CHAPTER 22 Galeazzi Fracture-Dislocations
Galeazzi fracture-dislocations are defined by fracture of the middle to distal third of the radial diaphysis with simultaneous traumatic disruption of the distal radioulnar joint (DRUJ), resulting in either dorsal or ulnar subluxation/dislocation of the ulnar head from within the sigmoid notch. Although first described by Cooper in 1882,1,2 this complex forearm fracture-dislocation has been credited to Galeazzi,3 who in 1934 reported a series of 18 patients with this injury pattern. Mikic1 proposed that both-bone forearm fractures with concomitant DRUJ dislocation be considered within the spectrum of the classic Galeazzi fracture-dislocation because similar principles of management are applied.
Several early series demonstrated uniformly poor results with nonoperative management, and, as a result, the Galeazzi fracture-dislocation has been referred to as a “fracture of necessity.” Hughston4 reported that nonoperative treatment of the classic Galeazzi lesion resulted in unsatisfactory results in 92% (35 of 38) of patients. Mikic1 reported an 80% failure rate with conservative management in 86 adults with Galeazzi fracture-dislocations due to both inability to control progressive displacement of the radius fracture as well as recurrent subluxation or dislocation of the DRUJ despite cast immobilization. Mikic postulated that rupture of the triangular fibrocartilage complex (TFCC) was the primary cause of redislocations and the poor results observed. Other early series reported similar disappointing results with closed reduction and immobilization.2,5
With advances in surgical techniques to achieve osteosynthesis and soft tissue reconstruction, open reduction and internal fixation (ORIF) has become the standard of care to optimize outcomes after forearm fractures associated with DRUJ disruption. Operative management has yielded satisfactory results in more than 80% of adult patients with these injuries.6–9
Regional Anatomy and Biomechanics
Stability of the forearm, and specifically the DRUJ, is dependent on the presence of dynamic (musculotendinous) and passive (ligamentous) soft tissue stabilizers and, to a lesser extent, osseous anatomy. Bony congruity between the ulnar head and sigmoid notch of the radius contributes only approximately 20% of total DRUJ stability. In the transverse plane, the sigmoid notch is shallow relative to the ulna seat and the radii of their articular seats are disparate; thus, appositional contact is small.10,11 As a result, motion at the DRUJ is predominantly translational—a combination of sliding and rotation. However, its axis of motion remains adjacent to the center of the ulnar head.
Tolat and associates11 analyzed the osseous characteristics of the sigmoid notch and ulnar head in 50 cadaveric specimens in the coronal and transverse planes with multiple articular surface-based measurements. Three midcoronal DRUJ articular types (types I to III) were confirmed: type I DRUJ (55%)—apposing joint surfaces are parallel to the long axis of the radius and ulna; type II DRUJ (33%)—oblique apposing surfaces at the sigmoid and ulnar articular seats; and type III DRUJ (12%)—“reverse oblique” joint orientation with the DRUJ angular apex formed proximal to the DRUJ. In addition, four axial plane anatomical variants of the sigmoid notch were also noted and included flat face (42%), ski slope (14%), C-type (30%), and S-type (14%) notches. Furthermore, an extra-articular palmar osteocartilaginous lip was found in 80% of specimens and was found to serve as a consistent point of attachment for the volar radioulnar ligament and volar DRUJ capsule. When the TFCC is sectioned in the laboratory or incompetent in the clinical setting, this palmar lip serves as a buttress to palmar dislocation of the ulnar head and, thus, acts as a supplemental stabilizer to the interosseous membrane (IOM). This buttress effect is lost when there is a longitudinal tear in the interosseous membrane or fracture of the palmar rim (i.e., sigmoid notch fracture).
The soft tissue anatomy about the DRUJ is well defined,12 and its stabilizers include the pronator quadratus, ulnocarpal ligaments, extensor carpi ulnaris subsheath, dorsal and volar radioulnar ligaments, IOM, and DRUJ capsule. The TFCC is considered the primary stabilizer of the DRUJ, and the IOM is a secondary restraint. The ulnar styloid projects 2 to 6 mm and is the site of attachment for the superficial (distal) limbs of the radioulnar ligaments and the extensor carpi ulnaris subsheath. The deep (proximal) fibers of the distal radioulnar ligaments and the ulnocapitate ligament insert into the fovea at the styloid base. Gofton and colleagues13 found that the radioulnar ligaments and the triangular fibrocartilage maintain DRUJ kinematics with simulated active forearm motion when more proximal soft tissue stabilizers (i.e., pronator quadratus, IOM, extensor carpi ulnaris subsheath, ulnar collateral ligament) are sacrificed. Furthermore, the radioulnar ligaments may play a greater stabilizing role in DRUJ stability in patients with flat sigmoid notches.11
The IOM has multiple biomechanical functions: it helps to transmit force from the radius to the ulna, acts to prevent excessive supination, serves as an aponeurosis for insertions of the deep flexors and extensors, and resists radius and ulna diastasis. The complexity of the IOM structure has been studied by several groups.14–16 In a cadaveric study, Hotchkiss and associates14 defined a central band of ligamentous tissue that contributed 71% of the longitudinal stiffness of the IOM after radial head excision. Injury to this region may represent the pathoanatomy responsible for proximal migration of the radius after radial head excision. Skahen and coworkers16 found that the IOM was consistently organized into a central band, one to five accessory bands, a dorsal proximal interosseous band, and membranous portions. Fibers from the central band originate from the radius and run in a distal-ulnar direction at a 20-degree angle to the long axis of the ulna. Peak strain occurs in the central band during pronation, the assumed position of the forearm when a Galeazzi fracture-dislocation is sustained. Other authors17,18 have demonstrated that the IOM also serves as a coronal (transverse) and sagittal (dorsal-volar) plane stabilizer of the DRUJ, in addition to its described role as a longitudinal restraint. Analyses by Watanabe and colleagues18 suggest that it is a specific injury to the distal portion of the IOM (distal to the central band) that confers increased dorsal-volar instability at the DRUJ throughout a range of forearm rotation when the TFCC and distal radioulnar ligaments are incompetent; when the midportion of the IOM (including the central band) is sectioned together with the distal IOM, the DRUJ becomes unconstrained. Similarly, in a cadaveric biomechanical model, Gofton and coworkers13 demonstrated that the IOM was essential in the maintenance of DRUJ kinematics when distal soft tissue stabilizers are sacrificed (i.e., radioulnar ligaments and triangular fibrocartilage).
True Galeazzi fracture-dislocations have not been reproduced in an ex vivo biomechanical model.19–21 As a result, although these injuries are assumed to occur in definable stages, the failure sequence of the regional soft tissue restraints after fracture of the radius has not been elucidated. However, the contributions of the TFCC and IOM to the biomechanics of the Galeazzi fracture-dislocation have been studied. Moore and associates,20 in a cadaveric model, produced artificial Galeazzi fractures composed of transverse, uncomminuted radial metadiaphyseal fractures created with a Gigli saw at the distal insertion of the pronator teres followed by sequential sectioning of the TFCC and IOM. Moore and associates20 and Schneiderman and coworkers15 independently demonstrated that radial shortening greater than 10 mm required complete disruption of both the TFCC as well as the IOM. Intermediate shortening occurred with isolated sectioning of the TFCC or IOM, respectively. The dorsal carpal retinaculum and ulnar collateral ligaments of the wrist were not found to be significant soft tissue constraints.
Classification
Galeazzi fracture-dislocations are relatively rare injuries, constituting 3% to 7%22 of all forearm fractures. In a retrospective review, Ring and colleagues23 reported that the incidence of isolated radial diaphyseal fractures without DRUJ involvement is greater than that of the true Galeazzi fracture-dislocations. Of the 36 radial shaft fractures, only 9 (25%) occurred in conjunction with DRUJ disruption, whereas 27 (75%) radial diaphyseal fractures occurred in isolation and had no evidence of DRUJ dysfunction at latest follow-up. If both-bone forearm fractures with DRUJ dislocation are included, the incidence is higher. In Mikic’s series of 125 patients with Galeazzi fracture-dislocations,1 20% of cases included fractures of both the radius and ulna.
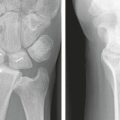
Dameron24 originally subdivided Galeazzi fracture-dislocations into the ulna-volar type (ulna volar to the radiocarpal complex) and the ulna-dorsal type (ulna dorsal to the radiocarpal complex). In a retrospective review of 40 operatively treated Galeazzi fracture-dislocations, Rettig and Raskin8 introduced a classification scheme for these injuries with prognostic value with regard to the probability of intraoperative DRUJ instability after ORIF of the radial shaft fracture. Two patterns of fracture-dislocation were identified based on the distance of the radial shaft fracture from the midarticular surface of the distal radius. In 12 of 22 (55%) type I fractures, occurring within the distal third of the radial shaft and within 7.5 cm of the midarticular surface (Fig. 22-1), operative stabilization of the DRUJ was required with percutaneous Kirschner wire (K-wire) fixation secondary to persistent DRUJ instability after ORIF of the radial shaft fracture. Three of these 12 patients underwent concomitant open repair of the TFCC because the DRUJ was found to be irreducible. In contrast, only 1 of 18 (6%) patients with a type II injury, within the middle third of the radial shaft and more than 7.5 cm from the midarticular surface of the distal radius (Fig. 22-2), required percutaneous fixation of an unstable DRUJ (P < .001).


The mechanism of injury includes a high-velocity direct impact with axial loading of an outstretched arm. Axial loading of the forearm combined with hyperpronation of the forearm is the most common mechanism and causes dorsal dislocation of the DRUJ1; conversely, hypersupination leads to volar dislocation of the ulnar head from the sigmoid notch. We have postulated that for distal radial shaft fractures (type I injuries) within 7.5 cm of the midarticular surface, a high-impact hyperextension mechanism results in a direct continuum of complete injuries through the TFCC and IOM, which predisposes the DRUJ to residual instability and dorsal subluxation despite anatomical radial shaft fracture fixation8 (Fig. 22-3A). With fractures through the middle third of the radial shaft (type II injuries) an indirect pronation force is incurred with incomplete disruption to the regional stabilizing soft tissue structures (see Fig. 22-3B). This may account for the high likelihood of DRUJ and ulnar head stability within the sigmoid notch after fixation of more proximally located radial shaft fractures. However, a significant relationship between the magnitude of initial radial shortening and DRUJ stability was not identified. In a retrospective review of 36 patients with radial shaft fractures treated with plate and screw fixation, Ring and coworkers23 observed a similar trend toward DRUJ stability with proximal and middle third fractures in accord with our findings. In this series, 5 of 8 distal third fractures were associated with DRUJ instability, whereas only 4 of 28 proximal/middle third radius fractures had DRUJ involvement.
Indications and Contraindications
The timing of surgery is dependent on the soft tissue status and clinical condition of the patient. Contraindications to early ORIF include severe, high-grade open fractures with soft tissue loss and gross contamination. Jones25 reported good or excellent results in 66% (12/18) of patients with grade III open forearm fractures treated with a protocol of immediate extensive primary débridement, open reduction and dynamic compression plate fixation, and serial re-débridements at 24- to 48-hour intervals until wound status allowed for soft tissue reconstruction. Duncan and coworkers26 found statistically significant differences in the rate of satisfactory outcomes between grade I, II, and IIIA open forearm fractures and those seen in grade IIIB and IIIC injuries when immediate (<24 hours) ORIF was performed. Patients with grade IIIB and IIIC open forearm fractures may be managed with initial external fixation, serial débridements, and meticulous wound care, followed by delayed internal fixation. Bone grafting should be planned for open fractures with extensive comminution and/or segmental defects at a minimum of 6 weeks from the time a closed soft tissue envelope is obtained. Multisystem trauma or multiple medical comorbidities are clinical scenarios in which early ORIF may also be contraindicated.
Initial Evaluation and Management
Physical examination demonstrates forearm deformity. Prominence of the ulnar head may be present, especially with dorsal DRUJ dislocation, and significant skin tenting may be present. Deforming forces of the radial shaft fracture include the pronator quadratus insertion on the volar surface of the distal fragment, the brachioradialis, and the extrinsic thumb abductor and extensors.4 A thorough neurovascular examination of the upper extremity should be performed and the status of the forearm compartments should be documented. Circumferential inspection of the skin is also performed to identify an open injury. Given the magnitude of energy required to produce this injury, a thorough secondary survey should be performed to rule out any additional musculoskeletal injuries. Prerequisite radiographs include those of the ipsilateral elbow, forearm, and wrist. Radiographic markers of DRUJ disruption are assessed and include fracture through the fovea of the ulnar styloid, DRUJ widening on the anteroposterior view, more than 5 mm of radial shortening, and dorsal subluxation/dislocation of the DRUJ on a true lateral view of the wrist. The importance of radiographic imaging of the ipsilateral elbow and wrist is highlighted by numerous reports of the presence of coincident ipsilateral upper extremity trauma.9,23,27–32 In a series by Ring and coworkers,23 10 of 36 radial diaphyseal fractures were sustained together with ipsilateral upper extremity trauma, including diaphyseal humerus fracture (2), proximal humerus fracture (1), elbow dislocation (1), and scaphoid fracture (1). Strehle and Gerber9 identified additional upper extremity fractures in 21% of their cases. Contralateral wrist radiographs may be obtained if radiographs are equivocal on the injured side. Although advanced imaging modalities are available,33–35 they are rarely obtained preoperatively for true Galeazzi fracture-dislocations. Fester and colleagues36 have recommended the use of both ultrasonography and magnetic resonance imaging when there is clinical suspicion of injury to the IOM because both modalities have impressive testing characteristics (sensitivity, specificity, and positive and negative predictive values).
Surgical Technique
The fracture site is identified and the extent of comminution is evaluated. Fracture site débridement is performed. Manual reduction of the radial shaft fracture is performed, and provisional reduction is maintained with bone reduction clamps. A 3.5-mm AO dynamic compression plate or low-contact dynamic compression plate may be applied to the volar surface and temporarily held with bone reduction clamps. Locked plating techniques may be utilized if there is significant comminution and/or osteoporosis. If the radial shaft fracture is located at the metadiaphyseal junction or within the distal radius metaphysis, consideration may be given to the use of a long volar fixed-angle plate and screw construct. Plate length, anatomical reduction, and restoration of radial length and bow are each evaluated and confirmed with intraoperative fluoroscopy. The chosen implant is then secured to the radial shaft with fully threaded cortical screws and the bone reduction clamps are then removed. Certain fracture patterns may be amendable to supplemental small or mini-fragment cortical lag screws to achieve interfragmentary compression (i.e., butterfly fragments) (Fig. 22-4).

The location and extent of comminution and cortical bone loss are noted on fluoroscopy. Release of the radial septum from the dorsoradial aspect of the radial shaft affords access for bone grafting of the fracture site, often eliminating the need to perform a separate dorsal incision. Cortical fragments devoid of soft tissue attachments should be removed because they represent a potential nidus for infection. Options for bone graft are multiple and include autogenous iliac crest and the ipsilateral distal radius, as well as a host of osteoconductive and/or osteoinductive commercially available products.
After anatomical reduction and fixation of the radial shaft fracture, the DRUJ is evaluated clinically with the forearm in supination for both stability and reducibility. Because it is possible to force the DRUJ into a reduced position despite soft tissue or bone interposition, accurate lateral radiographs without undue force are evaluated. Dorsally directed manual stress is applied to the DRUJ in an attempt to dorsally translate the ulnar head out from the sigmoid notch. If the DRUJ is stable to stress, an above-elbow splint is applied with the forearm in supination (Fig. 22-5). In Galeazzi fracture-dislocations without associated fracture of the ulna styloid, the triangular ligament is disrupted. Cast immobilization in supination allows for reapproximation and healing of the triangular ligament at the site of avulsion to ensure long-term DRUJ stability.

If the ulnar head is unstable but reducible within the sigmoid notch in supination and there is no associated basilar ulnar styloid avulsion fracture fragment, then percutaneous transfixion of the DRUJ is performed. With the forearm in supination and the ulnar head held reduced within the sigmoid notch, two 0.062-inch (1.6 mm) K-wires are percutaneously placed from the ulna through the radius transversely approximately 1 cm proximal to the sigmoid notch to stabilize the DRUJ in supination (Fig. 22-6). The surgeon should be suspicious for and predict residual DRUJ instability after ORIF of the radial shaft fracture in type I injury patterns.8

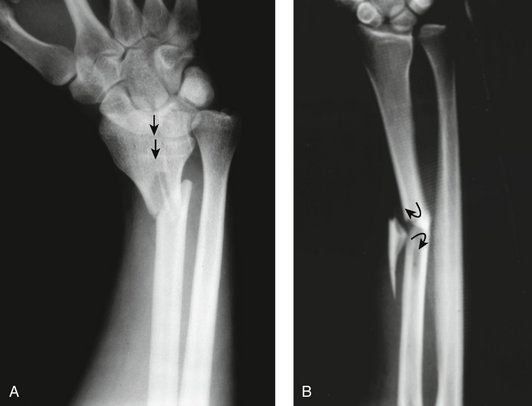
FIGURE 22-6 Posteroanterior (A) and lateral (B) forearm trauma radiographs demonstrate a type I injury pattern with a distal third radial shaft fracture and dorsal dislocation of the ulnar head. C to E, Postoperative radiographs reveal congruent DRUJ reduction after K-wire transfixion, which was required to maintain the ulnar head reduced within the sigmoid notch after radial shaft fracture fixation.
Open reduction of the DRUJ may be necessary if the ulnar head remains unstable and irreducible after reduction and internal fixation of the radial shaft fracture. Soft tissue interposition usually prevents anatomical reduction of the ulnar head into the sigmoid notch. Several regional soft tissue structures have been implicated as blocks to DRUJ reduction in Galeazzi fracture-dislocations. Interposition of the extensor retinaculum, DRUJ capsule, extensor carpi ulnaris, extensor digitorum communis to the ring and little fingers, and the extensor digiti minimi have been separately reported37–43 as causes of an irreducible DRUJ in these complex injuries.
For open reduction of the DRUJ, a dorsal approach to the distal ulna between the fifth and sixth extensor compartments is utilized. The dorsal sensory branch of the ulnar nerve is protected. The extensor retinaculum is elevated from the dorsal DRUJ capsule. A dorsal DRUJ capsulotomy is then completed. However, a traumatic capsulotomy may be present and the ulna head may be buttonholed through the dorsal capsule with dorsal DRUJ dislocations. The DRUJ is inspected for loose bodies and traumatic chondromalacia and then débrided. The TFCC is evaluated. In all three cases of type I injuries requiring open reduction of the DRUJ in our series,8 the triangular fibrocartilage was observed avulsed from its insertion into the base of the ulnar styloid (Palmer class 1B)44 and interposed within the DRUJ. In these cases, the insertion site was prepared for reattachment through drill holes (one patient) or bone suture-anchors (two patients).
Ulnar styloid repair may supplement soft tissue repair/reconstruction and is indicated if a displaced, large ulnar styloid fracture through its base is present. With a displaced ulnar styloid fracture through the fovea, the DRUJ can be unstable as the TFCC is attached to this fragment. Ulnar styloid fractures can be repaired with a 24- or 26-gauge stainless steel figure-of-eight tension band construct or K-wires. Of the nine Galeazzi fracture-dislocations presented by Ring and coworkers,23 four were associated with displaced fractures through the base of the ulna styloid and underwent ORIF of the ulna styloid. Kikuchi and Nakamura45 reported a case of a Galeazzi fracture-dislocation with an irreducible DRUJ secondary to entrapment of an avulsion fracture of the ulna fovea with its preserved attachments to the dorsal portion of the triangular ligament. After reattachment of the foveal fragment to its donor site and K-wire fixation of the ulnar styloid, DRUJ stability was achieved.
Complications
Complications after operative treatment of Galeazzi fracture-dislocations are not uncommon, and several authors have reported a complication rate of 32% to 39%.9,22 Complications include nonunion, malunion, infection, refracture after hardware removal, and persistent DRUJ pain and instability.
Symptomatic post-traumatic DRUJ instability may be due to ligamentous incompetence, bony deformity, or both. Clinical manifestations include pain and limited forearm rotation. The efficacy of conservative management of DRUJ instability with functional bracing is unclear, but bracing has been shown to reduce translational motion at the DRUJ experimentally in a cadaveric study.46 The role of arthroscopic TFCC repair in the setting of chronic DRUJ instability is evolving. In the absence of DRUJ arthritis and significant incongruity, various ligamentous reconstructive procedures of the DRUJ may be considered when the TFCC is irreparable. Ulnar shortening may be considered for symptomatic ulnocarpal impaction and early DRUJ arthritis. Several salvage procedures are available, including the Darrach resection in the low-demand patient, the Sauvé-Kapandji procedure, hemi-resection arthroplasty, and implant arthroplasty. Procedure selection is dependent on individual patient characteristics, radiographic findings, and surgeon preference.
Results of Treatment
With advances in techniques for achieving rigid osteosynthesis and soft tissue reconstruction, ORIF has become the standard of care to optimize outcomes after forearm fractures associated with DRUJ disruption. Although the literature is limited to a relatively small number of retrospective reviews with modest cohort sizes, the data strongly indicate that operative management6–9 yields results superior to those after closed treatment.1,2,4,5
We have previously reported excellent clinical results according to Mikic’s criteria1 in 38 of 40 patients with acute closed Galeazzi fracture-dislocations who were treated with a uniform surgical algorithm.8 Only 2 patients had a poor result, and both had sustained a type I fracture-dislocation. Both subsequently required DRUJ reconstruction at an average of 9 months after the initial injury because of pain and limited supination. At 1-year follow-up, Mohan and associates7 obtained good results in 80% (40/50) of cases treated with ORIF. Two patients subsequently underwent excision of the ulnar head secondary to limited supination and pronation. When anatomical alignment of the radius is achieved and congruent reduction of the DRUJ is maintained, full DRUJ function can be expected.9 Kraus and Horne47 reported a satisfactory outcome according to Hughston’s criteria in 25 of 27 (93%) patients at 32 months postoperatively.
1. Mikic ZD. Galeazzi fracture-dislocations. J Bone Joint Surg Am. 1975;57:1071-1080.
2. Reckling FW, Cordell LD. Unstable fracture-dislocations of the forearm: the Monteggia and Galeazzi lesions. Arch Surg. 1968;96:999-1007.
3. Galeazzi R. Di una particolae sindrome traumatica dello scheletro dell’avambraccio. Atti Mem Soc Lomb Chir. 1934;2:12.
4. Hughston JC. Fracture of the distal radial shaft; mistakes in management. J Bone Joint Surg Am. 1957;39:249-264.
5. Wong PC. Galeazzi fracture-dislocations in Singapore 1960-1964: incidence and results of treatment. Singapore Med J. 1967;8:186-193.
6. Macule Beneyto F, Arandes Renu JM, Ferreres Claramunt A, Ramon Soler R. Treatment of Galeazzi fracture-dislocations. J Trauma. 1994;36:352-355.
7. Mohan K, Gupta AK, Sharma J, et al. Internal fixation in 50 cases of Galeazzi fracture. Acta Orthop Scand. 1988;59:318-320.
8. Rettig ME, Raskin KB. Galeazzi fracture-dislocation: a new treatment-oriented classification. J Hand Surg [Am]. 2001;26:228-235.
9. Strehle J, Gerber C. Distal radioulnar joint function after Galeazzi fracture-dislocations treated by open reduction and internal plate fixation. Clin Orthop Relat Res. 1993;293:240-245.
10. Ekenstam F, Hagert CG. Anatomical studies on the geometry and stability of the distal radioulnar joint. Scand J Plast Reconstr Surg. 1985;19:17-25.
11. Tolat AR, Stanley JK, Trail IA. A cadaveric study of the anatomy and stability of the distal radioulnar joint in the coronal and transverse planes. J Hand Surg [Br]. 1996;21:587-594.
12. Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist—anatomy and function. J Hand Surg [Am]. 1981;6:153-162.
13. Gofton WT, Gordon KD, Dunning CE, et al. Soft-tissue stabilizers of the distal radioulnar joint: an in vitro kinematic study. J Hand Surg [Am]. 2004;29:423-431.
14. Hotchkiss RN, An KN, Sowa DT, et al. An anatomic and mechanical study of the interosseous membrane of the forearm: pathomechanics of proximal migration of the radius. J Hand Surg [Am]. 1989;14:256-261.
15. Schneiderman G, Meldrum RD, Bloebaum RD, et al. The interosseous membrane of the forearm: structure and its role in Galeazzi fractures. J Trauma. 1993;35:879-885.
16. Skahen JR3rd, Palmer AK, Werner FW, Fortino MD. The interosseous membrane of the forearm: anatomy and function. J Hand Surg [Am]. 1997;22:981-985.
17. Pfaeffle HJ, Fischer KJ, Manson TT, et al. Role of the forearm interosseous ligament: is it more than just longitudinal load transfer? J Hand Surg [Am]. 2000;25:683-688.
18. Watanabe H, Berger RA, Berglund LJ, et al. Contribution of the interosseous membrane to distal radioulnar joint constraint. J Hand Surg [Am]. 2005;30:1164-1171.
19. McGinley JC, Hopgood BC, Gaughan JP, et al. Forearm and elbow injury: the influence of rotational position. J Bone Joint Surg Am. 2003;85:2403-2409.
20. Moore TM, Lester DK, Sarmiento A. The stabilizing effect of soft-tissue constraints in artificial Galeazzi fractures. Clin Orthop Relat Res. 1985;194:189-194.
21. Snook GA, Chrisman OD, Wilson TC, Wietsma RD. Subluxation of the distal radioulnar joint by hyperpronation. J Bone Joint Surg Am. 1969;51:1315.
22. Moore TM, Klein JP, Patzakis MJ, Harvey JPJr. Results of compression-plating of closed Galeazzi fractures. J Bone Joint Surg Am. 1985;67:1015-1021.
23. Ring D, Rhim R, Carpenter C, Jupiter JB. Isolated radial shaft fractures are more common than Galeazzi fractures. J Hand Surg [Am]. 2006;31:17-21.
24. Dameron TBJ. Traumatic dislocation of the distal radioulnar joint. Clin Orthop Relat Res. 1972;83:55-63.
25. Jones JA. Immediate internal fixation of high-energy open forearm fractures. J Orthop Trauma. 1991;5:272-279.
26. Duncan R, Geissler W, Freeland AE, Savoie FH. Immediate internal fixation of open fractures of the diaphysis of the forearm. J Orthop Trauma. 1992;6:25-31.
27. Clare DJ, Corley FG, Wirth MA. Ipsilateral combination Monteggia and Galeazzi injuries in an adult patient: a case report. J Orthop Trauma. 2002;16:130-134.
28. Jones TR, Bond CD, Shin AY. Open Galeazzi fracture with concomitant radial head dislocation. Am J Orthop. 2001;30:417-420.
29. Khurana JS, Kattapuran SV, Becker S, Mayo-Smith W. Galeazzi injury with an associated fracture of the radial head. Clin Orthop Relat Res. 1988;234:70-71.
30. Sarup S, Bryant PA. Ipsilateral humeral shaft and Galeazzi fractures with a posterolateral dislocation of the elbow: a variant of the “floating dislocated elbow.”. J Trauma. 1997;43:349-352.
31. Shiboi R, Kobayashi M, Wantanabe Y, Matsushita T. Elbow dislocation combined with ipsilateral Galeazzi fracture. J Orthop Sci. 2005;10:540-542.
32. Stahl S, Freiman S. Simultaneous scaphoid and Galeazzi fractures. Hand Surg. 1999;4:185-188.
33. Failla JM, Jacobson J, van Holsbeeck M. Ultrasound diagnosis and surgical pathology of the torn interosseous membrane in forearm fractures/dislocations. J Hand Surg [Am]. 1999;24:257-266.
34. Matsuoka J, Beppu M, Nakajima H, Aoki H. Ultrasonography for the interosseous membrane of the forearm. Hand Surg. 2003;8:227-235.
35. McGinley JC, Roach N, Hopgood BC, et al. Forearm interosseous membrane trauma: MRI diagnostic criteria and injury patterns. Skeletal Radiol. 2006;35:275-281.
36. Fester EW, Murray PM, Sanders TG, et al. The efficacy of magnetic resonance imaging and ultrasound in detecting disruptions of the forearm interosseous membrane: a cadaver study. J Hand Surg [Am]. 2002;27:418-424.
37. Alexander AH, Lichtman DM. Irreducible distal radioulnar joint occurring in a Galeazzi fracture-case report. J Hand Surg. 1981;6:258-261.
38. Biyani A, Bhan S. Dual extensor tendon entrapment in Galeazzi fracture-dislocation: a case report. J Trauma. 1989;29:1295-1297.
39. Borens O, Chebab EL, Roberts MM, Helfet DL. Bilateral Galeazzi fracture-dislocations. Am J Orthop. 2006;35:369-372.
40. Cetti NE. An unusual cause of blocked reduction of the Galeazzi injury. Injury. 1977;9:59-61.
41. Hanel DP, Scheid DK. Irreducible fracture-dislocation of the distal radioulnar joint secondary to entrapment of the extensor carpi ulnaris tendon. Clin Orthop Relat Res. 1988;234:56-60.
42. Itoh Y, Horiuchi Y, Takahashi M, et al. Extensor tendon involvement in Smith’s and Galeazzi fractures. J Hand Surg [Am]. 1987;12:535-540.
43. Jenkins NH, Mintowt-Czyz WJ, Fairclough JA. Irreducible dislocation of the distal radioulnar joint. Injury. 1987;18:40-43.
44. Palmer AK. Triangular fibrocartilage complex lesions: a classification. J Hand Surg [Am]. 1989;14:594-606.
45. Kikuchi Y, Nakamura T. Irreducible Galeazzi fracture-dislocation due to an avulsion fracture of the fovea of the ulna. J Hand Surg [Br]. 1999;24:379-381.
46. Millard GM, Budoff JE, Paravic V, Noble PC. Functional bracing for distal radioulnar joint instability. J Hand Surg [Am].. 2002;27:972-977.
47. Kraus B, Horne G. Galeazzi fractures. J Trauma. 1985;25:1093-1095.