Chapter 13 Pediatric Gynecology
APPROACH TO THE PEDIATRIC GYNECOLOGY PATIENT
Establishing Confidentiality
With an older child (over age 10) with concerns of sexual abuse and with all adolescents, all questions regarding sexual history, vaginal discharge, and vulvar itching should be asked without a parent in the room. Adolescents are often loathe to answer questions honestly with a parent listening, especially if they are engaging in a risk behavior about which they don’t want the parents to know. Older children with suspected sexual abuse may not wish to disclose with the perpetrating parent or the spouse of the perpetrator present for fear of punishment at disclosure or for fear of not being believed, with consequences for “lying.” Establishing confidentiality provides an opportunity to ask questions directly of the child without the influence of the parents, with an expectation of honesty. The child or adolescent may still withhold the truth, often delaying to determine whether the clinician is “trustworthy” or if he/she can really help.
The HEADS Questions
The major adolescent morbidities and mortalities stem from risk-taking behaviors rather than disease processes. Therefore, questions designed to elucidate those risk-taking behaviors in an expedient way can be used to avoid the “Oh By the Way” experience, or the major problem casually mentioned in the last few minutes allotted for a visit. A useful acronym for obtaining the psychosocial history from an older child or adolescent is HEADS.1,2 Table 13-1 outlines these questions, which are geared more toward the adolescent but can be modified into simpler terms for the child. With risk behaviors such as cigarettes or drugs, asking about peers’ or friends’ use can be particularly helpful with the older child or younger adolescent, because they may easily talk about others’ risk behaviors, which can then make it easier to talk about themselves.
| Home: Who lives in the home? What happens when there is an argument in the home? |
| If father is not in the home, how often does the child see him? Does that feel like the right amount? In cases of sexual abuse, any boy babysitters? Any alone time with stepfathers, uncles, neighbors, cousins? |
| Education: What grade is the child in? How are their grades this year? How were they last year? |
| Activities: How does the child spend their time? Any sports, or other activities? For teens, are they in a gang or do they have access to a gun? |
| Drugs: Do they know anyone who smokes cigarettes? Do they smoke cigarettes? How much, how often, what have they tried to quit? Do their friends use any drugs? If so, which ones? Have they tried any drugs? Do their friends drink alcohol? Have they tried alcohol? How much, how often, ever to the point of blacking out or passing out? |
| D is also for depression: Ever been depressed? Ever to the point of wanting to hurt yourself? Have you tried to hurt yourself? Ever to the point of wishing you were dead? (passive suicidal ideation). Ever to the point of wanting to kill yourself? Have you specifically had a plan? Which plan(s)? Have you ever tried to kill yourself? Which ways? |
| Sex: Have you ever had sex? Are you sexually attracted to guys, girls, or both? Sexually, has anyone ever touched you in a way that made you uncomfortable? Have you ever had to swap sex for food, clothes, drugs, or shelter? |
The Gynecologic Examination Itself: The Rules
The genital examination of the child should be approached with special verbal acknowledgement to the child and parent before requesting the child to disrobe. With the younger child at preventive healthcare visits, the clinician can state that he/she will look at her bottom every year to make sure that everything is okay, reminding the child and parent that this part of the examination is an expected and routine part of every well-child visit. With younger children, it is useful to state, “It is okay if a doctor looks at your private parts with your mommy here, but it’s not okay if anyone else looks at your private parts without your mommy’s permission. If anyone ever did that, what would you do?” If the child does not respond, often the parent will chime in, “Oh, she knows about strangers, tell the doctor what you know.” Give positive feedback for whatever response the child gives, especially if the child states that she would tell mommy (and the doctor and the police).
Parents often have misconceptions about the hymen. Before and during the examination, the clinician can teach the parents that hymens come in varying shapes and sizes, and that the examination will not harm or “break” the hymen in any way. Use of a diagram can help educate the parent or child about normal female anatomy and can help clear up any misconceptions (Figs. 13-1 and 13-2). Because not all clinicians routinely inspect genitalia despite national recommendations that it should be part of the annual examination, parental anxiety may set a tone for the child. The clinician can educate both parent and child while allaying anxiety and teaching parents to send calming cues to their child, helping reassure the child rather than raise anxiety. Occasionally, this may require more than one visit to complete a gynecologic examination.


Helping the Child Feel in Control
Attention to the little things can help a child feel in control. Rather than asking if the child wants to be in a gown, asking, “Do you prefer the green gown or the yellow one?” allows the child some autonomy in the process. The otoscope or hand lens can be used for magnification; allowing the child to look through the lens to see how it works can help put her at ease. If a colposcope will be used, letting the child view jewelry or fingers through the instrument and showing her how the light turns on and off can demystify the examination. Asking the older child if she prefers the parent in or out of the room can also help the child feel in control.
The child can also maintain control by being asked to assist in holding her labia apart. If the clinician acts relaxed and confident, the patient (and parent) will usually cooperate.3 An abrupt or hurried approach may lead to a child’s refusal to continue, so patience and a calm, confident tone are required. If a child needs more time, the examiner can leave the room until the patient feels ready. Several visits may be necessary to set the child at ease and build confidence that she will not be hurt. If an acute need for an examination exists, as in the case of vaginal bleeding, often an examination under anesthesia may be necessary.
The Actual Examination
Examination of the child with gynecologic complaints should include measuring height, weight (and body mass index if obese), performing a visual inspection from head to toe, including head, neck, heart, lungs, abdomen, Tanner staging (see Chapter 11), breasts (inspection and palpation for masses or discharge), and skin for rashes/lesions. A simple way to remember Tanner staging is as follows. For pubic hair, Tanner I means prepubertal, or no hair. Tanner II hair is fine and downy, and you can count them. Tanner III hair is coarse, in a triangular pattern, and you can count them if you are obsessive-compulsive! Tanner IV pubic hair means too many to count, and Tanner V means out to the thighs. For breast development, Tanner I means no bud yet, or prepubertal. Tanner II means just a breast bud under the nipple. Tanner III extends beyond the nipple, and Tanner IV is a mound of areola on top of a mound of breast. Tanner V refers to adult breasts, with the areola now flush with the breast but the nipple protruding.
Gynecologic assessment includes inspection of the external genitalia, palpation of the inguinal area for hernias or masses, and visualization of the vagina. Hymenal anatomy should be noted and documented in the medical record (see Figs. 13-1 and 13-2). Hymens come in different configurations, with many variants of “normal.” Hymens can be classified as crescentic or posterior rim, annular, or redundant.3,4 Recognition of an imperforate hymen before puberty is generally greatly appreciated by parents, so that anticipatory guidance can be given and an easy procedure accomplished before menstrual flow accumulates behind a blocked passageway. Cribriform or microperforate hymens and septate hymens can also be confusing to the untrained eye; pictures of each are seen in Figure 13-2. Further subtleties of the hymenal examination are addressed in the section Approach to the Child who Has Been Sexually Abused.
Often foreign bodies such as bits of toilet paper can be identified with the child in this position. A butterfly catheter of any size with the needle cut off can be attached to a tuberculin syringe with 1 μL of saline, and then placed inside a 12-inch red rubber bladder catheter to irrigate or wash off the genitalia.5 This catheter within a catheter can be squirted on the patient’s hand or thigh, so as not to surprise her, with explanation that it may feel cold and wet, allowing the area to be irrigated easily.
During the gynecologic examination, the clinician should note the presence of pubic hair, the size of the clitoris, hymenal configuration, signs of estrogenization of the vagina and hymen, and perineal hygiene.3 A clitoris larger than 10 mm in a pubertal girl is considered enlarged. The clitoris in the premenarchal child averages 3 mm in length and 3 mm in transverse diameter.6 If the hymen is viewed in lithotomy or frogleg position and likened to the face of a clock, irregular notching or transactions of the hymen between 5 and 7 o’clock are suggestive of sexual abuse, forced sexual intercourse, or trauma.
In the adolescent, inspection of the genitalia allows for identification of normal versus abnormal medical findings, including folliculitis or “razor burn” in patients who shave or use other means of hair removal (usually noninfectious). Candidal vulvovaginitis can also be seen and may be the first presenting sign of diabetes. In patients who present repeatedly with yeast vaginitis, a urinalysis can rule out diabetes, and a culture on bismuth sulfate (BiGGY) agar can determine whether Candida is the offending organism. Visual inspection allows the opportunity to educate the adolescent in tampon use and in proper hygiene techniques; it may also elicit questions that the teen may have been too embarrassed to ask about (e.g., clitoral size, irregularities in size or shape of labia). A “lump” felt by a teenager may be a Bartholin’s cyst rather than perceived cancer.
Specialized Techniques for the Gynecologic Examination
A small vaginoscope, cystoscope, hysteroscope, or flexible fiberoptic scope with water insufflation of the vagina can be used when knee-chest or lithotomy position does not provide sufficient visualization.3 Capraro first described a step-by-step approach for insertion of the vaginoscope in a young child.7 The child is first allowed to touch the instrument and told that it feels “slippery, funny, and cool.” The instrument is then placed against her inner thigh, repeating the same phrase, and then against her labia, with the physician again stating, “This feels slippery, funny, and cool.” As the vaginoscope is inserted through the hymen, the clinician repeats the same words while firmly pressing the child’s buttocks with the other hand to divert her attention.3 Lidocaine jelly or EMLA cream may be used at the introitus to ease insertion. A Killian nasal speculum with an attached fiberoptic light source or a narrow veterinary otoscope speculum can also be used; the former may not be long enough to visualize the upper aspect of the vagina.8
Office supplies should include kits to test for Neisseria gonorrhoeae and Chlamydia trachomatis, including both culture media/swabs for cases of sexual abuse and nucleic acid amplification test (e.g., GenProbe) for nonabuse cases. Slides, microscope (when permitted by CLIA), saline solution, and 10% potassium hydroxide (KOH) should also be available for use performing wet preps to visualize trichomonads and clue cells, and yeast with KOH. Some clinicians’ offices are not cleared for microscope use; in that case, vaginal swabs for Trichomonas, yeast, and bacterial vaginosis have been shown to be efficacious.9 Having 5% acetic acid available can be useful to identify the gray-white changes of human papillomavirus, and tests for herpes simplex virus should also be available. Newer methods such as DNA probes remain inconsistently accepted evidence in court cases of suspected sexual abuse.
If a vaginal discharge is present in a prepubertal child, cultures can be obtained using a nasopharyngeal Calgiswab moistened with nonbacteriostatic saline. Individual ampules of nebulized saline solution may be kept for convenient office use.3 In obtaining the sample, the clinician should avoid touching the hymenal edges, because the child may find those areas to be particularly sensitive. Asking the child to cough during this part of the examination can both distract the child and allow for the hymen to gape open for a quick swab. The catheter-in-a-catheter technique described earlier can also be useful for sampling vaginal secretions. A Dacron male urethral swab scraped along the vaginal wall can be obtained and directly plated for a Chlamydia culture.3 Muram describes a technique of squirting saline with an Angiocath (needle removed) to fill the vagina followed by holding three swabs perpendicular just outside the vagina with the examiner holding the labia closed over the swabs. The child is asked to cough hard to expel the solution, and the wet swabs can then be used for the needed tests.3
In amenorrheic adolescent girls, a vaginal smear can be obtained to assess estrogenization. A saline-moistened cotton-tipped applicator or moistened Calgiswab can be inserted through the hymenal opening and scraped along the upper lateral sidewall of the vagina.3 If a speculum is being used, the sample can be obtained at that time. The swab is then rolled onto a glass slide, and the slide is sprayed with Pap fixative. The cytologist reads the smear, determining percentages of: parabasal, intermediate, and superficial cells. Parabasal cells are given a score of 0, intermediate cells 0.5, and superficial cells, which are associated with estrogenization, a score of 1. A score of 0 to 30 is seen in prepubertal girls, 50 to 60 in normal pubertal girls, 31 to 50 in hypoestrogenic patients, 60 to 70 in newborns (from maternal estrogen), and 90 to 100 in hyperestrogenic patients.
Screening Interval
Sexually active adolescents should be screened 3 to 6 months after every new partner, with a first pelvic examination within 3 years of initiating sexual activity or by age 21, according to the latest American Cancer Society recommendations.10 Hormonal contraception per se does not mandate a pelvic examination or Papanicalou (Pap) test; linking prescriptions for hormonal contraception to an annual pelvic examination can be an insurmountable barrier to a teenager, resulting in unplanned teen pregnancy.3,11 Adolescents often equate a pelvic examination with Pap smear; if her examination was performed in an ED setting, where Pap smears are not obtained routinely, she may have never received screening for cervical cancer or human papillomavirus. Immunosuppressed girls and teens with multiple partners may require more frequent screening.
APPROACH TO THE CHILD WITH SUSPECTED VULVOVAGINITIS
Infectious Causes
Nonspecific vaginitis accounts for 25% to 75% of cases of vulvovaginitis evaluated at referral centers.12–16 Candida, Peptostreptococcus, and Bacteroides species have been found more commonly in girls with vaginal discharge and/or with vulvovaginitis than in asymptomatic girls.16 In a study of 80 prepubertal girls aged 2 to 12 with vulvovaginitis, pathogenic bacteria were isolated from vaginal swab in 36% of cases, with 59% of this group positive for group A β-hemolytic streptococci.17 The presence of leukocytes in vaginal secretions was associated with the finding of pathologenic bacteria, with a sensitivity of 83% and a specificity of 59%.
Pathogenic bacteria can include group A β-hemolytic streptococci (Streptococcus pyogenes), Haemophilus influenzae, Staphylococcus aureus, Moraxella catarrhalis, Streptococcus pneumoniae, Neisseria meningitides, Shigella, and Yersinia entercolitica.3,17 Vaccination against H. influenzae may be having the unplanned positive effect of lowering the incidence of vaginitis caused by that organism. E. coli was found in the vagina of 36% of girls presenting with vaginitis and in 23% of asymptomatic girls.18 Ninety percent of girls under age 3 had E. coli vaginal colonization, as compared to 15% of 3- to 10-year-old asymptomatic girls.19 In one case report, a prepubertal girl was diagnosed with a prolonged course of vulvovaginitis caused by antibiotic-resistant Shigella flexneri.20 After 3 years of intermittent vaginal bleeding, dysuria, and foul smelling vaginal discharge, unsuccessfully treated with ampicillin, trimethoprim-sulfamethoxazole, cefixime, and amoxicillin/clavulinic acid, symptoms finally resolved with a 14-day course of ciprofloxacin. Bloody discharge is less common in this age group and should warrant culture in the prepubertal child.20,21 Patients may present with or without recent diarrhea.
Noninfectious Causes
A majority of cases of vulvovaginitis in the prepubertal age group are noninfectious; when infectious in etiology, symptoms tend to include more severe inflammation and vaginal discharge.12 Given the great overlap between normal flora and potential pathogens, a positive culture may or may not indicate infection.12 If a young girl presents with green vaginal discharge and no foreign body is found (a common cause, mainly with toilet paper as the offending object), and the culture grows predominantly one organism, infection should be considered and appropriately treated. Cultures should be obtained when visible or profuse discharge is noted and in patients with moderate to severe inflammation.
APPROACH TO THE CHILD WHO HAS BEEN SEXUALLY ABUSED
Acquired abnormalities of the hymen can be the result of either sexual abuse or, more rarely, accidental trauma. Tampon use rarely will cause lacerations of the hymen.22 Signs of acute trauma with sexual abuse can include hymenal transections, hematomas, abrasions, lacerations, and vulvar erythema or irritation. Physical healing after trauma occurs quickly, with complete resolution often by 10 to 12 days.3 Although a hymenal notch, remnant, or scar may be visualized, most girls with a history of substantiated sexual abuse have a completely normal examination.3
Appropriate testing in cases of sexual abuse include a culture for N. gonorrhoeae on modified Thayer-Martin-Jembec medium, with the bacteriology laboratory notified that the specimen is from the vagina of a prepubertal child, so that if a Neisseria species grows, it is properly and unequivocally identified as N. gonorrhoeae for medicolegal purposes.3 Bacterial isolates initially identified as N. gonorrhoeae from children may be other species such as N. lactamica, N. meningitidis, and N. cinerea.23,24 Culture tests for C. trachomatis should be used in the diagnosis of prepubertal infections, especially because false-positive results can occur with some nonculture tests. If culture is not available, nucleic acid amplification tests (NATs) are acceptable if another NAT that targets a different sequence can be performed if the first NAT test is found to be positive.3,25,26
APPROACH TO THE CHILD WITH VAGINAL BLEEDING
Vaginal bleeding in the prepubertal child requires a sensitive approach and careful assessment. In the newborn, vaginal bleeding usually represents withdrawal from maternal estrogen and can be impressive to the clinician or parent, with the passing of clots. After the initial newborn period, the differential diagnosis expands, with foreign body near the top of the list, and including sexual abuse, lichen sclerosis, vulvovaginitis, precocious puberty, and tumors. Other conditions causing vaginal bleeding include urethral prolapse, hemangiomas, and condyloma (although the latter rarely bleed).
Questions for the parent and child include timing and duration of the bleeding, any history of trauma, hematuria, rectal bleeding, symptoms of vaginitis, pubertal development, and potential abuse. Pubertal findings in a child under age 7 or 8, especially with accelerated linear growth, may indicate precocious puberty. Patients with thrombocytopenia are likely to have evidence of bleeding elsewhere, as in petechiae, easy bruising, or epistaxis.3
OTHER GENITAL FINDINGS IN PREPUBERTAL CHILDREN
Atopic Dermatitis
A few children may be sensitive to various diaper creams, wipes, or to a specific brand of diapers themselves. In these children, the perineal area will be brightly erythematous without the satellite lesions common with candida. A simple brand change will usually suffice; in extreme cases, wiping with water on a washcloth rather than using commercially available wipes may be necessary. Given the moist nature of the diaper area, typical atopic dermatitis tends to spare the diaper area until the child is out of diapers. Once toilet trained, the child may scratch at the buttocks or perineum enough to cause superinfection with S. aureus or Streptococcus species; S. aureus infection rarely involves the vagina.27 Use of emollients, hypoallergenic soaps (e.g., Aveeno, Lever 2000, Dove, Neutrogena), and light-handed use of 1% hydrocortisone cream will usually relieve symptoms. Parents need to be taught not to overuse steroid creams to avoid creation of atrophic areas.
Systemic Diseases
Common illnesses such as infectious mononucleosis can present with uncommon findings, such as vulvar ulcers that can mimic herpes simplex virus.27,28 Kawasaki syndrome can be accompanied by desquamation of the perineum, as can Stevens-Johnson syndrome. Crohn’s disease is more likely to involve the perianal area than the vulvar area. Rarely seen in pediatrics, Behçet’s disease is an autoimmune response characterized by the clinical triad of iridocyclitis, oral ulceration, and genital ulceration. Other findings include retinal vasculitis, optic atrophy, meningoencephalitis, proteinuria and hematuria, thrombophlebitis, aneurysms, and arthralgias. With a prevalence ranging from 1:10,000 in Japan to 1:500,000 in North America and Europe, Behçet’s syndrome usually starts with oral apthous ulcers, with genital ulcers often occurring over time and ocular symptoms starting usually in the teenage years.27,29,30 Again, ulcers and excoriation of the vulva may mimic herpes simplex virus infection and cause pain and/or embarrassment to the child, adolescent, and parent. Zinc deficiency can be associated with acrodermatitis enteropathica, or perioral cracking, along with an eroded bilateral vulvar rash with a well-demarcated edge.31,32
Genital Tumors
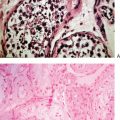
Although rare, genital tumors should be considered in any girl presenting with chronic genital ulceration, nontraumatic swelling of the external genitalia, protrusion of a mass from the vagina, foul-smelling bloody discharge and no evidence of foreign body, or virilization or precocious puberty. Embryonal carcinoma of the vagina (botyroid sarcoma) is found more commonly in young children, with a peak incidence in 2 year olds, and 90% of cases occurring in children under age 5. In younger children, the tumor is often found in the lower vagina, in contrast to tumors of children over age 10, in whom the tumor more often affects the upper vagina or cervix.27 Originating in the lamina propria from undifferentiated mesenchyme, the tumor spreads rapidly below the vaginal epithelium, infiltrating the vaginal wall, bulging outward with polypoid growths containing edematous stroma and dilated blood vessels. Thus, the tumor takes on a cluster-of-grapes appearance. Chemotherapy and conservative surgery, with or without radiation therapy, has resulted in a survival rate of 80% to 90% in girls with localized pelvic rhabdomyosarcoma.3,33,34
CONCLUSION
1 Goldenring JM, Cohen E. Getting into adolescent heads. Contemp Pediatr. 1988;July:75-90.
2 Goldenring JM, Rosen DS. Getting into adolescent heads: An essential update. Contemporary Pediatrics. 2004;60:28-30.
3 Emans SJ, Laufer MR, Goldstein DP. Pediatric and Adolescent Gynecology, 5th ed. Philadelphia: Lippincott Williams & Wilkins, 2005.
4 Pokorny SF. Configuration of the prepuberatal hymen. Am J Obstet Gynecol. 1987;157:950-956.
5 Pokorny SF, Stormer LVN. Atraumatic removal of secretions from the prepubertal vagina. Am J Obstet Gynecol. 1987;157:950-956.
6 Huffman JW, Dewhurst CJ, Capraro VJ. The gynecology of childhood and adolescence. Philadelphia: WB Saunders, 1981.
7 Capraro VJ. Gynecologic examination in child and adolescents. Pediatr Clin North Am. 1972;19:511-528.
8 Hairston L. Physical examination of the prepubertal girl. Clin J Obstet Gynecol. 1997;40:127-134.
9 Blake DR, Duggan A, Quinn T, et al. Evaluation of vaginal infections in adolescent women: Can it be done without a speculum? Pediatrics. 1998;102:939.
10 Saslow D, Runowicz CD, Solomon D, et al. American Cancer Society guideline for the early detection of cervical neoplasia and cancer. CA Cancer J Clin. 2002;52:342.
11 Stewart FH, Harper CC, Ellertson CE, et al. Clinical breast and pelvic examination requirements for hormonal contraception: Current practice vs evidence. JAMA. 2001;285:2232.
12 Jaquiery A, Stylianopoulos A, Hogg G, Grover S. Vulvovaginitis: Clinical features, aetiology, and microbiology of the genital tract. Arch Dis Child. 1999;81:64-67.
13 Paradise JE, Compos JM, Friedman HM, et al. Vulvovaginitis in premenarchal girls: Clinical features and diagnostic evaluation. Pediatrics. 1982;70:193.
14 Emans SJ, Goldstein DP. The gynecologic examination of the prepubertal child with vulvovaginitis: Use of the knee-chest position. Pediatrics. 1980;65:758.
15 Heller RH, Joseph JH, David HJ. Vulvovaginitis in the premenarchal child. J Pediatr. 1969;74:370.
16 Pippo S, Lenko H, Vuento R. Vulvar symptoms in paediatric and adolescent patients. Acta Paediatr. 2000;9:431.
17 Stricker T, Navratil F, Sennhauser FH. Vulvovaginitis in prepubertal girls. Arch Dis Child. 2003;88:324-326.
18 Gerstner GJ, Grunberger W, Boschitch E, et al. Vaginal organisms in prepubertal children with and without vulvovaginitis. Arch Gynecol. 1982;231:247.
19 Hammerschlag MR, Albert S, Rosner I, et al. Microbiology of the vagina in children: Normal and potentially pathogenic organisms. Pediatrics. 1978;68:57.
20 Baiulescu M, Hannon PR, Marcinak JF, et al. Chronic vulvovaginitis caused by antibiotic-resistant Shigella flexneri in a prepubertal child. Pedatr Infect Dis J. 2002;21:170-172.
21 Murphy TV, Nelson JD. Shigella vaginitis: Report of 38 cases and review of the literature. Pediatrics. 1979;63:511-516.
22 Emans SJ, Woods ER, Allred EN, Grace E. Hymenal findings in adolescent women: Impact of tampon use and consensual sexual activity. J Pediatr. 1994;125:153.
23 Alexander ER. Misidentification of sexually transmitted organisms in children: Medicolegal implications. Pediatr Infec Dis J. 1988;7:1.
24 Whittington WL, Rice RJ, Biddle JW, et al. Incorrect identification of Neisseria gonorrhoeae from infants and children. Pediatr Infect Dis J. 1988;7:3.
25 Centers for Disease Control and Prevention. Screening tests to detect Chlamydia trachomatis and Neisseria gonorrhoeae infections 2002. MMWR. 2002;51(RR-15):1.
26 Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2002. MMWR. 2002;51(RR-6):1.
27 Mroueh J, Muram D. Common problems in pediatric gynecology: New developments. Curr Opin Obstet Gynecol. 1999;11:446-463.
28 Sisson BA, Glick L. Genital ulceration as a presenting manifestation of infectious mononucleosis. J Pediatr Adolesc Gynecol. 1998;11:185-187.
29 Uziel Y, Brik R, Padeh S, et al. Juvenile Behçet’s disease in Israel. The Pediatric Rheumatology Study Group of Israel. Clin Exp Rheumatol. 1998;16:502-505.
30 Elem B, Onur C, Ozen S. Clinical features of pediatric Behçet’s disease. J Pediatr Ophthalmol Strabismus. 1998;35:159-161.
31 Fischer GO. Vulvar disease in pre-pubertal girls. Australas J Dermatol. 2001;42:225-236.
32 Stapleton KM, O’Loughlin E, Relic JP. Transient zinc deficiency in a breast-fed premature infant. Australas J Dermatol. 1995;36:157-159.
33 Copeland LJ, Gershenson DM, Saul PB, et al. Sarcoma botyroides of the female genital tract. Obstet Gynecol. 1985;66:262.
34 Arndt CA, Donaldson SS, Anderson JR, et al. What constitutes optimal therapy for patients with rhabdomyosarcoma of the female genital tract. Cancer. 2001;91:2454.
The Center for Young Women’s Health, Children’s Hospital, Boston, provides a useful site for clinicians, educators, parents, and youth, at www.youngwomenshealth.org
For hymenal anatomy: www.youngwomenshealth.org/hymen.htm
American College of Obstetrics and Gynecology (ACOG): www.acog.org
Policy statements for professionals, educational materials for teens and families.
American Academy of Pediatrics (AAP): www.aap.org
Policy statements for pediatricians/health care professionals, educational materials for patients, with links to the Bright Futures web site: http://brightfutures.aap.org/web
American Medical Association (AMA): www.ama-assn.org/ama/pub/category1979.html
Adolescent-specific section with educational resources.
The North American Society for Pediatric and Adolescent Gynecology (NASPAG): www.naspag.org
Useful site for clinicians, including teaching slide set that is available for purchase.