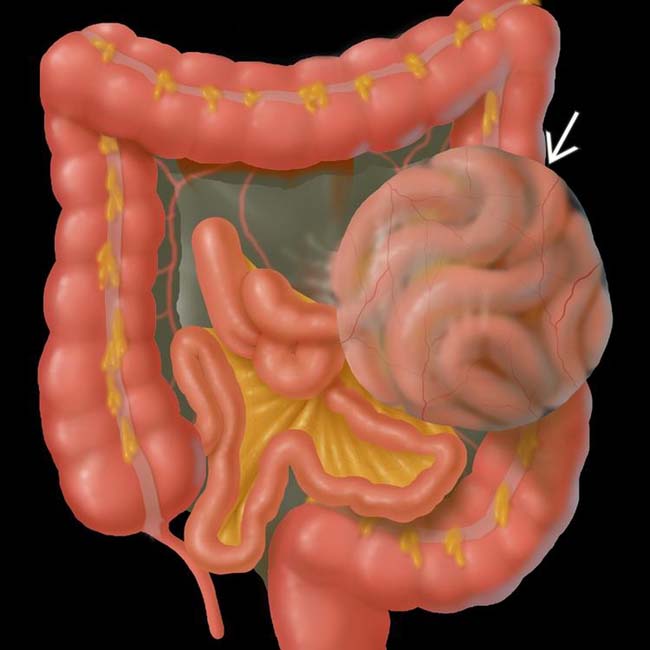
Left (75%): Protrusion of small bowel through paraduodenal mesenteric fossa of Landzert

• CT features
 Left paraduodenal hernia
Left paraduodenal hernia
Left paraduodenal hernia
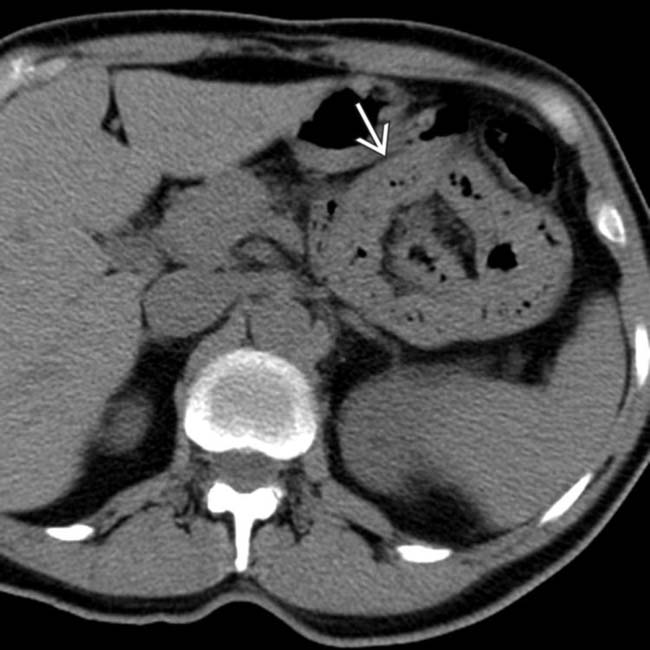
– Encapsulated “cluster” or sac-like mass of small bowel loops located between pancreatic body/tail and stomach to left of ligament of Treitz

• Small bowel follow-through






 containing dilated proximal jejunal loops in a peritoneal sac.
containing dilated proximal jejunal loops in a peritoneal sac.
 of mildly dilated jejunal segments in the left upper quadrant. The outer confines of the hernia sac are well defined. The herniated bowel exerts mass effect on the greater curvature of the stomach, characteristic of a left paraduodenal hernia.
of mildly dilated jejunal segments in the left upper quadrant. The outer confines of the hernia sac are well defined. The herniated bowel exerts mass effect on the greater curvature of the stomach, characteristic of a left paraduodenal hernia.
 in the left upper quadrant.
in the left upper quadrant.
 interposed between the pancreas and stomach. Note the displaced inferior mesenteric vein
interposed between the pancreas and stomach. Note the displaced inferior mesenteric vein  that runs along the anterior edge of the hernia sac. This constellation of findings is characteristic of a left paraduodenal hernia.
that runs along the anterior edge of the hernia sac. This constellation of findings is characteristic of a left paraduodenal hernia.IMAGING
General Features




CT Findings
• Left paraduodenal hernia
 Encapsulated “cluster” or sac-like mass of small bowel loops located between pancreatic body/tail and stomach to the left of ligament of Treitz
Encapsulated “cluster” or sac-like mass of small bowel loops located between pancreatic body/tail and stomach to the left of ligament of Treitz
Encapsulated “cluster” or sac-like mass of small bowel loops located between pancreatic body/tail and stomach to the left of ligament of Treitz


• Right paraduodenal hernia
 Clustered, encapsulated small bowel loops in right upper abdomen lateral and inferior to descending duodenum
Clustered, encapsulated small bowel loops in right upper abdomen lateral and inferior to descending duodenum
Clustered, encapsulated small bowel loops in right upper abdomen lateral and inferior to descending duodenum




Fluoroscopic Findings
• Small bowel follow-through
 Abnormally crowded, clustered bowel loops in right or left upper abdomen with small bowel often absent from pelvis
Abnormally crowded, clustered bowel loops in right or left upper abdomen with small bowel often absent from pelvis
 In cases with bowel obstruction (either complete or partial), point of transition between dilated and nondilated bowel may be visualized
In cases with bowel obstruction (either complete or partial), point of transition between dilated and nondilated bowel may be visualized
Abnormally crowded, clustered bowel loops in right or left upper abdomen with small bowel often absent from pelvis
In cases with bowel obstruction (either complete or partial), point of transition between dilated and nondilated bowel may be visualized


DIFFERENTIAL DIAGNOSIS
Transmesenteric Internal Hernia
• Internal hernia that is most often acquired in setting of prior surgery (most commonly Roux-en-Y gastric bypass and liver transplantation)




PATHOLOGY
General Features













CLINICAL ISSUES
Presentation
• Most common signs/symptoms
 Larger hernias can produce vague discomfort, abdominal distension, periumbilical colicky pain, palpable mass, and localized tenderness
Larger hernias can produce vague discomfort, abdominal distension, periumbilical colicky pain, palpable mass, and localized tenderness
 Larger hernias can produce vague discomfort, abdominal distension, periumbilical colicky pain, palpable mass, and localized tenderness
Larger hernias can produce vague discomfort, abdominal distension, periumbilical colicky pain, palpable mass, and localized tenderness











 in the left abdomen. Notice the location of these loops, immediately adjacent to the distal duodenum, posterior wall of the stomach, and colon, in keeping with a paraduodenal hernia.
in the left abdomen. Notice the location of these loops, immediately adjacent to the distal duodenum, posterior wall of the stomach, and colon, in keeping with a paraduodenal hernia.
 in the left upper quadrant, displacing the stomach forward. Mesenteric vessels supplying the herniated bowel segments converge toward the center of the cluster.
in the left upper quadrant, displacing the stomach forward. Mesenteric vessels supplying the herniated bowel segments converge toward the center of the cluster.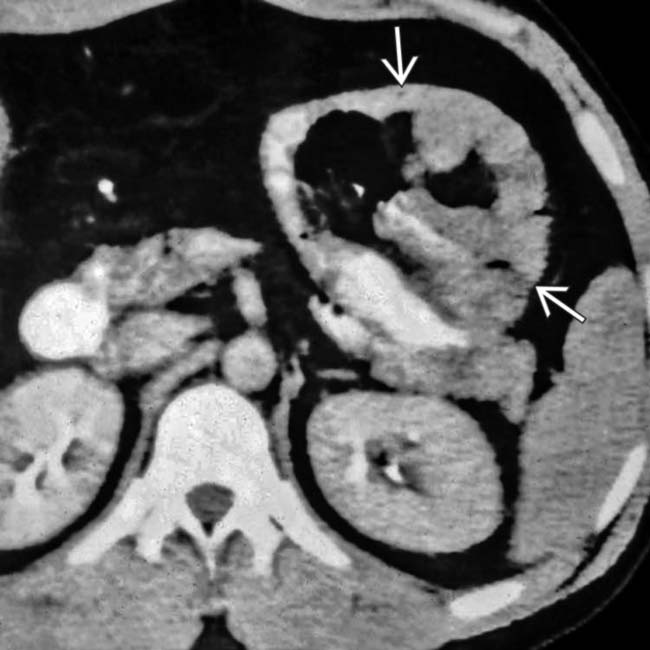
 in the left upper quadrant. Note the sharply defined outer margin of the peritoneal sac around the herniated bowel, and the mesenteric vessels converging toward the sac center, compatible with a left paraduodenal hernia.
in the left upper quadrant. Note the sharply defined outer margin of the peritoneal sac around the herniated bowel, and the mesenteric vessels converging toward the sac center, compatible with a left paraduodenal hernia.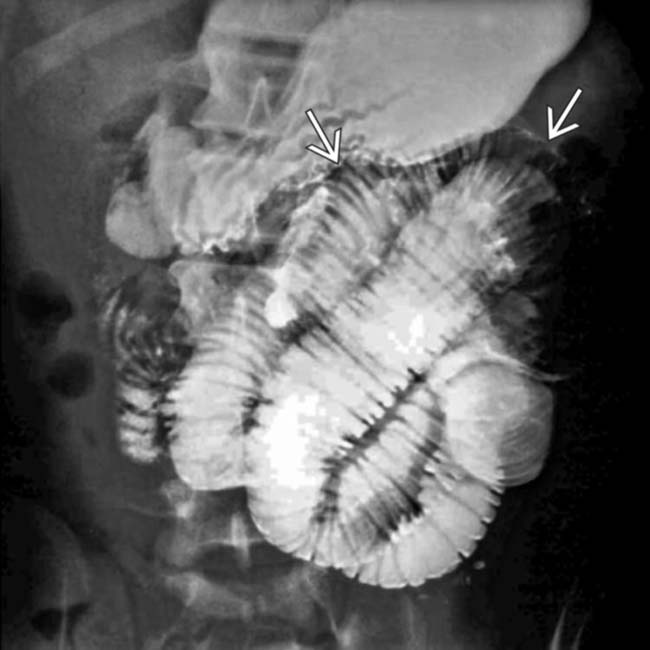
 and delayed passage of contrast to the normal caliber distal small bowel.
and delayed passage of contrast to the normal caliber distal small bowel.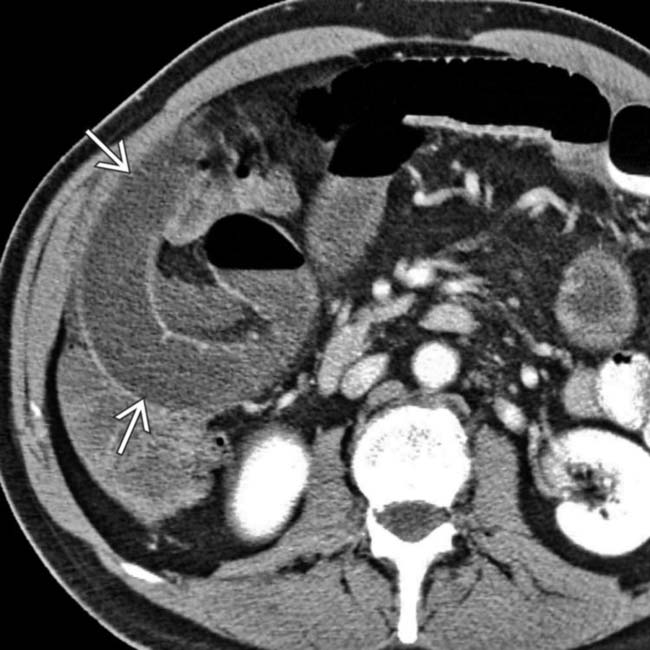
 .
.
 . Note the engorged mesenteric vessels extending directly into the hernia sac.
. Note the engorged mesenteric vessels extending directly into the hernia sac.
 in LUQ, displacing the stomach forward. Mesenteric vessels and herniated bowel segments converge toward the center of the cluster.
in LUQ, displacing the stomach forward. Mesenteric vessels and herniated bowel segments converge toward the center of the cluster.
 .
.
 supplying the constricted segments of bowel.
supplying the constricted segments of bowel.
 between the pancreas and stomach.
between the pancreas and stomach.
 that seem to lie within a confining sac, characteristic of a left paraduodenal hernia.
that seem to lie within a confining sac, characteristic of a left paraduodenal hernia.
 near the pancreatic body, displacing the stomach ventrally.
near the pancreatic body, displacing the stomach ventrally.
 .
.
 with inward-directed mesenteric vessels.
with inward-directed mesenteric vessels.
 with a sac of bowel behind the stomach and inward-directed, engorged mesenteric vessels.
with a sac of bowel behind the stomach and inward-directed, engorged mesenteric vessels.
 with dilated, distorted mesenteric vessels.
with dilated, distorted mesenteric vessels.
 with the dilated jejunum and its mesenteric vessels twisted and displaced.
with the dilated jejunum and its mesenteric vessels twisted and displaced. 
 with distorted, inward-directed mesenteric vessels interposed between pancreatic body and stomach, in keeping with a paraduodenal hernia.
with distorted, inward-directed mesenteric vessels interposed between pancreatic body and stomach, in keeping with a paraduodenal hernia.

