Can be solitary (73%), multiple (10%), or diffusely infiltrative (15%)


• Pancreatic lymphoma










 in the pancreatic tail due to metastatic sarcoma. Metastases from lung, breast, colon, or melanoma could have a similar appearance.
in the pancreatic tail due to metastatic sarcoma. Metastases from lung, breast, colon, or melanoma could have a similar appearance.
 in a patient with a history of prior nephrectomy for renal cell carcinoma (RCC), a characteristic appearance for an RCC metastasis. Based on appearance alone, this mass is indistinguishable from a neuroendocrine tumor.
in a patient with a history of prior nephrectomy for renal cell carcinoma (RCC), a characteristic appearance for an RCC metastasis. Based on appearance alone, this mass is indistinguishable from a neuroendocrine tumor.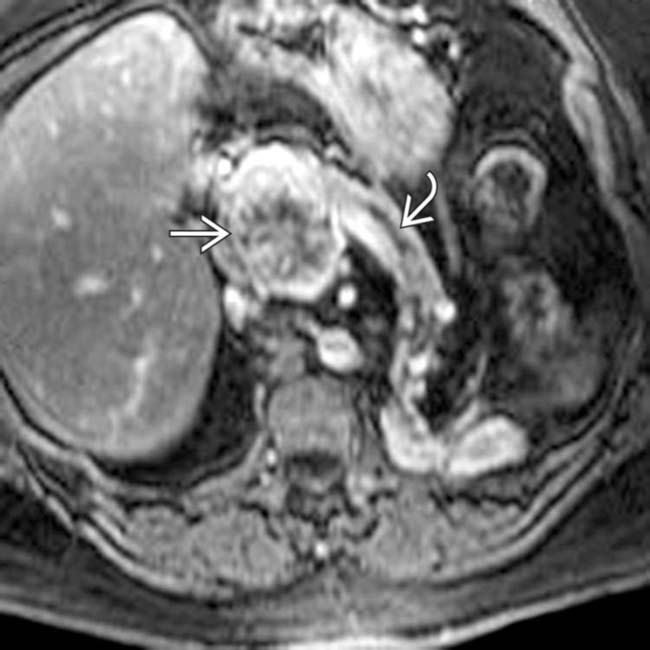
 in the pancreatic head. The pancreatic duct
in the pancreatic head. The pancreatic duct  is mildly dilated upstream. Note the posterior position of the pancreatic tail as a result of a prior left nephrectomy for RCC several years prior to this scan.
is mildly dilated upstream. Note the posterior position of the pancreatic tail as a result of a prior left nephrectomy for RCC several years prior to this scan.
 by non-Hodgkin lymphoma. Also note the associated peripancreatic lymphadenopathy
by non-Hodgkin lymphoma. Also note the associated peripancreatic lymphadenopathy  .
.IMAGING

CT Findings
• Pancreatic metastases


























 from metastatic melanoma. Note also the associated pancreatic tail metastasis
from metastatic melanoma. Note also the associated pancreatic tail metastasis  .
.
 with stippled calcification
with stippled calcification  involving the pancreatic head and neck. The stippled calcifications are not typical for pancreatic ductal adenocarcinoma and are more typical of this patient’s mucinous colon cancer, which has metastasized to the pancreas.
involving the pancreatic head and neck. The stippled calcifications are not typical for pancreatic ductal adenocarcinoma and are more typical of this patient’s mucinous colon cancer, which has metastasized to the pancreas.
 in the pancreas and kidneys
in the pancreas and kidneys  . This combination of findings is typical of renal and pancreatic involvement from non-Hodgkin lymphoma. A neck node biopsy confirmed the diagnosis.
. This combination of findings is typical of renal and pancreatic involvement from non-Hodgkin lymphoma. A neck node biopsy confirmed the diagnosis.
 in the pancreatic head. Note the absence of the right kidney, a finding that should suggest the correct diagnosis of a RCC metastasis.
in the pancreatic head. Note the absence of the right kidney, a finding that should suggest the correct diagnosis of a RCC metastasis.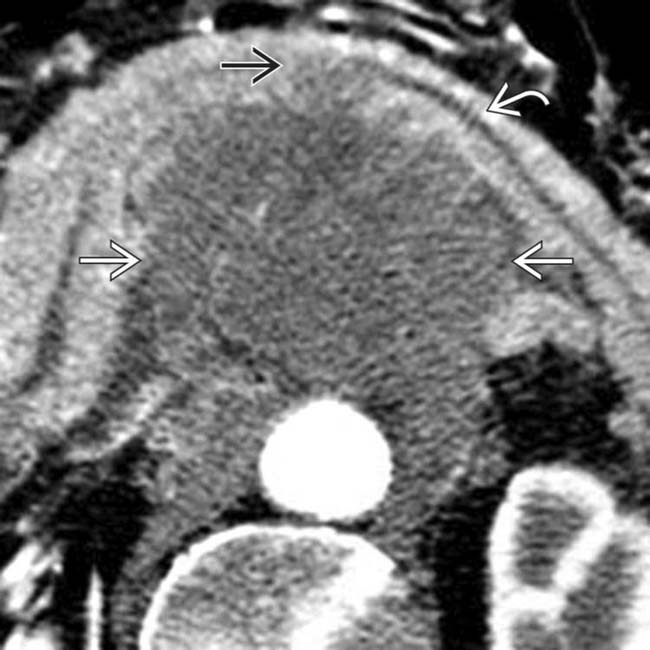
 . Note that the entire pancreatic body is displaced anteriorly by a large, hypodense, periaortic mass
. Note that the entire pancreatic body is displaced anteriorly by a large, hypodense, periaortic mass  that directly invades the body of the pancreas
that directly invades the body of the pancreas  .
.
 by hypodense nodal tissue. Biopsy of an axillary node revealed non-Hodgkin lymphoma.
by hypodense nodal tissue. Biopsy of an axillary node revealed non-Hodgkin lymphoma.
 with surrounding induration and stranding. Superficially, this appearance could initially be suggestive of pancreatitis.
with surrounding induration and stranding. Superficially, this appearance could initially be suggestive of pancreatitis.
 in the surrounding mesentery. Given this lymphadenopathy, the appearance of the pancreas represents diffuse lymphomatous infiltration of the pancreas in a patient with B-cell lymphoma.
in the surrounding mesentery. Given this lymphadenopathy, the appearance of the pancreas represents diffuse lymphomatous infiltration of the pancreas in a patient with B-cell lymphoma.
 extending from the neck of the pancreas and exhibiting marked mass effect on the stomach
extending from the neck of the pancreas and exhibiting marked mass effect on the stomach  . The mass was found to be non-Hodgkin lymphoma after surgery.
. The mass was found to be non-Hodgkin lymphoma after surgery.
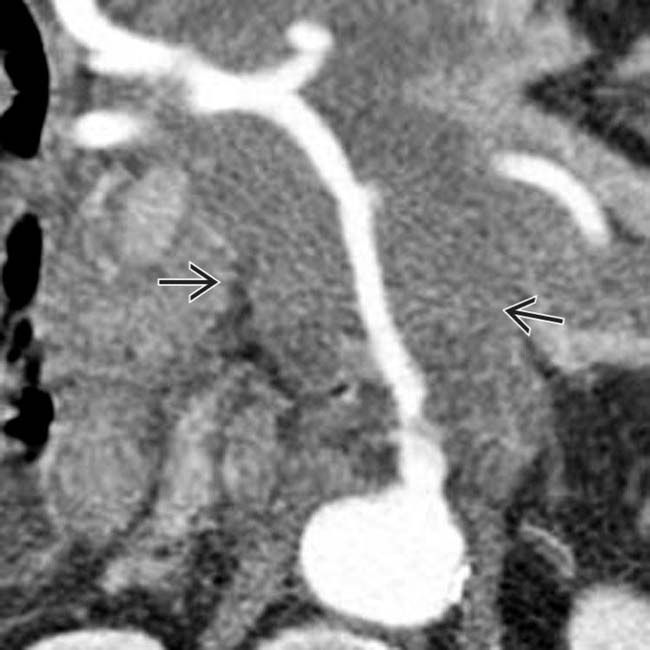
 in the pancreatic body resulting in severe upstream pancreatic ductal dilatation
in the pancreatic body resulting in severe upstream pancreatic ductal dilatation  and parenchymal atrophy. While the imaging features are strongly suggestive of pancreatic cancer, this turned out to be a colon cancer metastasis.
and parenchymal atrophy. While the imaging features are strongly suggestive of pancreatic cancer, this turned out to be a colon cancer metastasis.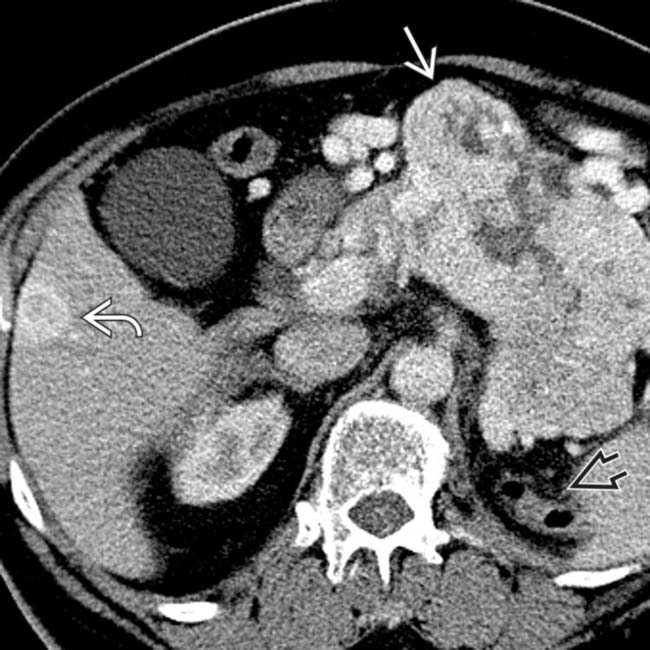
 in the left renal fossa and bulky hypervascular metastases
in the left renal fossa and bulky hypervascular metastases  to the pancreas and liver
to the pancreas and liver  . While a neuroendocrine tumor could appear identical, the nephrectomy suggests the diagnosis of RCC metastases to the pancreas.
. While a neuroendocrine tumor could appear identical, the nephrectomy suggests the diagnosis of RCC metastases to the pancreas.
 in the pancreas and omentum
in the pancreas and omentum  . The left kidney is absent in this patient with RCC mets, which are typically highly vascular, making the inclusion of arterial phase imaging very helpful for detection.
. The left kidney is absent in this patient with RCC mets, which are typically highly vascular, making the inclusion of arterial phase imaging very helpful for detection.
 in a patient whose left renal fossa surgical clips
in a patient whose left renal fossa surgical clips  indicate prior nephrectomy. This represents a characteristic appearance for metastatic renal cell carcinoma.
indicate prior nephrectomy. This represents a characteristic appearance for metastatic renal cell carcinoma.


