Hernia most commonly contains loop of Ileum, although can rarely involve other pelvic viscera (i.e., bladder)

 May also be located between superior and middle fasciculi of obturator externus or between internal and external obturator muscles
May also be located between superior and middle fasciculi of obturator externus or between internal and external obturator muscles




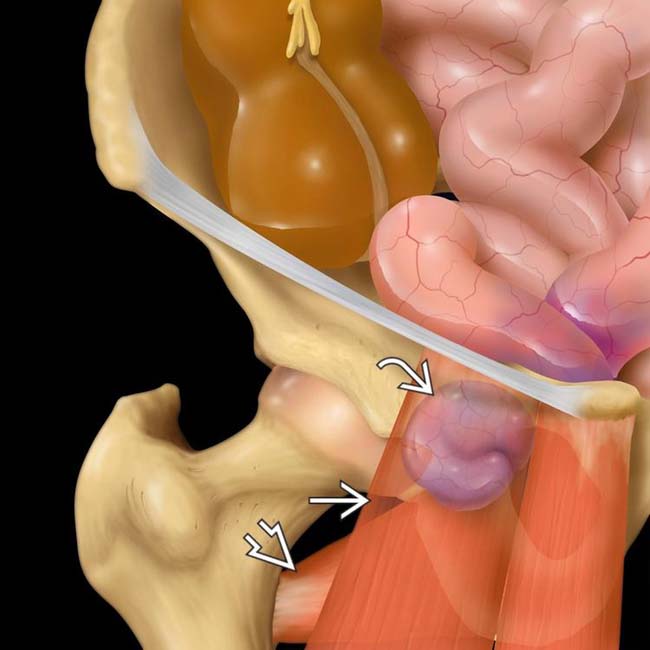
 lies deep to the pectineus muscle
lies deep to the pectineus muscle  and superficial to the obturator externus muscle
and superficial to the obturator externus muscle  .
.
 . Obturator hernias most commonly contain herniated ileum, but other pelvic viscera can also herniate, as in this case.
. Obturator hernias most commonly contain herniated ileum, but other pelvic viscera can also herniate, as in this case.
 and collapsed distal bowel
and collapsed distal bowel  .
.
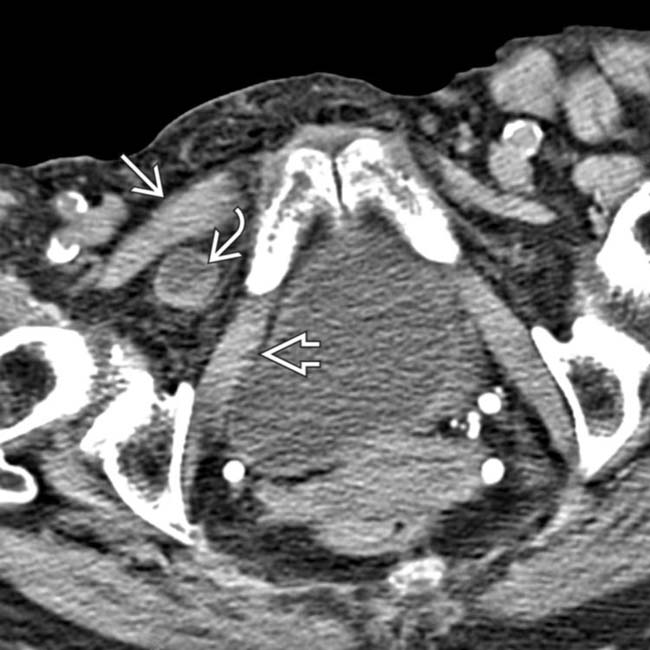
 trapped between the obturator externus
trapped between the obturator externus  and the pectineus
and the pectineus  muscles. These are the classic imaging findings of an obturator hernia.
muscles. These are the classic imaging findings of an obturator hernia.





















 lying between the pectineus
lying between the pectineus  and obturator muscles
and obturator muscles  in a patient with a obturator hernia.
in a patient with a obturator hernia.
 between pectineus and obturator externus muscles.
between pectineus and obturator externus muscles.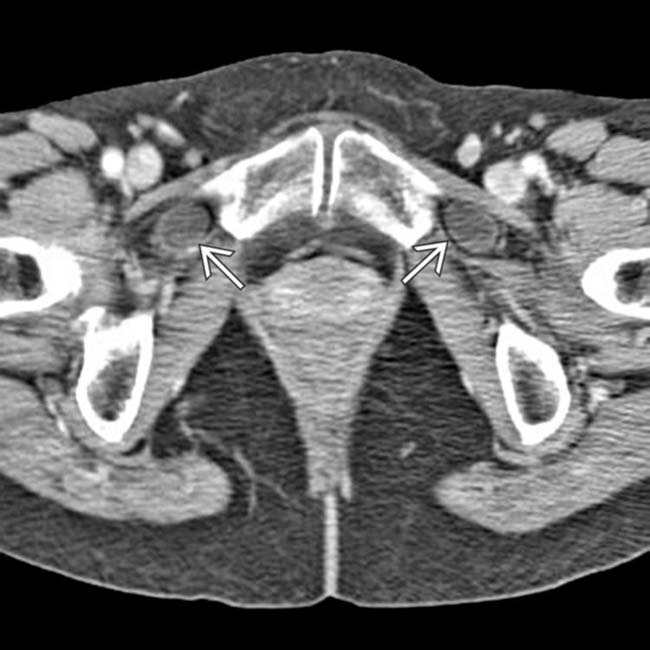
 . Bilateral obturator hernias are rare, accounting for only 6% of all cases.
. Bilateral obturator hernias are rare, accounting for only 6% of all cases.
 entrapped within an obturator hernia.
entrapped within an obturator hernia.
 within the hernia. Only 1 wall of the bowel appears to be trapped.
within the hernia. Only 1 wall of the bowel appears to be trapped.


