Chapter 7
Nuclear Cardiology
1. What is nuclear cardiology?
2. What is myocardial perfusion imaging (MPI)?
3. Define a perfusion defect and differentiate between a reversible and fixed defect.
A perfusion defect is an area of reduced radiotracer uptake in the myocardium.
If the perfusion defect occurs during stress and improves or normalizes during rest, it is termed reversible (Fig. 7-1). Generally, a reversible perfusion defect suggests the presence of ischemia.
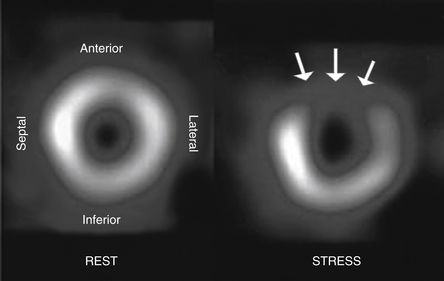
Figure 7-1 Nuclear stress testing short-axis view demonstrating a reversible perfusion defect. Normal myocardial perfusion occurred during resting images (left panel), but a large anterior wall perfusion defect (arrows) was seen during previous stress imaging (right panel). (Modified from Texas Heart Institute Website: Nuclear stress test. Available at http://www.texasheartinstitute.org/HIC/Topics/Diag/dinuc.cfm. Accessed March 22, 2013.)
4. What are the different uses of MPI?
 MPI is used to diagnose coronary artery disease (CAD) in patients with intermediate risk for CAD who present with chest pain or its equivalent.
MPI is used to diagnose coronary artery disease (CAD) in patients with intermediate risk for CAD who present with chest pain or its equivalent.




5. Is MPI the most sensitive and specific test for diagnosing CAD?
6. List the different perfusion agents used in MPI.
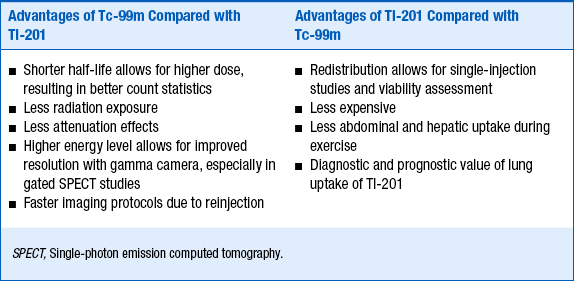
For an agent to be an effective radiopharmaceutical, its distribution has to be proportional to regional blood flow, have a high level of extraction by the organ of interest, and have rapid clearance from the blood. The two most important physiologic factors that affect myocardial uptake of a radiotracer are variations in regional blood flow and the myocardial extraction of the radiotracer. In other words, there will be more uptake of a radiotracer in areas of increased blood flow and less in areas supplied by diseased or stenosed vessels. Importantly, because myocardial extraction is an active process with regard to thallium-201 and a mitochondrial-dependent process with regard to the technetium-99m agents, it can only occur if the cells in that region are viable. The relative advantages and disadvantages of thallium-201 and technitium-99 are summarized in Table 7-1.
 Thallium-201 (Tl-201) is a potassium analog used for MPI. It is the oldest and best studied of the present-day agents. Thallium distribution is dependent on blood flow and tracer extraction by the myocardium. It enters the myocardium by active transport of membrane-bound Na+,K+-ATPase. One of the most important characteristics of Tl-201 is its myocardial redistribution. A dynamic quality to the uptake of Tl-201 gives it the ability to redistribute over time. There is continued influx of Tl-201 over time from the blood-pool activity and a clearance or washout from the myocardium. This phenomenon results in normalization or reversibility in areas that are ischemic, and over additional time, improvement or normalization can occur in areas that are viable but appeared as scar during the first rest imaging.
Thallium-201 (Tl-201) is a potassium analog used for MPI. It is the oldest and best studied of the present-day agents. Thallium distribution is dependent on blood flow and tracer extraction by the myocardium. It enters the myocardium by active transport of membrane-bound Na+,K+-ATPase. One of the most important characteristics of Tl-201 is its myocardial redistribution. A dynamic quality to the uptake of Tl-201 gives it the ability to redistribute over time. There is continued influx of Tl-201 over time from the blood-pool activity and a clearance or washout from the myocardium. This phenomenon results in normalization or reversibility in areas that are ischemic, and over additional time, improvement or normalization can occur in areas that are viable but appeared as scar during the first rest imaging.



 Tc-99m furifosmin is similar to Tc-99m tetrofosmin but is not currently approved for clinical use.
Tc-99m furifosmin is similar to Tc-99m tetrofosmin but is not currently approved for clinical use.

7. How is stress produced for MPI in the evaluation of CAD?
Stress can be produced in different ways. The goal of MPI is to produce vasodilation in order to assess the presence of diseased or stenosed vessels, which will vasodilate to a lesser extent than healthy, non-stenosed vessels. Forms of stress are either exercise or pharmacologic (Table 7-2).
TABLE 7-2
THE STRESS AGENTS USED FOR MYOCARDIAL PERFUSION IMAGING, AND THEIR INDICATIONS, CONTRAINDICATIONS, ADVANTAGES AND DISADVANTAGES
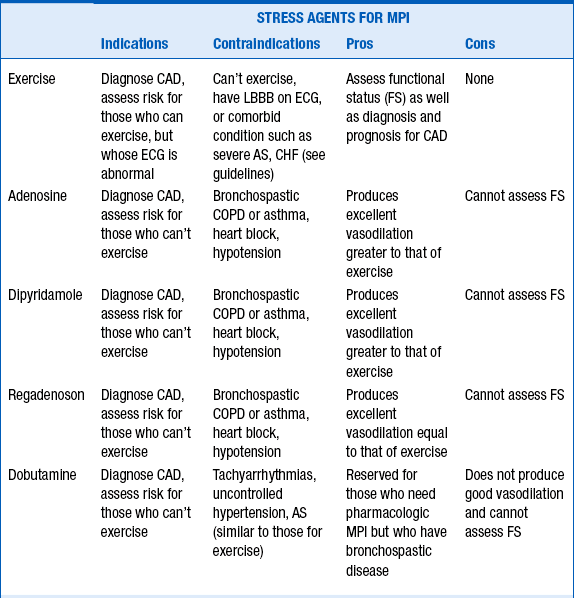
 Exercise can include treadmill, supine or erect bicycle, dynamic arm, or isometric handgrip. In general, because of its diagnostic and prognostic value, the treadmill is used most often. Functional capacity can also be determined during treadmill exercise testing. In addition, prognosis for cardiac events can be determined using the Duke treadmill score when using the Bruce protocol. Exercise increases myocardial blood flow and metabolic demand.
Exercise can include treadmill, supine or erect bicycle, dynamic arm, or isometric handgrip. In general, because of its diagnostic and prognostic value, the treadmill is used most often. Functional capacity can also be determined during treadmill exercise testing. In addition, prognosis for cardiac events can be determined using the Duke treadmill score when using the Bruce protocol. Exercise increases myocardial blood flow and metabolic demand.


8. How much radiation exposure does a patient get from a typical MPI study? How does it compare to other cardiac studies?
It depends on the radiotracer used and the protocol. Exposure can vary from about 10 mSv to upwards of 30 mSv. Table 7-3 summarizes radiation exposure from various tests.
TABLE 7-3
RADIATION EXPOSURE FROM VARIOUS STUDIES
| PA chest film | 0.02 mSv |
| Background radiation | 3 mSv |
| Coronary catheterization | 5 mSv |
| CT angiography | 10-14 mSv |
| CT coronary angiography 64 slice | 17 mSv |
| CT of the body | 20-40 mSv |
| Tc-99m MIBI (10 mCi [rest]/27.5 mCi [stress]) | 14.6 mSv |
| Tl-201 (3.5 mCi) | 29 mSv |
| Calcium scoring | 2.6 mSv |
9. Is it possible to assess both myocardial perfusion and left ventricular (LV) function with one study?
10. Functional assessment of cardiac performance is determined using which nuclear cardiology techniques?
 First-pass radionuclide angiography (FPRNA) uses a bolus technique and rapid acquisition to track the tracer bolus through the right atrium, right ventricle, pulmonary arteries, lungs, left atrium, left ventricle, and finally aorta. The first-pass technique can be used to assess both left and right ventricular ejection fraction, regional wall motion, and cardiopulmonary shunts. FPRNA can be done both at rest and during exercise.
First-pass radionuclide angiography (FPRNA) uses a bolus technique and rapid acquisition to track the tracer bolus through the right atrium, right ventricle, pulmonary arteries, lungs, left atrium, left ventricle, and finally aorta. The first-pass technique can be used to assess both left and right ventricular ejection fraction, regional wall motion, and cardiopulmonary shunts. FPRNA can be done both at rest and during exercise.
 Gated equilibrium blood pool imaging or multiple gated acquisition (MUGA) can also be used to assess left ventricular function and ejection fraction. The right ventricle is not easily assessed with this technique because of overlap of cardiac structures but can be done if care is taken in imaging. The technique is performed after a sample of the patient’s red blood cells is labeled with Tc-99m sodium pertechnetate and then reinjected for planar imaging in three different views. The gating is done similarly to SPECT gating; however, instead of a standard number of frames per cardiac cycle, there can be a variable number, depending on the R-to-R cycle length or heart rate. The cardiac images are then compiled into summed images. They are then processed and displayed as a continuous cinematic loop. From the cinematic loop, one can assess wall motion in the different views, including left anterior oblique (LAO), lateral, and anterior. The data from the LAO view is also displayed as still images so that the counts in the region of interest (the left ventricle) at end-systole and end-diastole can be used to calculate the end-diastolic volume (EDV) and end-systolic volume (ESV) and subsequently the ejection fraction.
Gated equilibrium blood pool imaging or multiple gated acquisition (MUGA) can also be used to assess left ventricular function and ejection fraction. The right ventricle is not easily assessed with this technique because of overlap of cardiac structures but can be done if care is taken in imaging. The technique is performed after a sample of the patient’s red blood cells is labeled with Tc-99m sodium pertechnetate and then reinjected for planar imaging in three different views. The gating is done similarly to SPECT gating; however, instead of a standard number of frames per cardiac cycle, there can be a variable number, depending on the R-to-R cycle length or heart rate. The cardiac images are then compiled into summed images. They are then processed and displayed as a continuous cinematic loop. From the cinematic loop, one can assess wall motion in the different views, including left anterior oblique (LAO), lateral, and anterior. The data from the LAO view is also displayed as still images so that the counts in the region of interest (the left ventricle) at end-systole and end-diastole can be used to calculate the end-diastolic volume (EDV) and end-systolic volume (ESV) and subsequently the ejection fraction.

11. Why should one use radionuclide angiography to assess LVEF?
 It is a precise and accurate measure of LVEF that is more reproducible than standard two- dimensional echocardiography, especially when doing serial studies to look for changes in LVEF caused by cardiotoxic agents, valvular heart disease, and new therapeutic agents in clinical trials.
It is a precise and accurate measure of LVEF that is more reproducible than standard two- dimensional echocardiography, especially when doing serial studies to look for changes in LVEF caused by cardiotoxic agents, valvular heart disease, and new therapeutic agents in clinical trials.
 It is less expensive and more feasible than magnetic resonance imaging for evaluation of LVEF.
It is less expensive and more feasible than magnetic resonance imaging for evaluation of LVEF.


Bibliography, Suggested Readings, and Websites
1. Baghdasarian, S.B., Heller, G.V. The role of myocardial perfusion imaging in the diagnosis of patients with coronary artery disease: developments over the past year. Curr Opin Cardiol. 2005;20:369–374.
2. Berman, D.S., Shaw, L.J., Hachamovitch, R., et al. Comparative use of radionuclide stress testing, coronary artery calcium scanning, and noninvasive coronary angiography for diagnostic and prognostic cardiac assessment. Semin Nucl Med. 2007;37:2–16.
3. Bourque, J.M., Velasquez, E.J., Tuttle, R.J., et al. Mortality risk associated with ejection fraction differs across resting nuclear perfusion findings. J Nucl Cardiol. 2007;14:165–173.
4. Brindis, R.G., Douglas, P.S., Hendel, R.C., et al. ACCF/ASNC appropriateness criteria for single-photon emission computed tomography myocardial perfusion imaging (SPECT MPI). J Am Cardiol. 2005;51:1127–1147.
5. Hachamovitch, R., Berman, D.S. The use of nuclear cardiology in clinical decision making. Semin Nucl Med. 2005;35:62–72.
6. Hachamovitch, R., Hayes, S.W., Friedman, J.D., et al. Comparison of the short-term survival benefit associated with revascularization compared with medical therapy in patients with no prior coronary artery disease undergoing stress myocardial perfusion single photon emission computed tomography. Circulation. 2003;107:2900–2906.
7. Iskanderian, A.E., Verani, M.S. Nuclear cardiac imaging principles and applications, ed 3. New York: Oxford University Press; 2003.
8. Klocke, F.J., Baird, M.G., Bateman, T.M., et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging. J Am Cardiol. 2003;42:1318–1333.
9. Metz, L.D., Beattie, M., Hom, R., et al. The prognostic value of normal exercise myocardial perfusion imaging and exercise echocardiography. J Am Coll Cardiol. 2007;49:227–237.
10. Miller, T.D., Redberg, R.F., Wackers, F.J.T. Screening asymptomatic diabetic patients for coronary artery disease, why not. J Am Coll Cardiol. 2006;48:761–764.
11. Shaw, L.J., Berman, D.S., Maron, D.J., et al. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117:1283–1291.
12. Travin, M.I., Bergman, S.R. Assessment of myocardial viability. Semin Nucl Med. 2005;35:2–16.


