html xmlns=”http://www.w3.org/1999/xhtml” xmlns:mml=”http://www.w3.org/1998/Math/MathML” xmlns:epub=”http://www.idpf.org/2007/ops”>
Introduction
Recent trends in health-care delivery have dramatically increased the frequency of office based surgical procedures. Office procedures have quickly become more accessible and prevalent as technology, physician comfort, and reimbursement have reinforced this paradigm shift. Surgical procedures such as dilation and curettage, hysteroscopy, loop electrosurgical excision procedures, and global endometrial ablation are particularly well suited to an office setting provided the surgeon’s skill set and patient selection are considered. Patient preference, medical history, pain tolerance, anatomy and anxiety among other factors must be evaluated in selecting patients for surgical management in the office. For some patients, the office may provide a more comfortable and less intimidating setting while limiting cost and reducing exposure to hospital acquired infections. Time management, logistics, and administrative burdens may also be more favorable both for patients and providers in the office versus a hospital surgical suite. Despite the migration of some procedures out of a more formal surgical setting, attention to quality of care, physician competency, and patient safety remains paramount and must be equivalent irrespective of the chosen setting.[1]
Several aspects of safe surgical care are universal irrespective of the facility in which such care is delivered. Although not historically implemented in the office environment, credentialing and privileging of providers for surgical procedures should be part of a culture of safety in offices providing invasive care.[1] Although the office setting may allow for less paperwork, a detailed patient history and physical including attention to allergies, medications, bleeding dyscrasias, and surgical risk factors are still required preparations.[1] Informed consent is a universal standard and must not be approached more casually for office based surgical procedures. Consent is a process and requires more than a signed form to ensure the patient is fully prepared for the proposed surgery. The surgeon must ensure that patients are aware of and agree with the procedure, its possible complications, the anticipated level of discomfort, the potential for aborting in medias res, and the option for choosing a hospital or surgery center instead of the office. Though the tenets of care are similar, a patient planning for surgery in the office must understand the limitations and nuances of office care. Ambulatory Care National Patient Safety Goals (NPSG) established by the Joint Commission provides an excellent framework for surgical safety in the office setting. Fundamental elements of the NPSG are patient identification, attention to medication safety, patient history and documentation, a preoperative verification process, and the intraoperative time out.[2] Perioperative patient identification and confirmation of surgical plans should follow well established operating room protocols and practices. A reliable mechanism for specimen management and result tracking must be in place. Checklists are very useful adjuncts to safe patient care, verification of preparation, and compliance with office procedures.[1]
D&C/Hysteroscopy
Hysteroscopy is an outpatient surgical procedure particularly amenable to safe and convenient delivery in the office setting. Such procedures may offer prompt diagnostic, and in some cases, therapeutic benefits such as the identification and removal of endometrial polyps. Patients suspected to have submucosal myomas would typically be less ideal candidates for office surgery unless resection was not intended. Office hysteroscopy also provides the option of transcervical tubal sterilization procedures – currently the Essure®. Dilation and curettage (D&C) for missed abortion is also easily provided in the office. In many practices, office based D&C offers the additional benefit of readily available sonography for guidance of the cannula or curette, which avoids perforation and ensures complete evacuation or lesion retrieval. Global endometrial ablation by several methods lends itself to satisfactory delivery in the office. The authors prefer to pair hysteroscopy with all office endometrial ablations, which may add some degree of safety to the “blind” methods for the global endometrial ablation commonly in use. A sample medication algorithm for hysteroscopy and similar procedures is listed in Table 7-1. A typical equipment list for such procedures follows in Table 7-2.
Hydrocodone or oxycodone 1–2 tablets PO Promethazine 25 mg PO or ondansetron 8 mg PO Ketorolac 60 mg IM
Ibuprofen or another NSAID Hydrocodone or oxycodone prn |
|
Careful patient selection is prudent, and while postmenopausal and nulliparous patients may be safely evaluated by hysteroscopy in the office, a severely stenotic cervix or highly anxious patient should give the surgeon pause in the planning process. If the patient does not want her case in the office, the surgeon does not want her case in the office. Likewise, morbidly obese patients may be better served with a hospital procedure if medical complications are a concern or hyperflexion of the thighs is required to adequately access the cervix. Patients with cardiac or pulmonary disease and those with a complicated medical history should be carefully considered before offering surgical procedures in the office setting.
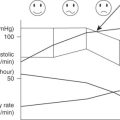
In the absence of plans for sedation, patients are not generally nil per os (NPO) and intravenous access is typically optional in most clinical situations. However, patients may be managed with more or less aggressive anesthesia protocols on an individual basis. In these authors’ experience, the “awake” patient may provide some degree of protection against the risk of perforation versus the patient under heavy sedation or general anesthesia where the surgeon’s tactile sense may be the only preventive measure. Pulse oximetry is an excellent monitoring device for instantaneous patient assessment throughout the surgical process. Some offices may utilize an anesthesia provider for sedation, thus making for a more outpatient surgery center experience. This approach is beyond the perspective of this chapter and does require a more rigorous medical screening process and more conservative perioperative management (NPO, IV access, supervised recovery).
Preoperative cervical ripening with misoprostol 12–24 hours prior to transcervical surgery often facilitates or eliminates the cervical dilation portion of the procedure. Patients are dosed with analgesics 30–60 minutes preoperatively. Oral oxycodone or hydrocodone, oral promethazine or ondansetron, and IM ketorolac in our practice are typical, although protocols vary considerably. Anxiolytics may be beneficial in some cases with use tailored to the individual patient. As with any surgical procedure, a time out is completed and the patient’s antiseptic preparation will vary by surgeon preference. We use betadine or chlorhexidine to cleanse the cervix and vagina for hysteroscopy or D&C with drapes limited to either side of the vulva. Some providers may opt to include antiseptic cleansing of the vulva and thighs followed by a more formal draping process, but infection rates are low with either approach. In fact, the rates of infection are so low that many surgeons do not administer prophylactic antibiotics as a routine for office hysteroscopy.[3] Oral doxycycline or clindamycin may be administered if prophylaxis is desired. A cervical or paracervical block is a useful adjuvant, typically using 10 cc–15 cc of 1% xylocaine. While the block is evolving, the previously inspected and assembled surgical instruments are readied for use.
Office dilation and curettage can be very useful for both expedient management and patient convenience. As noted earlier, preoperative cervical ripening with misoprostol the day prior to surgery eases the cervical dilation portion of the procedure. In the case of a missed abortion, this ripening may cause undesirable cramping and bleeding. As previously mentioned, patients’ may be dosed with analgesics 30–60 minutes preoperatively. Oral oxycodone or hydrocodone, oral promethazine or zofran, and IM ketorolac are commonly utilized. Anxiolytics may useful depending upon the patient. The D&C is performed in the usual manner following placement of a paracervical block using 10 cc–15 cc 1% xylocaine. The cervix is secured with a single tooth tenaculum and the os (opening) is dilated if necessary to accommodate a sharp currette or suction cannula. A 6 mm–7 mm suction cannula directed by sonography provides a safe and effective means of accomplishing surgical evacuation of most incomplete or missed abortions while minimizing risk of perforation or retained gestational tissue. Sharp curettage may be similarly utilized though often with greater patient discomfort. Several passes may be required, but the advantage of ultrasound guidance for the procedure is verification of complete evacuation without excessive endometrial trauma or risk of perforation. Perioperative hemorrhage is uncommon, but may be effectively treated with fluid resuscitation and 0.2 mg IM methylergonovine or 400 mcg–800 mcg misoprostol rectally. Intrauterine balloon via Foley or Bakri™ device may be an effective management of hemorrhage in extreme cases.
For simple diagnostic hysteroscopy, premedication and preparation are completed as previously detailed, and the hysteroscope is readied for insertion by priming the irrigation fluid though the tubing and completing a white balance for the camera. A single tooth tenaculum is placed on the anterior or posterior ectocervix. The cervix is then gently dilated to accommodate the hysteroscope as necessary. Preoperative misoprostol ripening may obviate the need for cervical dilation, especially in the parous patient. In fact, some patients may require use of the tenaculum to buckle the cervix around the hysteroscope to adequately seal the scope for uterine distension. The hysteroscope is advanced into the endometrial cavity under direct and hysteroscopic visualization. The findings may be documented by photography or by videography. Once the procedure is accomplished and the hysteroscope withdrawn, endocervical and endometrial tissue samples for histology may be obtained as clinically indicated. A repeat hysteroscopy may be performed following curettage to confirm adequate sampling of the endometrium or sampling of a particular lesion targeted for the procedure. Upon completion, the tenaculum and speculum are withdrawn and the patient is gradually returned to a supine and then sitting position.
Endometrial ablation
A global endometrial ablation in the office follows a similar preparation and implementation as described for hysteroscopy. If well screened for tolerance, motivation, and medical risk factors, the office ablation can be a very satisfying approach for clinician and patient. Preparing patients emotionally for the experience is critical. Once the patient has been dosed with preoperative narcotic, antiemetic, and NSAID as detailed earlier, the procedure is initiated with visualization of the cervix and paracervical block placement. The cervix is dilated to accommodate the hysteroscope if a cavity assessment was planned prior to the ablation. A preablation and postablation hysteroscopy is helpful in our opinion to evaluate the anatomy, confirm the trajectory for safe entry into the endometrial cavity, verify cavity dimensions, and to confirm a thorough ablative result upon completion. Endometrial sampling is accomplished if not previously performed. The ablation is then completed with the surgeon’s preferred device (balloon, radiofrequency, cryoablation). Due to the potential for vagal hypotension and bradycardia, continuous pulse oximetry is a prudent choice during such a procedure. Such patients may require intramuscular atropine in severe cases.
Hysteroscopic sterilization
Essure and Adiana for tubal sterilization were developed with the expectation of in-office placement for most patients desiring this contraceptive approach. The Adiana is no longer marketed or available, but the Essure is a very effective and well-tolerated office sterilization procedure. It is so well tolerated that in our experience, some may only require a paracervical block in patients motivated to avoid all other perioperative medications for personal reasons. It is a safe and viable option for women who have completed childbearing. Advantages include the ability to safely perform the procedure in the office setting with minimal or no anesthesia, avoidance of intra-abdominal entry, and the avoidance of incisions. Appropriate patient selection and counseling is mandatory prior to the procedure (Table 7-3). Complications of Essure placement include tubal perforation (1%–3% in the Essure clinical trials), improper coil placement (intraperitoneal placement in 0.5%–3% and other improper placements in 0.5%) and expulsion of the occlusion device (in 0.4%–2.2%). A retrospective study of 4, 306 office-based Essure placements demonstrated its efficacy and safety with 98.5% of patients having successful bilateral coil placement and a low overall complication rate of 2.7%, the most common of which was vasovagal syncope.[4, 5] Patients should be counseled on the possibility that bilateral coil placement may not be achievable for each patient, therefore, contingency plans should be reviewed in the event that bilateral placement is not achieved. Known contraindications to the procedure should also be identified prior to the procedure (Table 7-4).[6]
|
1. Sterilization is considered permanent and not meant for reversal. 2. The details of the procedure, including the risks and benefits of the procedure itself and of analgesia should be reviewed with the patient. Some of the risks associated with hysteroscopy and Essure® include fluid overload, infection, cervical injury, uterine or tubal perforation, insert expulsion, cramping, pain, nausea, vomiting, dizziness, light-headedness, vasovagal response, vaginal bleeding/spotting. 3. Five-year failure rate for Essure is 1.64 pregnancies per 1,000 procedures, including the possibility of ectopic pregnancies. 4. The risk of regret, which is higher in women who are younger than 30 years, regardless of parity or marital status, should be discussed. 5. Alternative methods of contraception such as long-acting reversible methods and vasectomy should be reviewed. 6. Sterilization does not protect against sexually transmitted infections; therefore, condom use should be encouraged. 7. The patient needs to use an alternative method of contraception until tubal occlusion can be confirmed by hysterosalpingogram, typically three months after the procedure. 8. Regulations mandating time interval from consent to procedure, if applicable. |
|
Ideally, the patient is scheduled during the early proliferative phase of her menstrual cycle to ensure a thin endometrium. Alternatively, she may be pretreated with combined oral contraceptives or progestins. If indicated, she may be provided with a single dose of misoprostol 200 mcg–400 mcg the night prior to the procedure for cervical preparation. A negative pregnancy test is required. The patient is given NSAIDs (e.g., IM ketorolac) one hour prior to the procedure. An anxiolytic may be provided 30 minutes prior to the procedure. IV sedation may also be provided if desired. The patient is prepped for hysteroscopy as described previously. The uterine cavity is distended with prewarmed saline at a minimum infusion pressure to visualize both tubal ostia and prevent tubal spasm. The procedure should be aborted if the tubal ostium is not visible or accessible or if either ostium does not appear to be patent. For cost containment, it is prudent to delay opening the Essure packaging until visualization of both tubal ostia is confirmed. The speculum may be removed following introduction of the hysteroscope into the uterine cavity. The introducer is inserted through the sealing cap on operating channel of the hysteroscope. The delivery catheter is then inserted through the introducer and under direct visualization; the catheter is advanced through the operating channel into the proximal fallopian tube with gentle, constant forward movement to prevent tubal spasm. If excessive resistance is encountered, the procedure should be terminated to avoid uterine perforation or placement into a false passage. The proximal end of the black positioning marker is aligned with the ostium. The delivery system is stabilized against the hysteroscope to prevent inadvertent forward movement. The thumbwheel is rotated on the handle toward the surgeon until the wheel no longer rotates. The delivery catheter and the black positioning marker will move away from the tubal ostium and disappear into the operating channel. The gold marker should be just outside the ostium and the distal tip of the green release catheter should be easily visualized. If more than 1 cm of the insert is visible in the uterus, the insert can be repositioned by moving the entire system further into the tube. The button on the purple handle is pressed, thus enabling one to rotate the thumbwheel further for insert deployment. When the thumbwheel cannot be rotated any further and the expanded outer coils are visible, the delivery system may be removed. The same procedure is performed on the opposite tube. Ideally, three to eight expanded outer coils should be trailing into the uterus. The number of visible coils should be recorded. The patient is advised to call for fevers, excessive vaginal bleeding, or severe or persistent pain. It is imperative that a hysterosalpingogram (HSG) be performed three months after placement to confirm tubal occlusion and that back-up contraception is used until then.[7]
LEEP
The loop electrosurgical excision procedure (LEEP) is another procedure that may readily be performed in the office setting. It involves removal of the transformation zone of the cervix and is currently the most common method for the treatment of cervical intraepithelial neoplasia CIN 2,3. It is typically performed in the office under local anesthesia. It is well tolerated by patients and offers the advantage of less bleeding and smaller volume of tissue loss compared to cold knife conization.[8]
Counseling the patient adequately on the risks associated with the procedure such as bleeding, infection, discomfort, potential cervical stenosis, implications for future pregnancies including the risk of preterm birth is necessary. The potential for positive margins requiring repeat excision should also be reviewed with the patient.
An insulated speculum with suction via intravaginal tubing is placed in the vagina ensuring good visualization of the cervix. The cervix is cleansed and acetic acid or Lugol’s solution is placed on the cervix to better identify the lesion(s) for excision. A paracervical block using 1% lidocaine with or without epinephrine is injected circumferentially into the cervix. Studies performed to evaluate pain relief for women undergoing loop excisions found that intracervical injection of local anesthetic with a vasoconstrictor appears to provide optimum analgesia for treatment.[9] The patient is grounded appropriately. An appropriately sized wire loop is chosen and attached to the cautery instrument that provides a cutting current. The appropriate settings are chosen and set into the electrosurgical generator. Some providers use a blended current, which mixes cutting and coagulating currents (one can set the generator at 30 W–40 W on blend 1). It is important to note that the higher the blend, the more the coagulating current and the greater the thermal damage. Some providers use a pure cutting current at 80 W. Normal saline can be applied to the exocervix to rehydrate the tissue and decrease the risk of the loop electrode sticking to the tissue. The loop is then carefully passed around and under the transformation zone, thus excising it fully. Care should be taken to move the loop along the tissue properly to obtain an appropriate specimen. If the loop is passed too quickly through the cervix, the loop can drag, bend, or adhere to the tissue, which may result in a shallower excision than intended. If the loop is passed too slowly through the tissues, there may be excess thermal damage to the specimen. If the lesion extends into the endocervical canal, additional tissue may be excised using a smaller diameter rectangular loop or a top hat. Once the specimen is obtained, it is carefully removed in the correct orientation. A suture placed at the 12 o’clock position on the excised specimen will better orient the specimen for histopathologic examination.
Hemostasis of the LEEP bed typically requires coagulation using the 5 mm ball electrode on a coagulating setting. Use of Monsel’s (ferric subsulfate) paste/solution will also aid in hemostasis. If bleeding continues despite these measures, one can place a suture at the 3 o’clock and 9 o’clock positions at the distal point of the cervix to decrease the pulse pressure from the cervical arteries. Gelfoam® may also be placed at the base and a suture tied across the front of the cervix to keep the Gelfoam in place.[8, 10, 11]
After the procedure, the patient is then advised to avoid intercourse and observe pelvic rest for two to four weeks. The patient is typically seen in the office six weeks after the procedure. The patient is also advised of signs to watch for including: abnormal looking vaginal discharge and excessive vaginal bleeding.
Vulvar biopsy
The investigation of a vulvar lesion or persistent irritation will often include a biopsy. This is typically an office procedure in all but the most hesitant of patients or in the case of a very extensive lesion. Vascular lesions may also be better served in a better equipped surgical setting. Any lesion of uncertain etiology, irritation that has failed medical or expectant therapy, abnormal pigmentation, or tissue suspicious for atypia warrants a biopsy for histologic evaluation. Targeting biopsies when atypia is suspected may improve with the application of 5% acetic acid and magnification via a colposcope.
Vulvar tissue samples may be obtained as a punch biopsy (Keyes punch), shave biopsy, or elliptical excisional biopsy. Location may dictate the diagnostic approach and anesthetic options. Topical xylocaine-prilocaine may provide adequate anesthesia for some patients, but the typical biopsy is performed with local subcutaneous xylocaine anesthesia. Take care during injection to avoid distorting the targeted tissue with an excessive volume of anesthetic. A deeper subcutaneous injection of xylocaine may elevate the lesion to improve access for a shave biopsy. Excessive infiltration may obscure the targeted tissues and compromise accurate sampling.
Once a antimicrobial preparation has been preformed and adequate local anesthesia is established, a punch biopsy is obtained by stabilizing the skin between the thumb and forefinger while cutting tissue perpendicularly into the skin with a Keyes punch or with a cervical biopsy instrument such as a Kevorkian or Tischler cervical biopsy punch. When using a cervical punch biopsy device on the vulva, avoid skimming the epidermis when closing the jaws by applying pressure against the targeted tissue prior to closing the device to obtain a more substantial biopsy. A Keyes punch cuts a cylindrical biopsy using a simple twisting motion – clockwise and counterclockwise perpendicular to the vulvar surface. The cored specimen may require forceps to retrieve and scissors or a scalpel to divide at the base. A localized lesion highly suspicious for atypia or malignancy should be excised with peripheral margins of normal tissue if possible. This may require an elliptical excision if the lesion is larger than a few millimeters. Using a scalpel and stabilizing the vulvar skin in the linear direction of the incision, an elliptical incision around the lesion may allow for full exision, but will likely require suture closure for approximation and hemostasis.
Direct pressure may accomplish adequate hemostasis for small biopsy sites, but the vascularity of the vulva typically results in a magnitude of bleeding which may exceed expectations even in the most minimal of excisions. Silver nitrate or ferrous subsulfate (Monsel’s solution) applied to the biopsy site followed by direct pressure will achieve hemostasis in most cases. If bleeding persists, place simple interrupted or figure-eight stitches using fine (3–0 or 4–0) catgut or polyglactin suture. Application of a folded gauze or sanitary pad to be held in place by the patient’s underwear may avoid subsequent bleeding or soiled clothing.
Nexplanon
The Nexplanon® device is a long-term reversible contraceptive method that is implanted subdermally in the upper arm. It is easily placed and removed in the office setting. It consists of a single 4 cm radio-opaque rod that contains 68 mg of etonorgestrel that is slowly released over a three-year period. Careful counseling prior to placement is important and should include the risks of infection, scarring, hematoma, irregular/breakthrough bleeding, failure, migration, expulsion, and risks of deep insertion including difficult removal requiring removal in the operating room and the risk of neurovascular injury. Prior to placement, one should ensure that there are no contraindications to progesterone use and that pregnancy is excluded.
When placing the Nexplanon device, the patient is laid in supine position with the nondominant arm flexed at the elbow and externally rotated with the wrist parallel to the ear and the hand next to the patient’s head. The insertion site is identified and marked. This is located on the inner side of the nondominant upper arm about 8 cm–10 cm or 3 in–4 in above the medial epicondyle of the humerus in the sulcus between the biceps and the triceps. A second mark is made several centimeters proximal to the initial mark to serve as a guide during the insertion process. The insertion site is cleansed with an antiseptic solution such as Betadine. Local anesthesia such as 1% lidocaine is injected along the intended track. The protection cap on the Nexplanon applicator should be easy to remove and the presence of the device can be confirmed by visualizing the white-colored implant by looking into the tip of the needle. The skin at the insertion site is stretched with one’s free hand. The skin is then punctured with the tip of the needle angled about 30 degrees. The applicator is then lowered to a horizontal position and the entire needle is inserted along the track. It is important to lift the skin as the needle is inserted into the track to ensure subdermal placement. A seated position and looking at the applicator from the side is the best position to see the movement of the needle. With the applicator in place and stabilized, the purple slider is pushed and slid back fully until it stops to deploy the device. The implant will now be in place and can be palpated in its subdermal position. It is important not to touch the purple slider until this point. The implant should be palpated by the physician and the patient. Steri-Strips and Mastisol should then be applied to the puncture site; this can be removed in three to five days. A pressure bandage using sterile gauze is then applied to minimize bruising, the patient is instructed to remove this in 24 hours.
To remove the Nexplanon device, it is important to know the exact location of the implant on the arm, as verified by palpation. The distal end of the implant (closest to the elbow) is marked and cleaned with an antiseptic solution. The incision site is anesthesized with local anesthesia, the anesthetic is injected under the implant to keep the implant close to the skin. A longitudinal incision toward the elbow is made with the scalpel on the distal end of the implant. The implant is gently pushed toward the incision site until the tip is visible. The implant is then grasped with forceps and removed. If it is encapsulated, an incision can be made into the tissue sheath and the implant removed with forceps. If the implant is not visible, forceps could be inserted into the incision and a second pair forceps can be used to dissect the tissue around the implant and grasp the implant for removal. Once removed, the implant is measured (should be 4 cm) to ensure complete removal of the device. If a new implant is desired, it may be placed immediately after the old implant is removed using the same incision. The incision is then closed with Steri-Strips and Mastisol, which may be removed in three to five days. A pressure bandage using gauze is applied to minimize bruising and the patient is instructed to remove this in 24 hours.
If the implant is not immediately palpable, efforts to locate the implant such as two-dimensional x-ray, x-ray computer tomography (CT), ultrasound scanning with a high-frequency linear array transducer (10 MHz or higher), or magnetic resonance imaging (MRI) should be undertaken. If this fails to identify the implant, the company should be called at 1-877-467-5266 to determine etonorgestrel levels. After confirming the location of the implant, removal can be undertaken with ultrasound guidance. Exploratory surgery is not recommended until the exact location of the implant is known. If an implant is deeply inserted, removal should be performed by a health-care provider familiar with anatomy of the arm to avoid injury to deeper neurovascular structures.
Ultrasound utilization
Ultrasound guidance is an invaluable adjunct to office procedures. Specifically, sonography may contribute to the ease and safety of IUD placement, IUD retrieval, endometrial polypectomy, endometrial sampling by directed curettage, and suction evacuation of early pregnancy loss. For difficult IUD insertions (e.g., nulliparous patients or those with a malpositioned uterus), one may consider the use of 400 mcg of intravaginal or oral misoprostol administered 12 hours prior to insertion. Data on the use of intravaginal misoprostol for cervical preparation in IUD candidates have been conflicting. A double blind randomized trial using 400 mcg of intravaginal misoprostol administered three hours prior to IUD insertion showed no difference in patient perception of pain and provider ease of IUD placement.[13] Conversely, a randomized controlled trial using administration of 400 mcg sublingual misoprostol was associated with easier insertion as perceived by the provider and no difference in patient perception.[14] A paracervical or intracervical block using 10 cc–15 cc of 1% lidocaine may also improve patient tolerance.[15] Sonography during or following a difficult IUD insertion may assist with appropriate placement or confirmation of appropriate placement within the uterine cavity. During retrieval of an IUD when the strings are not visible, sonography often makes recovery a simple and easy process. This obviates the need for retrieval by operative hysteroscopy. IUD forceps or Randall stone forceps combined with transabdominal imaging allows for real time visualization of an IUD or polyp for the safest possible entry into the uterus and efficient recovery of the target. A paracervical block is typically helpful for patient tolerance of the procedure and oral or intramuscular analgesia may be appropriate for some patients. Patients with a missed or incomplete abortion may benefit from ultrasound guided suction curettage. A sonogram guided D&C provides the additional benefit of confirmatory imaging immediately preoperatively. This verification is especially helpful for the potential doubt of a patient suffering a miscarriage and in other patients to reassess the location and size of endometrial polyps or pathology. In the author’s experience, the addition of sonography improves efficiency of the evacuation and reduces the risk of perforation by real-time visualization of the cannula or curette throughout the procedure.
Concluding remarks
Surgical care in the office introduces a variety of logistical and safety issues beyond those typical of routine office care. The additional risk of a perioperative complication requires emergency preparedness, which should include staff training, resuscitation equipment, and mock drills. There should be one standard of care for procedures whether in the hospital or ambulatory surgical setting or the office. It is expected that office procedures will only increase over the next few years, and strict attention and diligence to protocols is paramount. This chapter sought to present a few such protocols and safety standards to ensure that patients having procedures in the office for convenience are not compromising safety. Finally, it is the providers’ responsibility to assure that the patient is an appropriate candidate for an office procedure as well as assuring that all office personnel are trained and educated in emergency preparedness if complications arise.