W9 Reconstruction of the Distal Radius Facet by a Free Vascularized Osteochondral Graft
Rationale and Basic Science
Intra-articular malunions of the distal radius should be ideally treated by an outside-in1–5 or inside-out osteotomy,6 in such a way as to restore the normal joint anatomy. Sometimes the degree of damage on the articular cartilage or the degree of comminution is such that an intra-articular osteotomy is no longer an alternative. Currently, the gold standards when the lunate or scaphoid facet cartilage is irreversibly damaged are partial or total arthrodeses.7,8 Partial arthrodeses limit the range of motion and may overload neighboring joints, which may degenerate in the midterm.9
Taking into account that the original problem is the loss of cartilage in the distal radius, a more logical approach was to try to replace it with a similar piece of tissue, rather than to fuse the joint. Giachino and coworkers10,11 resurfaced irreversibly damaged distal radius articular surface by transferring nonvascularized osteochondral grafts from the proximal fibula. Their experience in two cases was positive in the short-term, but the fate of nonvascularized osteochondral grafts has been shown to be unpredictable in other joints.12–15 Ishida and colleagues12 recommend limiting the graft size to 50% of the proximal interphalangeal joint to avoid massive graft resorption. Other studies have found on histology, even with small autogenous osteochondral plugs, the appearance of multiple tidemarks on the deep layer of the cartilage,16 a finding that has been associated with osteoarthritis.15,17
The problem of restoring articular cartilage loss has been widely explored in other fields of orthopaedic surgery. There are several methods for repairing cartilage defects, including microfracture, chondrocyte cultures, mosaicplasty, fresh and frozen allografts, autologous osteochondral grafts, and perichondroplasty, but none of them totally successful.18–24 The fact that the anatomy of the hyaline cartilage is extremely complex and difficult to reproduce was considered by Poole17 as being responsible in part for the failures with these methods.
Cartilage has been said to get its nutrients from the synovial fluid.25–27 Collapse or even total joint disappearance has been shown to occur, however, when a joint or a part thereof is transferred as a nonvascularized graft.28–30 Conversely, vascularized joint transfers do maintain the joint spaces open in the long-term.31,32 Several studies have shown the blood supply of the subchondral bone is important for the nutrition of the bone-cartilage interface or even the deep layers of the hyaline cartilage.17,33 It seems logical to conclude, based on current evidence, that the cartilage’s nourishment via the subchondral blood vessels is also an important issue. It seemed to us important when transplanting a piece of cartilage to include the underlying vascularized subchondral bone. Bone that has been transferred with microsurgical technique has long been shown to maintain its biological and mechanical properties.34 Even reliable growth has been shown to occur when a vascularized epiphysis is included.35,36
My colleagues and I searched for a donor site with similar shape to the distal radius facets, which contained cartilage and a reliable blood supply. This chapter presents our experience on transferring the base of the third metatarsal as a vascularized osteochondral graft.37–39
Anatomy
Twenty fresh feet were dissected under loop magnification for this study. The proximal facet of the base of the third metatarsal, which articulates with the third cuneiform, is pear-shaped, flat or slightly concave, and has a slant of about 5 degrees dorsal to plantar and fibular to tibial. We named this the “principal” facet to distinguish it from several minor ones that exist on both sides of the metatarsal base. One of the latter, located on the dorsofibular aspect, which we named the “accessory facet,” can be advantageously used for reconstructing the sigmoid fossa (Fig. W9-1).
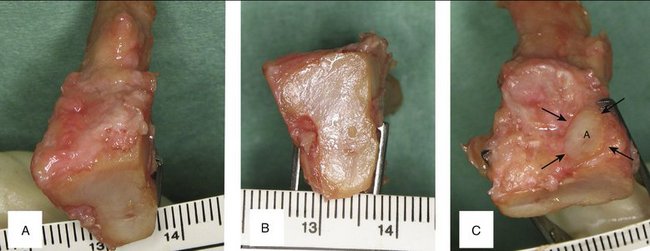
FIGURE W9-1 Anatomical features of the base of the left third metatarsal. A, Bird’s eye view to appreciate the slight inclination toward the second metatarsal. B, Proximal (principal) facet. C, Accessory (peroneal) facet.
(From del Piñal F, García-Bernal JF, Delgado J, et al: Reconstruction of the distal radius facet by a free vascularized osteochondral autograft: anatomical study and report of a case. J Hand Surg [Am]. 2005; 30:1200-1210; with permission from the American Society for Surgery of the Hand.)
The principal facet is 19 mm on its main axis with a maximal width of 12 mm dorsal and 8 mm plantar. Mekhail and associates40 studied the distal radius articular surface. They found the scaphoid facet to be a triangle measuring 18 mm dorsal × 16 mm palmar × 13 mm ulnar, and the lunate facet to be a polygon measuring 10 mm dorsal × 13 mm lateral × 14 mm palmar × 15 mm ulnar. The principal facet is approximately the right size for restoring one of the fossae. The accessory facet is about 8 × 8 mm, and slightly inclined plantarward and tibialward. This is sufficient to restore the dorsal part of the sigmoid facet in Tolat’s type I and II.41 Bearing in mind the three-dimensional shape and slanting of the different facets of the base of the third metatarsal, we can restore a die-punch defect in a single stage by harvesting the contralateral graft (Fig. W9-2).
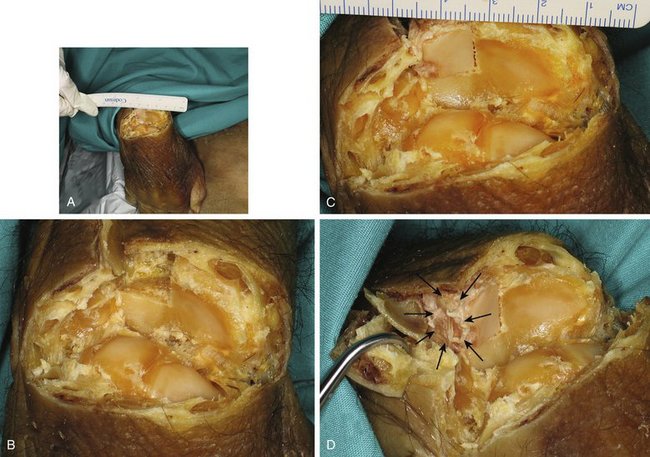
FIGURE W9-2 Simulation in a cadaver of the reconstruction of the malunited die-punch fragment. A, In this specimen, all the dorsal structures have been sharply divided at the radiocarpal level, and the wrist has been flexed to have an unimpeded view of the radius surface. B, Close-up view where the dorsal half of the right lunate facet of the distal radius has been resected in preparation for its reconstruction. C and D, The dorsal half of the left third metatarsal is replacing the dorsal half of the lunate facet of the distal radius. It matches the radius slope in both views, and the accessory facet (arrows) is located in a favorable position for reconstructing the sigmoid facet (when the contralateral metatarsal is selected).
(From del Piñal F, García-Bernal JF, Delgado J, et al: Reconstruction of the distal radius facet by a free vascularized osteochondral autograft: anatomical study and report of a case. J Hand Surg [Am]. 2005; 30:1200-1210; with permission from the American Society for Surgery of the Hand.)
The blood supply to the dorsum of the foot has been studied by several investigators. The classic anatomical description of the dorsalis pedis artery with three lateral branches (proximal lateral tarsal artery, distal lateral tarsal artery, arcuate artery) is rare; it may represent less than 30%.42–45 We found the description of the anatomy of the dorsum of the foot by Cormack and Lamberty42 closely matches our findings. They described a plexus where all the arteries are interrelated in a competitive fashion from where the dorsal intermetatarsal arteries originate (Fig. W9-3A). In all the specimens in our anatomical study, we were able to track a periosteal artery to the dorsalis pedis. In addition, in all of the specimens, the nutrient foramina could be found in the dorsum of the proximal aspect of the third metatarsal. We found that in two thirds of the cases, the distal lateral artery was dominant, whereas in the rest the arcuate was the larger vessel (Fig. W9-3B and C). Variations in vascular anatomy must be kept in mind when harvesting this flap; as is the case in modern perforator-based flaps, deviation of anatomy is the norm. The surgeon has to be prepared to perform a “freestyle” type of harvesting,46 rather than expecting a book type of anatomical findings.
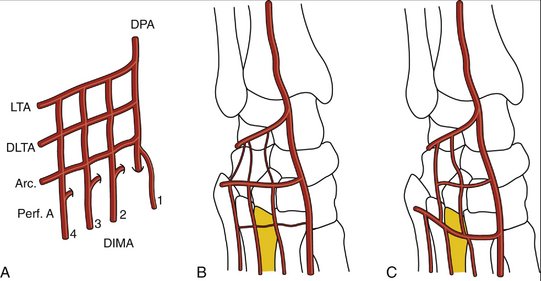
FIGURE W9-3 The blood supply to the dorsum of the foot, and the variations most commonly found (see text for details). A, Classic arterial network. B, Distal lateral tarsal artery dominance (the arcuate vessels are either hypoplastic or absent). C, Arcuate artery dominance (the distal lateral tarsal artery is hypoplastic or absent). Arc, arcuate vessels; DIMA, dorsal intermetatarsal arteries; DLTA, distal lateral tarsal artery; DPA, dorsalis pedis; LTA, lateral tarsal artery; Perf A, perforating arteries.
(From del Piñal F, García-Bernal JF, Delgado J, et al: Reconstruction of the distal radius facet by a free vascularized osteochondral autograft: anatomical study and report of a case. J Hand Surg [Am]. 2005; 30:1200-1210; with permission from the American Society for Surgery of the Hand.)
Indications
The ideal candidate for this operation is a young patient with irreversible damage to the articular cartilage of the lunate or the scaphoid facet of the distal radius. For these instances, the principal facet of the base of the third (or alternatively the second) metatarsal is used. The procedure also is indicated to reconstruct the die-punch malunion. In this instance, the dorsal aspect of the sigmoid fossa is reconstructed by the accessory facet of the base of the third metatarsal (see Fig. W9-2).
Focal cartilage loss (2 to 3 mm) and scarring on the corresponding scaphoid or the lunate’s articular surface are considered a relative contraindication. In a sedentary patient, the procedure may be unwise after the age of 50, but in an active or healthy manual worker we do not see age by itself to be a problem, provided that the patient is a nonsmoker and can tolerate a long operation.
There is no upper time limit for this procedure, provided that the joint surface of the corresponding carpal bone is preserved. This is more likely to occur when the step-off is located in the sagittal crease (the interfacetal ridge) because there is little load transfer in this area47,48 and little risk of wearing out the articular cartilage. The earlier the procedure is done, the better because there is an overload on the healthy cartilage.
Intrafacet step-offs produce not only overload on the unaffected areas,49 but also early erosion of the cartilage of the opposing carpal bone.5,50 Fernandez5 set 6 weeks as the upper limit until after which an intra-articular step-off would have caused irreversible cartilage damage on the opposing carpal bone. Rather than adhering to an exact timeline, I presently assess the joint arthroscopically and decide which operation to perform based on the quality of the cartilage on the radius and carpal surfaces. If both are preserved, we proceed with an arthroscopic-guided osteotomy; if the radius is damaged, but the carpal surface is preserved, we proceed with an osteochondral graft. If both sides of the joints are damaged, we proceed with a partial arthrodesis (Fig. W9-4).
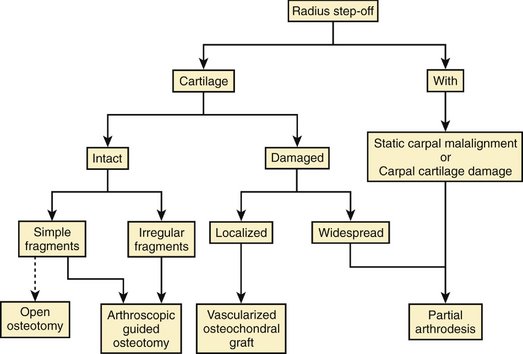
FIGURE W9-4 Treatment algorithm.
A final indication is the central defect that is created during the correction of irregular sagittal gaps/step-offs. In those circumstances after débriding the scarred area, the surgeon creates a secondary defect (Fig. W9-5A). If this is closed directly, without interposing any tissue, the radius would be narrower in the frontal plane, the normal ligamentous restraints of the carpus would be relatively lengthened, and the carpus would translocate ulnarly. This is a painful situation for the patient and the surgeon (Fig. W9-5B). This secondary carpal translocation can be avoided by interposing a vascularized osteochondral graft (Fig. W9-5C).
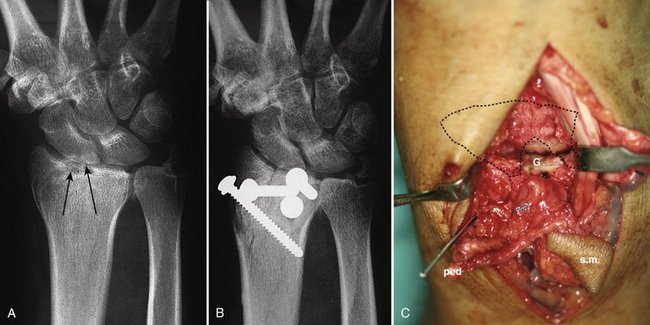
FIGURE W9-5 This patient was treated for a four-part malunion with a classic open outside-in osteotomy technique. A, The lunate fossa was anatomically reconstructed; however, the effect of resecting scarred and multifragmented tissue in the gap on the scaphoid fossa (arrows) entailed a narrower radius. B, In the early x-ray, already an ulnar carpal translocation can be seen. This became painful. (This case predated the vascularized osteochondral graft). C, To avoid this complication in case no. 4 of our series, with a similar problem in the lunate fossa, this was managed interposing a vascularized osteochondral graft (G). ped, pedicle; sm, skin monitor.
Contraindications
The procedure is absolutely contraindicated when the cartilage loss involves the corresponding carpal bone also. Under those circumstances, the metatarsal would face an eroded surface, and early osteoarthritis is to be expected.






