[level-membership-for-radiology-category] Favors distal small bowel (SB) and colon



• Mycobacterial













 affecting most of the small bowel (SB).
affecting most of the small bowel (SB).
 . The colon
. The colon  is spared. Endoscopy and biopsy confirmed cytomegalovirus (CMV) enteritis.
is spared. Endoscopy and biopsy confirmed cytomegalovirus (CMV) enteritis.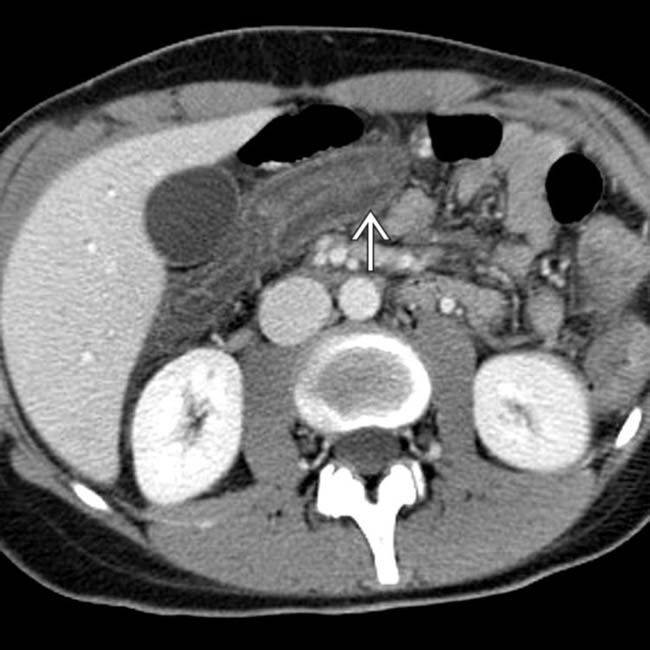
 but no hyperenhancement of the mucosa.
but no hyperenhancement of the mucosa.
 , proven to be due to CMV, which may induce ischemic injury to both the SB and colon in immunocompromised patients.
, proven to be due to CMV, which may induce ischemic injury to both the SB and colon in immunocompromised patients.IMAGING
General Features
• Best diagnostic clue
 Cytomegalovirus (CMV): Mucosal hyper- or hypoenhancement; submucosal edema
Cytomegalovirus (CMV): Mucosal hyper- or hypoenhancement; submucosal edema
 Mycobacterial
Mycobacterial
Cytomegalovirus (CMV): Mucosal hyper- or hypoenhancement; submucosal edema






 Mycobacterial
Mycobacterial























































 .
.
 . CMV colitis infects an immunocompromised host with a virus that causes vasculitis.
. CMV colitis infects an immunocompromised host with a virus that causes vasculitis.
 and mesenteric adenopathy
and mesenteric adenopathy  .
.
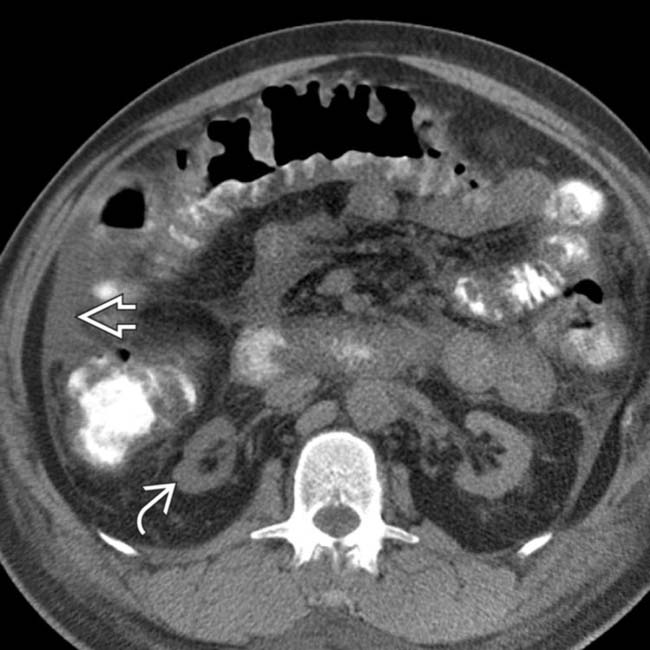
 and large bowel
and large bowel  , along with mesenteric lymphadenopathy
, along with mesenteric lymphadenopathy  . Cryptosporidium was the causative organism and typically causes diarrhea.
. Cryptosporidium was the causative organism and typically causes diarrhea.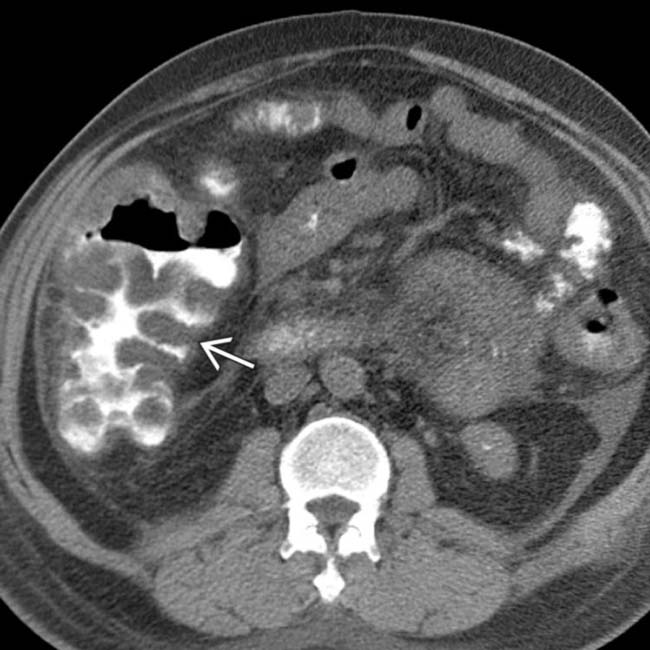
 .
.
 and mesenteric edema. Note the atrophic native kidneys
and mesenteric edema. Note the atrophic native kidneys  . In spite of prompt diagnosis and treatment, the colitis progressed to perforation and emergency colectomy.
. In spite of prompt diagnosis and treatment, the colitis progressed to perforation and emergency colectomy.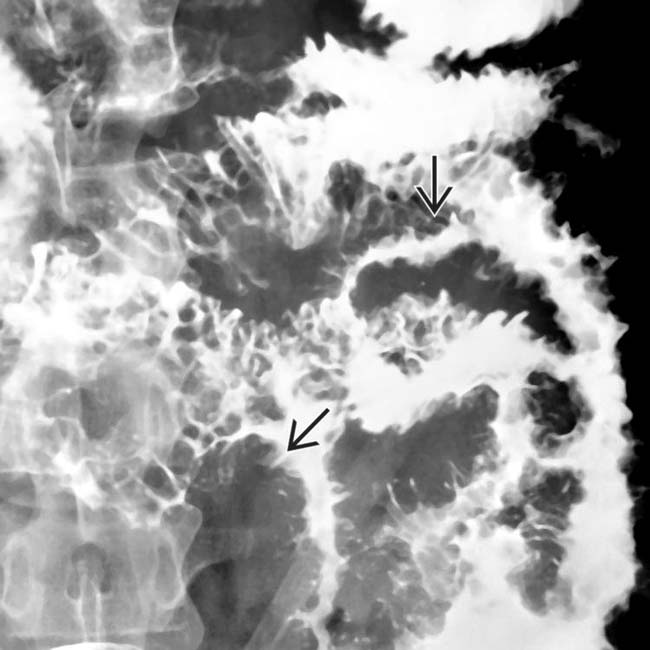
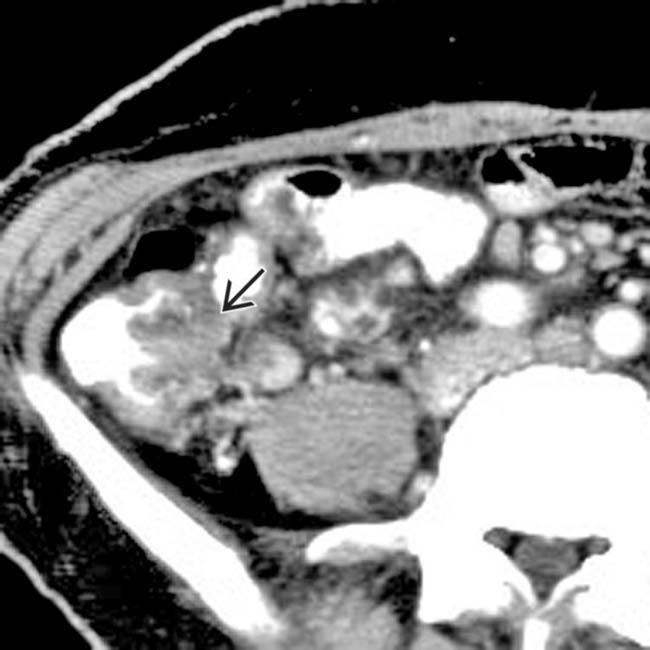
 in this patient with advanced cryptosporidiosis of the small bowel.
in this patient with advanced cryptosporidiosis of the small bowel.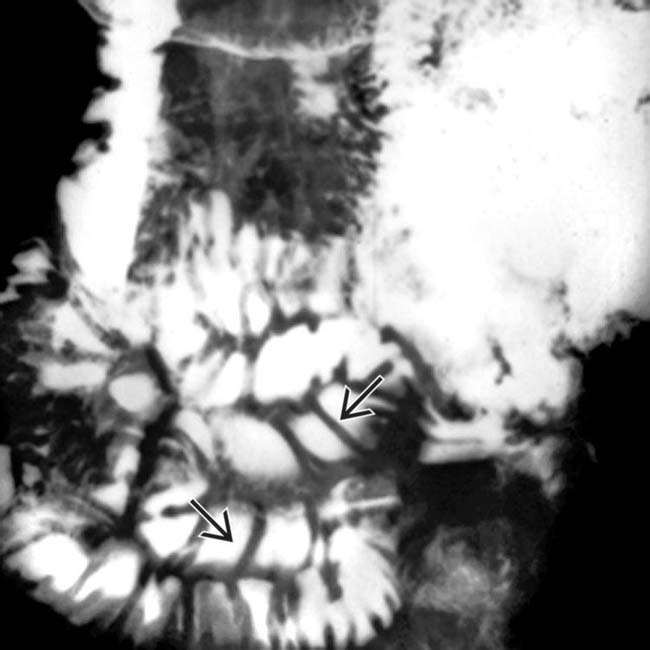
 in this patient with early cryptosporidiosis of the small bowel.
in this patient with early cryptosporidiosis of the small bowel.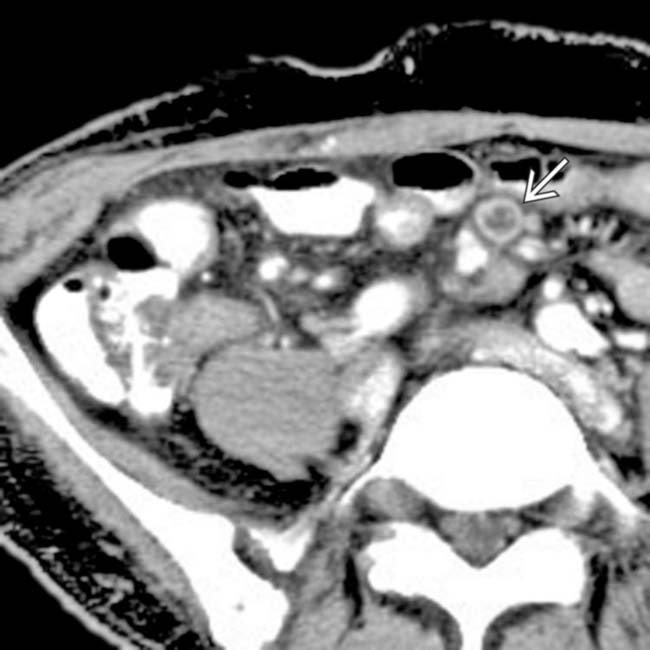
 .
.
 .
.
 .
.
 from antral CMV gastritis.
from antral CMV gastritis.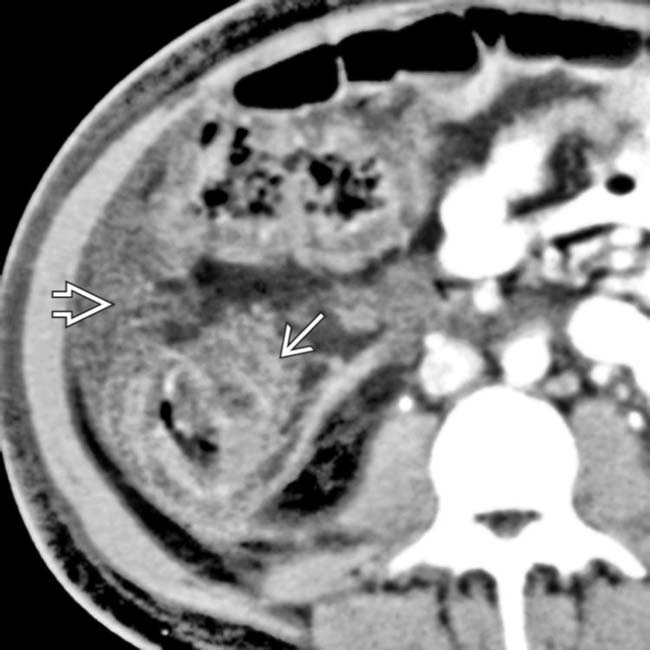
 with pericolonic soft tissue stranding
with pericolonic soft tissue stranding  .
.
 from CMV colitis.
from CMV colitis.[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Favors distal small bowel (SB) and colon
• Mycobacterial
affecting most of the small bowel (SB).. The colon is spared. Endoscopy and biopsy confirmed cytomegalovirus (CMV) enteritis. but no hyperenhancement of the mucosa., proven to be due to CMV, which may induce ischemic injury to both the SB and colon in immunocompromised patients.IMAGING
General Features
• Best diagnostic clue
Cytomegalovirus (CMV): Mucosal hyper- or hypoenhancement; submucosal edema
Mycobacterial
 Bacterial (Clostridium difficile colitis, Campylobacter, and others)
Bacterial (Clostridium difficile colitis, Campylobacter, and others)
Cytomegalovirus (CMV): Mucosal hyper- or hypoenhancement; submucosal edema
Mycobacterial
Bacterial (Clostridium difficile colitis, Campylobacter, and others)
– Distribution
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
