lung during expiration and cause it to expand slightly. During inspiration, however, some of this “rebreathed dead space gas” may move back into the normal lung. This paradoxic movement of gas within the lungs is known as pendelluft. As a result of the pendelluft, the patient hypoventilates (see Figure 22-2).
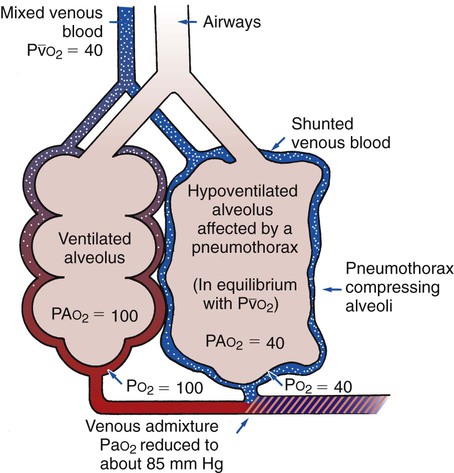
As a result of the reduced alveolar ventilation, the patient’s  ratio decreases. This leads to intrapulmonary shunting and venous admixture (Figure 22-5). Because of the venous admixture, the Pao2 and Cao2 decrease. As this condition intensifies, the patient’s arterial oxygen level may decline to a point low enough to stimulate the peripheral chemoreceptors. Stimulation of the peripheral chemoreceptors in turn initiates an increased ventilatory rate.
ratio decreases. This leads to intrapulmonary shunting and venous admixture (Figure 22-5). Because of the venous admixture, the Pao2 and Cao2 decrease. As this condition intensifies, the patient’s arterial oxygen level may decline to a point low enough to stimulate the peripheral chemoreceptors. Stimulation of the peripheral chemoreceptors in turn initiates an increased ventilatory rate.
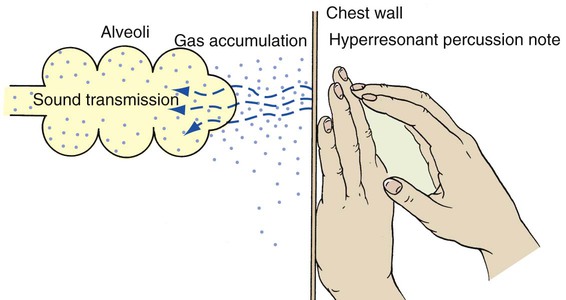
• Hyperresonant percussion note over the pneumothorax
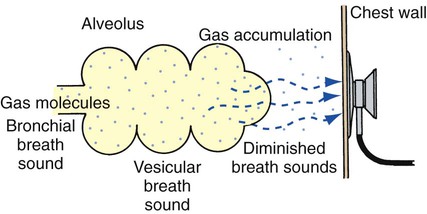
• Diminished breath sounds over the pneumothorax
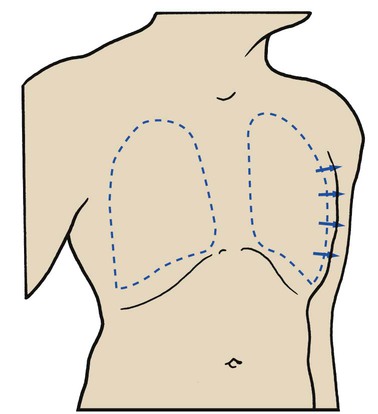
• Increased thoracic volume on the affected side (particularly in tension pneumothorax)
As gas accumulates in the pleural space, the ratio of air to solid tissue increases. Percussion notes resonate more freely throughout the gas in the pleural space as well as in the air spaces within the lung (Figure 22-6). When this area is auscultated, however, the breath sounds are diminished (Figure 22-7). When intrapleural gas accumulates, and intrathoracic pressure is excessively high, the mediastinum may be forced to the unaffected side. If this is the case, there will be a tracheal shift and the heart sounds will be displaced during auscultation.
Finally, the gas that accumulates in the pleural space enhances not only the natural tendency of the lungs to collapse but also the natural tendency of the chest wall to expand. Therefore in a large pneumothorax the chest often appears larger on the affected side. This is especially true in patients with a severe tension pneumothorax (Figure 22-8).
CLINICAL DATA OBTAINED FROM LABORATORY TESTS AND SPECIAL PROCEDURES

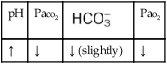

 values will be lower than expected for a particular Pa
values will be lower than expected for a particular PaOxygenation Indices*
| Do2† | O2ER | ||||
| ↑ | ↓ | N | ↑ (severe) | ↑ | ↓ |
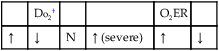
* , Arterial-venous oxygen difference; DO2, total oxygen delivery; O2ER, oxygen extraction ratio;
, Arterial-venous oxygen difference; DO2, total oxygen delivery; O2ER, oxygen extraction ratio;  , pulmonary shunt fraction;
, pulmonary shunt fraction;  , mixed venous oxygen saturation;
, mixed venous oxygen saturation;  , oxygen consumption.
, oxygen consumption.
†The Do2 may be normal in patients who have compensated to the decreased oxygenation status with (1) an increased cardiac output, (2) an increased hemoglobin level, or (3) a combination of both. When the Do2 is normal, the O2ER is usually normal.
Hemodynamic Indices‡
(Large Pneumothorax)
| CVP | RAP |  |
PCWP | CO | SV |
| ↑ | ↑ | ↑ | ↓ | ↓ | ↓ |
| SVI | CI | RVSWI | LVSWI | PVR | SVR |
| ↓ | ↓ | ↑ | ↓ | ↑ | ↓ |
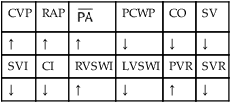
‡CO, Cardiac output; CVP, central venous pressure; LVSWI, left ventricular stroke work index;  , mean pulmonary artery pressure; PCWP, pulmonary capillary wedge pressure; PVR, pulmonary vascular resistance; RAP, right atrial pressure; RVSWI, right ventricular stroke work index; SV, stroke volume; SVI, stroke volume index; SVR, systemic vascular resistance.
, mean pulmonary artery pressure; PCWP, pulmonary capillary wedge pressure; PVR, pulmonary vascular resistance; RAP, right atrial pressure; RVSWI, right ventricular stroke work index; SV, stroke volume; SVI, stroke volume index; SVR, systemic vascular resistance.
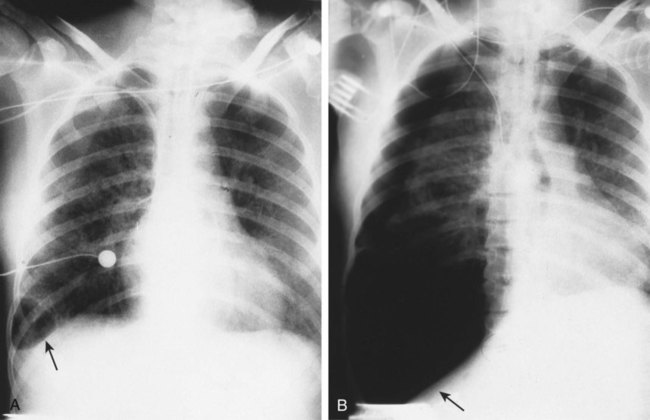
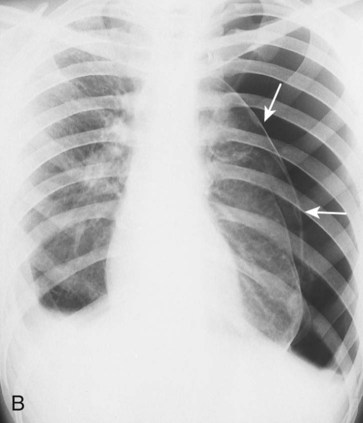
• Increased translucency (darker lung fields) on the side of pneumothorax
• Mediastinal shift to unaffected side in tension pneumothorax
Ordinarily, the presence of a pneumothorax is easily identified on the chest radiograph in the upright posteroanterior view. A small collection of air is often visible if the exposure is made at the end of maximal expiration because the translucency of the pneumothorax is more obvious when contrasted with the density of a partially deflated lung. The pneumothorax is usually seen in the upper part of the pleural cavity when the film is exposed while the patient is in the upright position. Severe adhesions, however, may limit the collection of gas to a specific portion of the pleural space. Figure 22-9, A shows the development of a tension pneumothorax in the lower part of the right lung. Figure 22-9, B shows progression of the same pneumothorax 30 minutes later. Figure 22-10 shows the classic body shape of a 19-year-old male, who is 6 feet 5 inches tall, who experienced a spontaneous left-sided pneumothorax while playing a round of golf.





CASE STUDY
Spontaneous Pneumothorax
Admitting History and Physical Examination
Respiratory Assessment and Plan
S Left chest pain worsened by cough; shortness of breath
O Normal vital signs. Left chest hyperresonant. Trachea shifted to the right. Breath sounds on left “distant.”
A Probable left tension pneumothorax (history and objective indicators)
P Notify physician (who is in the next room). Request stat CXR and ABG. Oxygen Therapy Protocol (partial rebreathing mask with Fio2 between 0.6 to 0.8). Oxygen therapy via partial rebreathing mask (Fio2 0.6 to 0.8). Obtain supplies for tube thoracostomy and place at patient’s bedside.
 21, and Pa
21, and PaRespiratory Assessment and Plan
S “This oxygen mask helps a little.”
O Persistent symptoms and physical findings as in SOAP-1 above. CXR: 50% left tension pneumothorax. Mediastinum shifted to right. ABGs: pH 7.53, Paco2 29,  21, and Pao2 56 (on partial rebreathing mask).
21, and Pao2 56 (on partial rebreathing mask).
P Inform physician of previous and current assessment. Up-regulate Oxygen Therapy Protocol (Increase Fio2 to 0.8 to 1.0 via a nonrebreathing mask). Stay at patient’s bedside until physician arrives. Assist in placement of chest tube.
Discussion
This case nicely demonstrates the signs and symptoms of Atelectasis and intrapulmonary shunting (see Figure 9-8). The physician and respiratory therapist could not hear crackles, however, presumably because the atelectatic segments were separated (distant) from the chest wall and the examiner’s stethoscope.
[/level-membership-for-pulmolory-and-respiratory-category][not-level-membership-for-pulmolory-and-respiratory-category]
Pneumothorax
After reading this chapter, you will be able to:
• List the anatomic alterations of the lungs associated with a pneumothorax.
• Describe the causes of a pneumothorax.
• List the cardiopulmonary clinical manifestations associated with a pneumothorax.
• Describe the general management of a pneumothorax.
• Describe the clinical strategies and rationales of the SOAPs presented in the case study.
• Define key terms and complete self-assessment questions at the end of the chapter and on Evolve.
Anatomic Alterations of the Lungs
A pneumothorax exists when gas (sometimes called free air) accumulates in the pleural space (see Figure 22-1). When gas enters the pleural space, the visceral and parietal pleura separate. This enhances the natural tendency of the lungs to recoil, or collapse, and the natural tendency of the chest wall to move outward, or expand. As the lung collapses, the alveoli are compressed and atelectasis ensues. In severe cases, the great veins may be compressed and cause the venous return to the heart to diminish.
Etiology and Epidemiology
Gas can gain entrance to the pleural space in the following three ways:
1. From the lungs through a perforation of the visceral pleura
2. From the surrounding atmosphere through a perforation of the chest wall and parietal pleura or, rarely, through an esophageal fistula or a perforated abdominal viscus
3. From gas-forming microorganisms in an empyema in the pleural space (rare)
Traumatic Pneumothorax
Penetrating wounds to the chest wall from a knife, a bullet, or an impaling object in an automobile or industrial accident are common causes of traumatic pneumothorax. When this type of trauma occurs, the pleural space is in direct contact with the atmosphere, and gas can move into and out of the pleural cavity. This condition is known as a sucking chest wound and is classified as an open pneumothorax (Figure 22-2).
A piercing chest wound also may result in a closed (valvular) or tension pneumothorax through a one-way valvelike action of the ruptured parietal pleura. In this form of pneumothorax, gas enters the pleural space during inspiration but cannot leave during expiration because the parietal pleura (or, more infrequently, the chest wall itself) acts as a check valve. This condition may cause the intrapleural pressure to exceed the atmospheric pressure in the affected area. Technically this form of pneumothorax is classified as a tension pneumothorax (Figure 22-3). This form of pneumothorax is the most serious of all.
Spontaneous Pneumothorax
When a pneumothorax occurs suddenly and without any obvious underlying cause, it is referred to as a spontaneous pneumothorax. A spontaneous pneumothorax is secondary to certain underlying pathologic processes such as pneumonia, tuberculosis, and chronic obstructive pulmonary disease (COPD). A spontaneous pneumothorax is sometimes caused by the rupture of a small bleb or bulla on the surface of the lung. This type of pneumothorax often occurs in tall, thin persons aged 15 to 35 years. It may result from the high negative intrathoracic pressure and mechanical stresses that take place in the upper zone of the upright lung (Figure 22-4).
A spontaneous pneumothorax also may behave as a tension pneumothorax. Air from the lung parenchyma may enter the pleural space via a tear in the visceral pleura during inspiration but is unable to leave during expiration because the visceral tear functions as a check valve (see Figure 22-4). This condition may cause the intrapleural pressure to exceed the intraalveolar pressure. This form of pneumothorax is classified as both a closed pneumothorax and a tension pneumothorax.
Iatrogenic Pneumothorax
OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Pneumothorax
The following clinical manifestations result from the pathologic mechanisms caused (or activated) by Atelectasis (see Figure 9-8)—the major anatomic alteration of the lungs associated with pneumothorax (see Figure 22-1).
CLINICAL DATA OBTAINED AT THE PATIENT’S BEDSIDE
Increased Respiratory Rate (Tachypnea)
Stimulation of Peripheral Chemoreceptors (Hypoxemia)
If the patient has a pneumothorax as a result of a sucking chest wound, an additional mechanism also may promote hypoventilation. In other words, when a patient with this type of pneumothorax inhales, the intrapleural pressure on the unaffected side decreases. As a result the mediastinum often moves to the unaffected side, where the pressure is lower, and compresses the normal lung. The intrapleural pressure on the affected side also may decrease, and some air may enter through the chest wound and further shift the mediastinum toward the normal lung. During expiration the intrapleural pressure on the affected side rises above atmospheric pressure, and gas escapes from the pleural space through the chest wound. As gas leaves the pleural space, the mediastinum moves back toward the affected side. Because of this back-and-forth movement of the mediastinum, some gas from the normal lung may enter the collapsed lung during expiration and cause it to expand slightly. During inspiration, however, some of this “rebreathed dead space gas” may move back into the normal lung. This paradoxic movement of gas within the lungs is known as pendelluft. As a result of the pendelluft, the patient hypoventilates (see Figure 22-2).
As a result of the reduced alveolar ventilation, the patient’s ratio decreases. This leads to intrapulmonary shunting and venous admixture (Figure 22-5). Because of the venous admixture, the Pao2 and Cao2 decrease. As this condition intensifies, the patient’s arterial oxygen level may decline to a point low enough to stimulate the peripheral chemoreceptors. Stimulation of the peripheral chemoreceptors in turn initiates an increased ventilatory rate.
[/not-level-membership-for-pulmolory-and-respiratory-category]
