[level-membership-for-radiology-category] Pancreas appears identical to lipomatous pseudohypertrophy, but with very different clinical presentation
Clinical presentation is very different, starting in childhood
• Pancreatic senescent changes
Pancreatic atrophy, but rarely clinically significant
Usually more uneven fatty replacement of pancreas
Also associated with obesity, diabetes, and steroid use
• Pancreatic focal fatty infiltration
Usually limited to head-uncinate or body-tail segments
• Shwachman-Diamond syndrome
Rare congenital disorder characterized by pancreatic insufficiency, bone marrow dysfunction, and short stature
• Retroperitoneal liposarcoma
Often confused with lipomatous pseudohypertrophy due to massive fatty hypertrophy in retroperitoneum
PATHOLOGY
• Exact etiology is unknown
• Possibly congenital, but may require inciting factor such as cirrhosis, viral infection, or abnormal metabolism
CLINICAL ISSUES
• Usually incidental finding on CT or in autopsy
• Rarely, patients require enzyme therapy due to exocrine deficiency
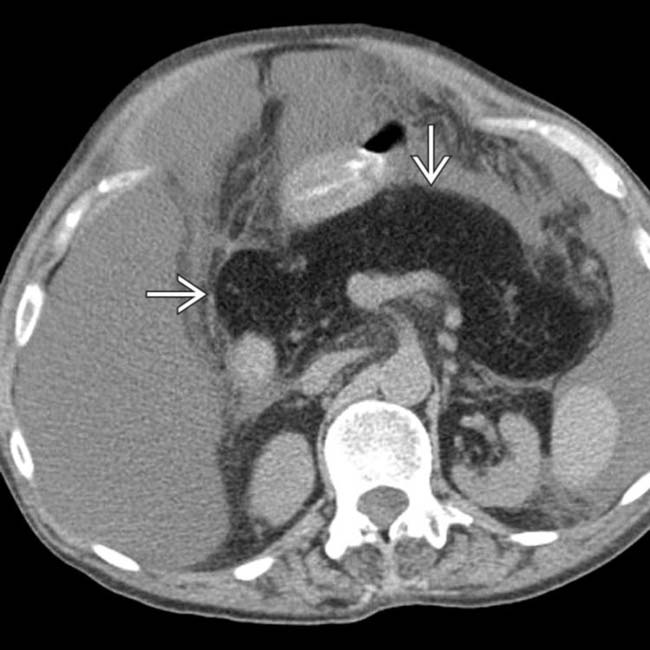
(Left) Axial NECT in a woman with alcoholic cirrhosis shows typical cirrhotic morphology of the liver (nodular with widened fissures) and ascites.
(Right) Axial NECT in the same patient shows diffuse enlargement and fatty replacement of the pancreas , which mimics findings seen in cystic fibrosis.
(Left) Axial T1WI C+ FS MR in the same patient shows the lipomatous pseudohypertrophy with diffuse dropout of signal throughout the body of the pancreas due to fat suppression.
(Right) Axial opposed-phase T1WI in the same patient shows high signal throughout the pseudohypertrophied pancreas .
TERMINOLOGY
Definitions
• Enlargement of pancreas due to replacement by adipose tissue with atrophy of normal exocrine parenchyma
IMAGING
General Features
• Best diagnostic clue
Diffuse enlargement and fatty replacement of pancreas
No imaging or clinical signs of cystic fibrosis
• Location
Focal (tail, body, head) or diffuse involvement (more common)
• Size
Usually 2-4x size of normal pancreas
• Morphology
Homogeneous fatty replacement
Imaging Recommendations
• Best imaging tool
CT or MR
CT Findings
• Homogeneous, focal or diffuse enlargement of pancreas with fatty replacement of affected pancreatic parenchyma
No imaging or clinical signs of cystic fibrosis
• Usually no evidence of ductal obstruction (pancreatic or biliary) or discrete mass
• Mass effect upon adjacent structures due to pancreatic enlargement is common
MR Findings
• Appearance of pancreas follows fat signal on all sequences
DIFFERENTIAL DIAGNOSIS
Cystic Fibrosis
• Appearance of pancreas identical to lipomatous pseudohypertrophy
• Patients with cystic fibrosis can develop cirrhosis
• Unique clinical presentation, beginning in childhood
Chronic infections in lungs, failure to thrive, bowel obstruction, etc.
Pancreatic Senescent Changes
• Age-related lipomatosis, fibrosis, and ductal epithelial alterations
• Pancreatic atrophy, but rarely clinically evident or significant
Usually more uneven, heterogeneous fatty replacement of pancreas
• Also associated with obesity, diabetes, and steroid use
Pancreatic Focal Fatty Infiltration
• Normal-sized pancreas
• Partial fatty replacement of acinar parenchyma
• Often limited to either head-uncinate or body-tail segments
Corresponds to fetal ventral and dorsal segments
Shwachman-Diamond Syndrome
• Rare congenital disorder characterized by pancreatic insufficiency, bone marrow dysfunction, and short stature
Retroperitoneal Liposarcoma
• Lipomatous pseudohypertrophy often confused with liposarcoma due to massive fatty hypertrophy in retroperitoneum and mass effect on adjacent structures
PATHOLOGY
General Features
• Etiology
Unknown
Possibly congenital, but may require inciting factor, such as cirrhosis, viral infection, or abnormal metabolism
• Enlargement of pancreas with focal/diffuse fatty replacement of normal pancreatic tissue
• No evidence of capsule
Microscopic Features
• Marked atrophy and loss of exocrine glandular elements
• Replacement by mature adipose tissue
• Preservation of ducts and islets of Langerhans
• No evidence of fat necrosis or underlying pancreatitis
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
Asymptomatic
Can rarely result in pancreatic exocrine dysfunction
• Other signs/symptoms
Mass effect (common), bile duct obstruction (rare)
Demographics
• Epidemiology
Rare, with only a few sporadic reports in literature
No gender predominance
Usually young patients, but increasingly reported in older patients
Natural History & Prognosis
• Very benign course
• Usually incidental finding on CT or in autopsy
• Rarely, patients require enzyme therapy due to exocrine deficiency
DIAGNOSTIC CHECKLIST
Image Interpretation Pearls
• Look for clinical or imaging evidence of cystic fibrosis as alternative diagnosis
Axial NECT of a patient with cirrhosis and ascites shows enlargement and fatty replacement of the pancreas that mimics findings seen in cystic fibrosis.
In a patient with lipomatous pseudohypertrophy of the pancreas, note the enlargement and fatty replacement of the pancreas , which mimics findings seen in cystic fibrosis. The clinical presentation for patients with cystic fibrosis is very different, with chronic pulmonary infections and other problems starting in early childhood.
Axial CECT in a 40-year-old man with longstanding Crohn disease shows marked fatty infiltration of the pancreas but no enlargement of the gland. The patient had no symptoms of pancreatic disease, and the fatty infiltration of the pancreas is believed to be due to chronic steroid use.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Pancreas appears identical to lipomatous pseudohypertrophy, but with very different clinical presentation
Clinical presentation is very different, starting in childhood
• Pancreatic senescent changes
Pancreatic atrophy, but rarely clinically significant
Usually more uneven fatty replacement of pancreas
Also associated with obesity, diabetes, and steroid use
• Pancreatic focal fatty infiltration
Usually limited to head-uncinate or body-tail segments
• Shwachman-Diamond syndrome
Rare congenital disorder characterized by pancreatic insufficiency, bone marrow dysfunction, and short stature
• Retroperitoneal liposarcoma
Often confused with lipomatous pseudohypertrophy due to massive fatty hypertrophy in retroperitoneum
PATHOLOGY
• Exact etiology is unknown
• Possibly congenital, but may require inciting factor such as cirrhosis, viral infection, or abnormal metabolism
CLINICAL ISSUES
• Usually incidental finding on CT or in autopsy
• Rarely, patients require enzyme therapy due to exocrine deficiency
(Left) Axial NECT in a woman with alcoholic cirrhosis shows typical cirrhotic morphology of the liver (nodular with widened fissures) and ascites.
(Right) Axial NECT in the same patient shows diffuse enlargement and fatty replacement of the pancreas , which mimics findings seen in cystic fibrosis.
(Left) Axial T1WI C+ FS MR in the same patient shows the lipomatous pseudohypertrophy with diffuse dropout of signal throughout the body of the pancreas due to fat suppression.
(Right) Axial opposed-phase T1WI in the same patient shows high signal throughout the pseudohypertrophied pancreas .
TERMINOLOGY
Definitions
• Enlargement of pancreas due to replacement by adipose tissue with atrophy of normal exocrine parenchyma
IMAGING
General Features
• Best diagnostic clue
Diffuse enlargement and fatty replacement of pancreas
No imaging or clinical signs of cystic fibrosis
• Location
Focal (tail, body, head) or diffuse involvement (more common)
• Size
Usually 2-4x size of normal pancreas
Buy Membership for Radiology Category to continue reading. Learn more here








 , which mimics findings seen in cystic fibrosis.
, which mimics findings seen in cystic fibrosis.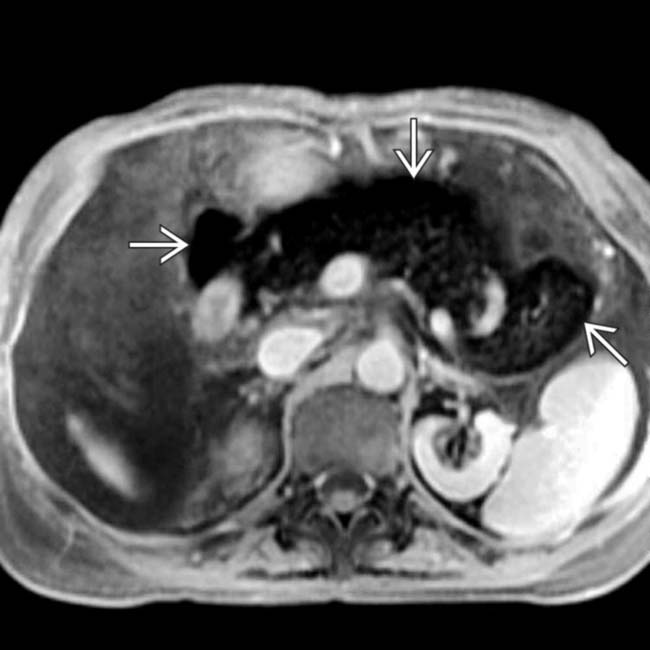
 due to fat suppression.
due to fat suppression.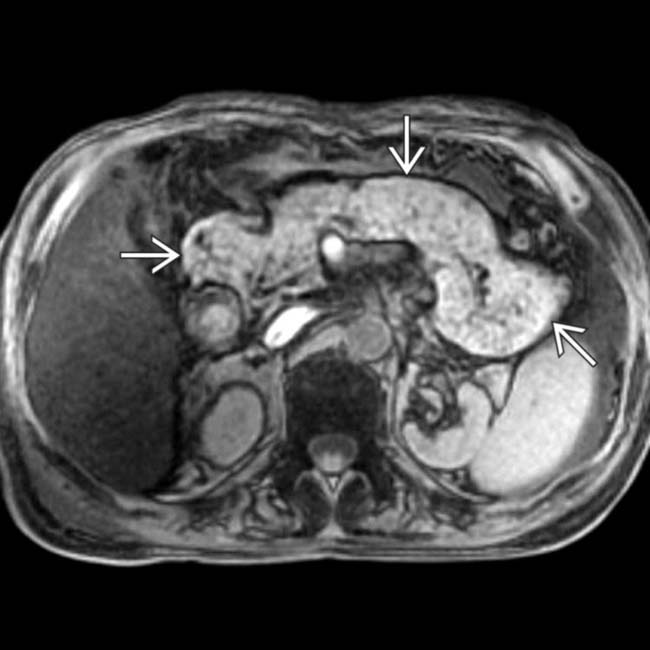
 .
.



















 that mimics findings seen in cystic fibrosis.
that mimics findings seen in cystic fibrosis.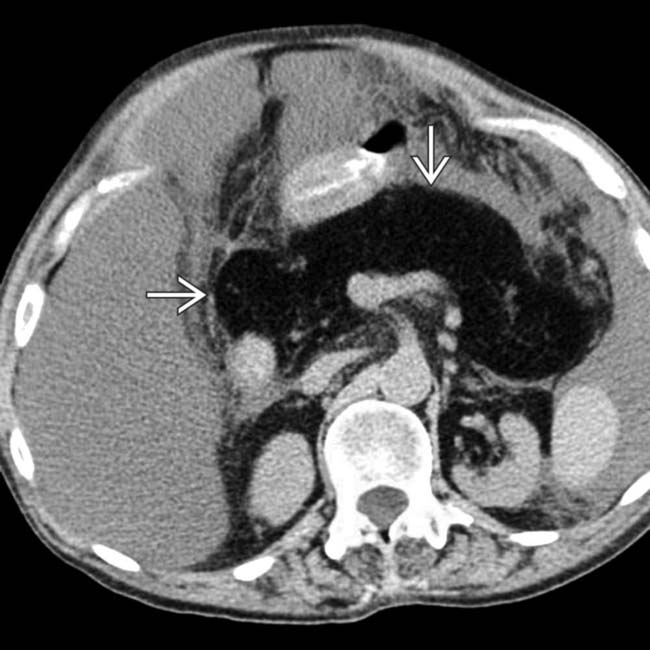
 , which mimics findings seen in cystic fibrosis. The clinical presentation for patients with cystic fibrosis is very different, with chronic pulmonary infections and other problems starting in early childhood.
, which mimics findings seen in cystic fibrosis. The clinical presentation for patients with cystic fibrosis is very different, with chronic pulmonary infections and other problems starting in early childhood.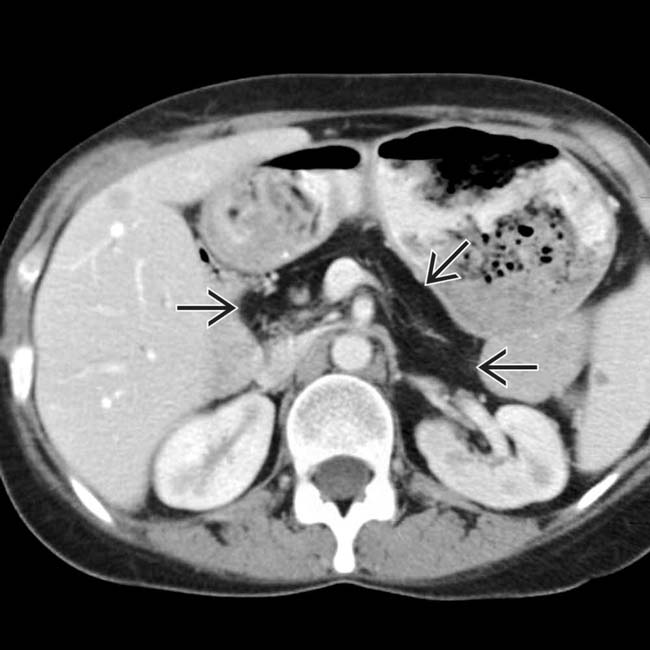
 but no enlargement of the gland. The patient had no symptoms of pancreatic disease, and the fatty infiltration of the pancreas is believed to be due to chronic steroid use.
but no enlargement of the gland. The patient had no symptoms of pancreatic disease, and the fatty infiltration of the pancreas is believed to be due to chronic steroid use.