Chapter 72 Pain Management in The Intensive Care Unit
3 How can pain be assessed in critically ill patients?
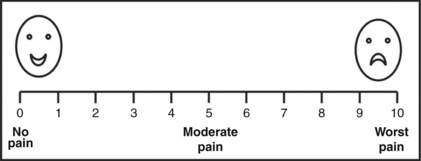
Pain should be assessed and documented at regular intervals. Pain is a subjective experience and is most reliably measured by using a subjective scale such as the numeric rating scale (Fig. 72-1), which can be employed in patients as young as 5 years. Younger patients’ pain is assessed by using the faces scale (Fig. 72-1), which is a modified visual analog scale. In patients unable to communicate, reliance on objective measures (physiologic or behavioral) becomes necessary. Whereas use of physiologic measures (blood pressure, heart rate, tearing, diaphoresis, mydriasis) can cause underreporting and overreporting of pain, use of behavioral measures such as observation of facial expression has been demonstrated to correlate with subjective reporting.
5 What are the treatment options for a critically ill patient in pain?
 Nonpharmacologic treatment of pain includes proper positioning of patients, stabilization of fractures, elimination of irritating physical stimulation, and environmental modification to promote comfort. Because sleep deprivation as well as anxiety and delirium may diminish the pain threshold, it is important to minimize stimuli that can disturb the normal diurnal sleep pattern (noise, artificial light) and treat anxiety and delirium promptly.
Nonpharmacologic treatment of pain includes proper positioning of patients, stabilization of fractures, elimination of irritating physical stimulation, and environmental modification to promote comfort. Because sleep deprivation as well as anxiety and delirium may diminish the pain threshold, it is important to minimize stimuli that can disturb the normal diurnal sleep pattern (noise, artificial light) and treat anxiety and delirium promptly.

7 Which opioids are recommended for routine administration in ICU patients?
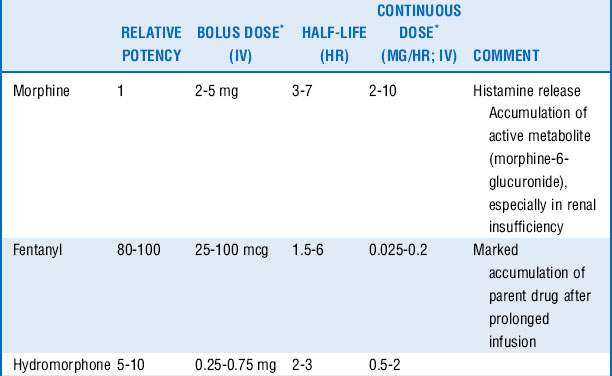
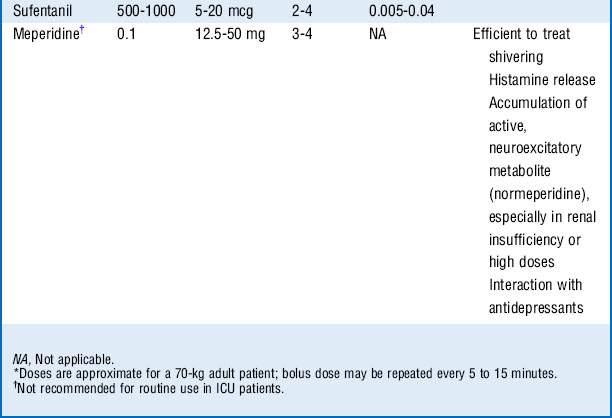
Morphine, fentanyl, hydromorphone, and sufentanil are the analgesic agents most commonly used and recommended in the ICU (Table 72-1).
8 How do you decide which opioid to use?
 Morphine is a naturally occurring, relatively hydrophilic opioid with a long clinical history and therefore familiarity with its use. The onset of action is slow (effect site equilibration time 15-30 minutes), and duration of action is 2 to 4 hours. However, it has relatively rapid hepatic clearance and tends not to accumulate because of its water solubility, which limits the volume of distribution, although glucuronide metabolites with sedative-analgesic properties may accumulate in the setting of renal insufficiency.
Morphine is a naturally occurring, relatively hydrophilic opioid with a long clinical history and therefore familiarity with its use. The onset of action is slow (effect site equilibration time 15-30 minutes), and duration of action is 2 to 4 hours. However, it has relatively rapid hepatic clearance and tends not to accumulate because of its water solubility, which limits the volume of distribution, although glucuronide metabolites with sedative-analgesic properties may accumulate in the setting of renal insufficiency.



10 Which other opioids should be avoided in the ICU for routine analgesia?



11 How should opioids be administered for acute pain management in the ICU?



14 What are the side effects of opioids? (See Table 72-2.)
| Central nervous system | Miosis Euphoria, dysphoria, sedation Addiction |
|---|---|
| Pulmonary | Respiratory depression Muscle rigidity (especially highly lipid-soluble opioids) |
| Cardiovascular | Bradycardia, hypotension |
| Gastrointestinal | Nausea, emesis Constipation, ileus |
| Urogenital | Urinary retention Antidiuretic hormone release (water retention) |
| Other | Histamine release: flushing, tachycardia, hypotension, bronchospasm Pruritus |
15 What is the role of nonopioid analgesics in the ICU, and what are their characteristics?
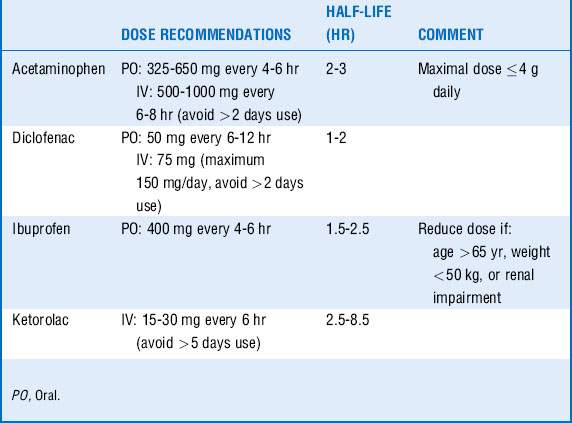
Acetaminophen and NSAIDs have been shown to decrease the need for opioids and are particularly effective in reducing muscular and skeletal pain. They are often more effective than opioids in reducing pain from pleural or pericardial rubs, a pain that responds poorly to opioids. Basic pharmacology is summarized in Table 72-3.
16 What are the side effects of nonopioid analgesics?
 Acetaminophen may be potentially hepatotoxic, especially in patients with depleted glutathione stores. Therefore acetaminophen should be avoided in acute liver failure, and the drug should be maintained at less than 2 g/day in patients with a significant history of alcohol intake or poor nutritional status.
Acetaminophen may be potentially hepatotoxic, especially in patients with depleted glutathione stores. Therefore acetaminophen should be avoided in acute liver failure, and the drug should be maintained at less than 2 g/day in patients with a significant history of alcohol intake or poor nutritional status.

20 Is epidural analgesia safe in the setting of deep vein thromboprophylaxis?
Regional anesthesia may be performed in this setting, although practitioners are advised to follow the guidelines of the American Society of Regional Anesthesia and Pain Medicine (www.asra.com) and be vigilant for the development of epidural hematoma. If low-dose unfractionated heparin is being used, needle placement and/or catheter removal should be done ≥ 2 hours after discontinuing heparin, and reheparinization may be started ≥ 1 hour after an uncomplicated epidural insertion. If fractionated low-molecular-weight heparin (LMWH) is being used in prophylactic doses, a waiting period of ≥ 12 hours for any neuraxial technique should be applied after the last dose of LMWH, and the next LMWH dose should be given ≥ 2 hours after an uncomplicated procedure.

1 Bonnet F., Marret E. Influence of anaesthetic and analgesic techniques on outcome after surgery. Br J Anaesth. 2005;95:52–58.
2 Domino E. Taming the ketamine tiger. Anesthesiology. 2010;113:678–684.
3 Jacobi J., Fraser G.L., Coursin D.B., et al. Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med. 2002;30:119–141.
4 Mehta S., McCullagh I., Burry L. Current sedation practices: lessons learned from international surveys. Crit Care Clin. 2009;25:471–488.
5 Riker R.R., Shehabi Y., Bokesch P.M., et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA. 2009;301:489–499.
