Other cranial nerves
Face, motor and sensory
Trigeminal nerve (5th)
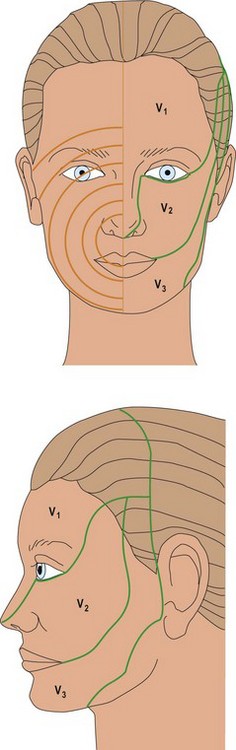
Facial sensation is supplied by the trigeminal nerve (Fig. 1), which has three branches:
Facial nerve (7th)
Look at the patient’s face for asymmetries. Compare the blink rate.
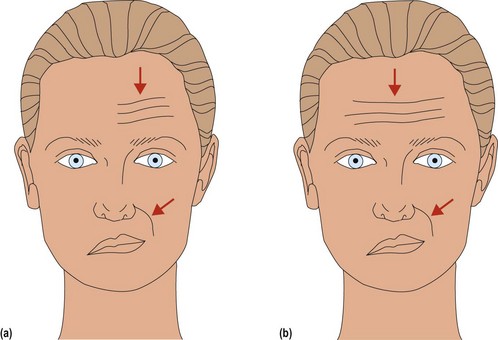
To test facial nerve function, ask the patient to look up at the ceiling (look at the frontalis), screw up the eyes (look at the orbicularis oculi), to whistle and show the teeth. Three patterns of abnormality are seen (Fig. 2):
Bilateral facial weakness is difficult to spot. The facial nerve also supplies (i) the stapedius, so LMN 7th can lead to hyperacusis (noises sound particularly loud); (ii) taste to the anterior two-thirds of the tongue, so LMN 7th can lead to altered taste; and (iii) the lacrimal and parotid glands, so aberrant recovery can lead to crocodile tears (crying when hungry).
Hearing and vestibular function (8th)
Hearing can be tested at the bed side in several ways. The volume of a sound can be compared between ears, for example using a whisper, a tuning fork or a ticking watch. If the hearing is impaired unilaterally, the Weber and Rinne tests will determine whether this is conductive or sensineural (Box 2).


Vestibular function is assessed by looking at eye movements, gait and coordination.
Mouth, tongue and palate (9th, 10th, 12th)
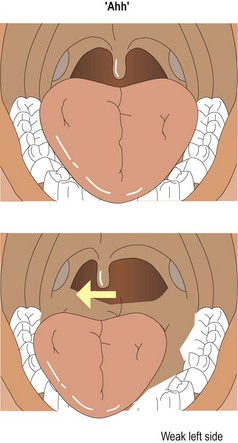
The vagus nerve has many functions: the parasympathetic supply to the stomach, upper gastrointestinal tract and heart, the supply to the larynx, muscles of deglutition and the palate. Palatal movement can be assessed by asking the patient to say ‘Ahh’. The uvula normally lifts centrally; unilateral weakness causes the uvula to be pulled to the good side, and bilateral lesions mean the uvula does not lift (Fig. 3).
Dysarthria
Dysarthria is a distortion of the articulation of speech. Listen to speech for a variation in tone, melody and rhythm. Phrases such as ‘yellow lorry’ test the lingual sounds, while ‘baby hippopotamus’ tests the labial sounds. The abnormalities are classified in Table 1.
| Clinical features | |
|---|---|
| Spastic | Laboured speech, with slow tongue and lip movements |
| Cerebellar | Slurred as if drunk; staccato with loss of normal variation of emphasis, as if scanning a poem |
| Extrapyramidal | Quiet and monotonous, running out of steam before the end of the sentence |
| Lower motor neurone, neuromuscular junction and muscle | Normal rhythm, difficulty with sounds depends on affected muscle groups: tongue – sound t; face – sound b (think ventriloquist); palate – sound c or k (as if patient has a bad cold) |




